Article Text

Abstract
Background Patients experiencing early pregnancy loss often first present to the emergency department (ED) where they can be managed non-operatively through expectant or medical management, or surgically by the obstetrical team. Studies have reported that physician gender can influence clinical decision making, but there is limited research on this phenomenon in the ED. The objective of this study was to determine whether emergency physician gender is associated with early pregnancy loss management.
Methods Data were retrospectively collected from patients who presented to Calgary EDs with a non-viable pregnