Article Text

Abstract
Background Patients with traumatic wounds frequently present to the ED. Literature on whether to treat these wounds sterile or non-sterile is sparse. Non-sterile treatment has the advantage of saving resources and costs, and could be of value in health settings where sterile materials are not readily available. Our objective was to compare the rate of wound infection after suturing traumatic lacerations with non-sterile gloves and dressings versus sterile gloves, dressings and drapes in the ED. We hypothesised that non-sterile gloves and dressings would be non-inferior to sterile gloves, dressings and drapes. The non-inferiority margin was set at 2%.
Methods A multicentre single-blinded randomised controlled trial testing for non-inferiority of non-sterile gloves and dressings versus sterile gloves, dressings and drapes for suturing of traumatic wounds was performed in 3 EDs in The Netherlands. Adults with uncomplicated wounds were included from July 2012 to December 2016. At the time of treatment, patient and wound characteristics and management were documented. The outcome was wound infection, which was identified during follow-up in the treating ED at 5–14 days postprocedure.
Results From 2468 eligible patients, 1480 were randomised in a sterile (n=747) or non-sterile (n=733) protocol. Baseline characteristics were similar in both study arms. The observed wound infection rate in the non-sterile group was 5.7% (95% CI 4.0% to 7.5%) vs 6.8% (95% CI 5.1% to 8.8%) in the sterile group. The mean difference of the wound infection rate of the two groups was −1.1% (95% CI −3.7% to 1.5%).
Conclusion Although recruitment ceased prior to reaching our planned sample size, the findings suggest that there is unlikely to be a large difference between the non-sterile gloves and dressings for suturing of traumatic wounds and sterile gloves, dressings and drapes for suturing of traumatic wounds in the ED.
Trial registration number NL 34798.078.11, NTR3541.
- emergency department
- wounds and injuries
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
What is known on this topic
There are few studies evaluating whether the use of sterile versus non-sterile materials (gloves, dressings and drapes) makes a difference in the development of wound infection in lacerations presenting to the ED.
One single centre study found no difference in infection rates in sterile versus non-sterile glove use in traumatic wound repair.
What does this paper add
A large multicentre, non-inferiority, randomised trial, involving 1480 patients, showing that the infection rate in patients treated with non-sterile gloves and dressings was similar to that of patients where sterile gloves, dressings and sterile drapes were used.
How might this study affect research, practice or policy
Although underpowered, the data in this study suggest it to be unlikely that there is a large difference in wound infection rates between the sterile and non-sterile group.
Introduction
Patients with traumatic wounds frequently present to the ED. These wounds arise in non-sterile skin, in a non-sterile environment and are caused by non-sterile objects. Such wounds may therefore be considered to be contaminated in contrast to surgical wounds where the skin is disinfected before this protective barrier is cut with a sterile object.1 Non-sterile treatment has the advantage of saving resources and costs, and could be of value in health settings where sterile materials are not readily available. Studies on the treatment of traumatic wounds and whether the use of sterile versus non-sterile materials, such as gloves, dressings and drapes, affects wound infection are sparse and conflicting.2 3 A systematic review and meta-analysis pooling data on Mohs surgery, laceration repair, standard cutaneous excisions and tooth extractions using non-sterile versus sterile gloves found no difference in infection rates.4 One single-centre study in an ED, with a relatively small sample size, showed no difference in infection rates between sterile versus non-sterile glove use in traumatic wound repair.5 This result has not been validated in a different population. Therefore, we conducted a multicentre non-inferiority trial that aimed to compare the effect of non-sterile and sterile suturing of traumatic wounds in the ED on wound infection. Our hypothesis was that a non-sterile suturing method would be non-inferior to a sterile suturing method.
Method
Study design and setting
This study is designed as a multicentre, single-blinded, randomised controlled trial testing for non-inferiority of non-sterile gloves and dressings versus sterile gloves, dressings and drapes for suturing of traumatic wounds. This manuscript is reported as per the Consolidated Standards of Reporting Trials statement.
Patients were included in this study from 25 July 2012 until 31 December 2016 when presenting with a traumatic wound to one of three participating hospitals in The Netherlands: one university medical centre and two regional hospitals.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination of plans of this study.
Selection of participants
Patients were eligible for inclusion when presenting to the ED with a traumatic wound for which sutures were required and were at least 18 years of age. Exclusion criteria were met if the traumatic wound was complicated (accompanied by bone, vascular, tendon, nerve or cartilage injury), due to a human or animal bite, needed direct intervention in the operating room, already infected at presentation or when the wound was >24 hours old. Patients eligible for inclusion were informed by a nurse or physician and given a patient information brochure providing more detailed background information on the proposed study.
Randomisation
Patients who met the inclusion criteria and agreed to participate were consecutively included and randomised to a sterile or non-sterile protocol and treated accordingly. A simple 1:1 randomisation was used without any stratification factors. Randomisation occurred using an internet-based electronic randomisation programme (Alea Data Management) by the treating physician.
Interventions
Following randomisation, preparation of the wound was undertaken by the nurse. Irrespective of the assigned study arm, this included removal of large contamination and rinsing thoroughly with tap water. After wound preparation, a physician working in the ED treated the wound according to the designated protocol. Materials used in both protocols included: chlorhexidine for disinfection, lidocaine 1% for infiltration anaesthesia, sterile sutures (Ethilon nylon suture size 3.0 up to 6.0 and Vicryl 3.0 up to 5.0) and sterile instruments. The study procedures differed between groups in the use of sterile versus non-sterile dressings and gauzes, sterile surgical gloves versus non-sterile boxed gloves and the use of sterile (fenestrated) drapes in the sterile protocol only. The use of masks, gowns, caps and shoe coverings is not common practice and were not used in either protocol.
Measurements
The patients’ baseline characteristics, wound characteristics, wound care at the ED and time interval between the injury and treatment were recorded by the treating physician on a research form. After wound treatment, verbal and written instructions were given on wound care and signs of wound infection. Patients were instructed to immediately return to the ED in case of a suspected infection or if they had any concerns regarding the wound. All agreed to return to the ED for wound inspection and removal of sutures; the time interval for follow-up was between 5 and 14 days depending on wound location and according to the wound care protocol of the treating hospital.
During follow-up, an attending emergency physician blinded to treatment allocation recorded the presence and degree of cellulitis, wound dehiscence, purulent discharge, abscess formation or signs of systemic infection. Additionally, information was recorded concerning the time interval between suturing and suture removal, if and why the patient returned prematurely for wound inspection, whether the patient had visited another physician and if they had received antibiotics for their wound or any other reason.
Standard actions in wound care were undertaken if an infection was diagnosed including opening and flushing the wound, antibiotic prescription, referral for hospital admission or surgical intervention.
In case of hospital admission or other reasons hindering ED follow-up, medical records were assessed by an investigator blinded for treatment protocol, and the necessary information regarding aspects of the wound at time of suture removal was collected. If information was missing from the medical records, attempts were made to complete the follow-up information by contacting patients by telephone. Patients were asked about signs of infection and if they received any wound-related treatment by another physician as per hospital follow-up. On the basis of the retrieved information, a wound was categorised as infected or not infected.
Outcomes
The primary outcome was wound infection.
A wound was considered infected if, during the time interval between wound treatment and follow-up, there was an abscess originating from the wound, cellulitis >10 mm, purulent fluid, wound dehiscence was seen and/or the physician found wound treatment to be necessary at follow-up, for example, prescription of antibiotics or opening and flushing the wound.
Analysis
A dedicated researcher collected and entered all treatment and follow-up data in a database.
Descriptive statistics were reported to compare baseline characteristics of the sterile versus the non-sterile study arm. Of the categorical data, frequencies were calculated and differences between both intervention groups were tested with a χ2 test or Fisher’s exact test if one or more of cells had an expected frequency of five or less. Infection rates were presented as percentages with 95% CI. The data were analysed using IBM SPSS V.25 (Statistical Product and Service Solutions, Chicago, Illinois, USA).
The expected infection rate in the sterile suture group was estimated at 3.5%, based on previous infection rates in the literature of 2.5%–7% vs 5.5% in the non-sterile group.1 5–7 The non-inferiority margin was set at 2% so that an infection percentage difference of ≥2% or more in the non-sterile group in comparison to the sterile group would be considered inferior to the use of sterile materials in clinical practice. To reach a power of 80% at a significance level of 0.05 for two-sided testing, 2140 patients needed to be included the study (1070 patients per study arm). We defined non-inferiority as the upper bound of the two-sided 95% CI not exceeding 2%.
Results
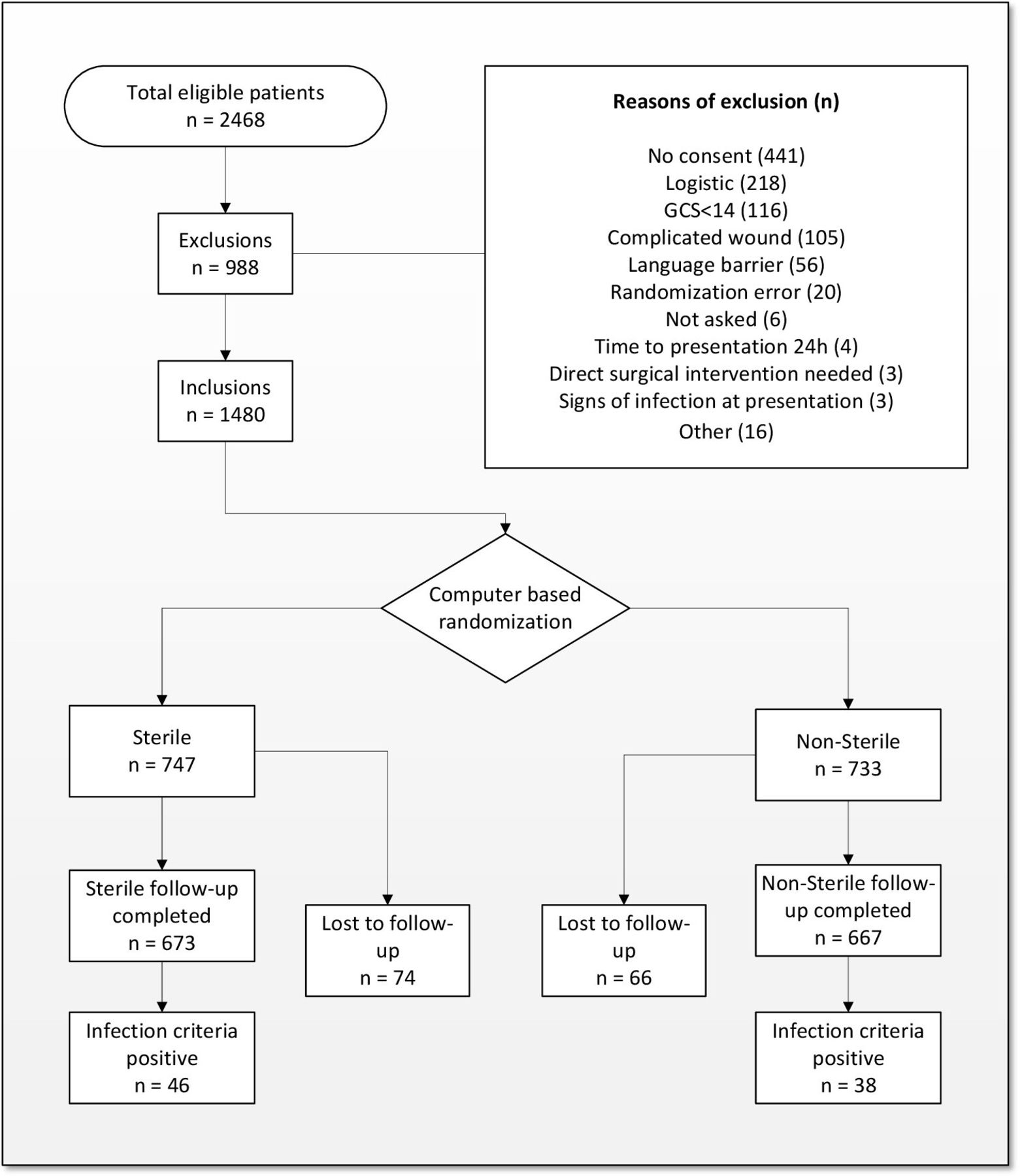
A total of 2468 patients were eligible for participation during the study period. Out of these patients, 968 were excluded and 20 were not included due to technical problems with the electronic randomisation programme. The main reasons for exclusion were no consent (n=437) and unable to come back to hospital for follow-up due to logistical reasons (n=218) (figure 1).
{kind=link}
Flow chart of eligible patients.
A total of 1480 patients were randomised in the sterile (n=747) or non-sterile (n=733) study group when we discontinued the study early because of decline in patient inclusions, which was due to the integration of general practitioner practices in the EDs. There were no differences in the baseline characteristics (table 1). In the sterile arm 74 patients were lost to follow-up vs 66 in the non-sterile arm.
Baseline characteristics of study patients
The mean age in the sterile versus non-sterile group was 39.2 and 39.5 years (table 1). Most patients were male (sterile group: 74.2%; non-sterile group: 73.0%). The use of oral antidiabetics, insulin and corticosteroids was low in both study groups. Although overall numbers are low, significantly more people were using immunosuppressant drugs in the non-sterile group. There were no differences in baseline wound characteristics or in characteristics of received treatment (tables 2 and 3).
Baseline characteristics of wounds
Baseline characteristics of wound treatment
Follow-up information was obtained for 91% of participants. Almost all of those patients (93%) returned to the ED for follow-up. The information of the patients who we were unable to return to ED (7%) was retrieved by telephone. There was no difference in characteristics of patients who were followed-up by telephone, in ED or were lost to follow-up in the two study arms.
Main results
The wound infection rate in the sterile treatment group was 6.8% (95% CI 4.0% to 7.5%) vs 5.7% (95% CI 5.1% to 8.8%) in the non-sterile treatment group. The mean difference of the wound infection rate of the two groups was −1.1% (95% CI −3.7% to 1.5%). In comparing characteristics in patients with or without wound infection, more infected wounds were located on the lower extremity (20.2% vs 12.2%) and patients were more likely to be using immunosuppressants (6% vs 1.5%) (online supplemental table 1).
Supplemental material
Out of 1340 inclusions with follow-up, 2 patients in the sterile group and 1 in the non-sterile group required admission and intravenous antibiotics.
Discussion
In this large multicentre randomised controlled trial, the upper bound of the 95% CI was lower than the prespecified non-inferiority margin and so it is likely that non-sterile gloves and dressings are non-inferior to their sterile counterparts. However, as the study stopped early and was underpowered, this finding should be interpreted cautiously. Nevertheless, we did not find any evidence that sterile gloves, gowns and drapes are associated with development of wound infection after suturing of traumatic wounds in the ED.
The wound infection rate was higher than expected in both study arms when comparing with previous literature.1 5–7 One reason could be that there is no consensus in the literature on the definition of wound infection. The boundaries between normal wound healing, inflammation and actual infection seem hard to discern and various criteria are used throughout the literature to define wound infection.1–17 Although almost all study patients (93%) were followed up in the treating ED, interclinician variety in wound judgement could have contributed to the higher overall incidence of infection in this study. Furthermore, in The Netherlands, primary care is easily accessible and more EDs are integrating primary care practices. Because of this, it may be that in this study, the simpler smaller wounds that could easily be managed by a general practitioner were filtered out and the study group consists of more complex wounds with a higher risk of infection.
In 2004, Perelman et al published a randomised controlled trial on the use of sterile versus non-sterile gloves for suturing of traumatic wounds in the ED.5 They found infection rates similar to those found in this study without a significant difference between the study groups. This study supports their results using protocols that reflect current common practice, using either non-sterile gloves and dressings or sterile gloves, dressings and drapes and in a larger sample reflecting the whole ED population. Also, the majority of patients in this study were followed up in the ED and only a small part of the study population received a follow-up by telephone, which makes it less prone to misclassification of outcome.
Patients with a chronic illness (eg, diabetes) or that use medication that might negatively influence wound healing (eg, corticosteroids) were not excluded from this study to reflect a more representative ED population.
Using sterile technique in the ED, the physician is more likely to require an assistant. Sterile gloves, dressings and drapes can expire and are not readily available in all treatment rooms in the ED. Therefore, non-sterile suturing in an ED setting will be more convenient and likely save time. Further research should be done to demonstrate cost-effectiveness of the non-sterile suturing technique.
On the other hand, while untested, the sterile suturing technique may provide reassurance for the patient which may also be of value, even if the non-sterile technique confers no greater risk of infection.
This study was limited by not meeting the intended statistical power. A little over two-thirds of the number of patients weres included during our study period. This was mainly due to primary care practice integration into EDs in The Netherlands during our study period. A shared triage system directs patients either to the ED or to a general practitioner, resulting in a large fall in number of traumatic wound presentations to EDs. After the implementation of the primary care practices, it was no longer feasible to reach the targeted inclusion number. This resulted in the decision to terminate our trial. The decision to terminate the trial early was taken by researchers that were blinded to treatment allocation and outcome data. No interim analyses were undertaken before the trial was stopped.
Furthermore, we did not test the role of other elements of sterile technique such as hand scrubbing, masks, caps, gowns and shoe covers. The use of masks, hand scrubbing, caps, gowns and shoe covers is not common practice in the ED. To be able to translate our results to daily practice, we decided to compare common practice: sterile gloves, dressings and drapes to a non-sterile technique with clean gloves, clean dressings.
In conclusion, this trial suggests that there is unlikely to be a large difference between the non-sterile gloves and dressings for suturing of traumatic wounds and sterile gloves, dressings and drapes for suturing of traumatic wounds in the ED.
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the medical research ethics committee of University Medical Center Rotterdam (Trial Number: NL 34798.078.11) and registered in the Netherlands Trial Registry (Trial Number: NTR3541). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor David Metcalfe
JJMZ and WR contributed equally.
Contributors JJMZ: initiation and design of the study, writing of the protocol and the manuscript. Contributed to supervised data collection and analysis. WR: supervised data collection of all participating centres. Contributed to initiation and design of the study, analysis of the data and to the writing, critical revision and final approval of the manuscript. AVR: contributed to initiation of the study and supervised data collection in SFVG and revision of the manuscript. EMMvL: contributed to the study design, data analysis and critical revision and final approval of the manuscript. GVW: contributed to initiation of the study and supervised data collection in HMC and revision of the manuscript. PP: contributed to the design of the study, supervised the conduction of the study and the critical revision and final approval of the manuscript. JAH: contributed to analysis of the data and writing, critical revision and final approval of the manuscript. PPMR: contributed to the initiation and design of the study, writing and revision of the protocol, supervised data collection and analysis and to the writing, critical revision and final approval of the manuscript. PPMR is acting as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.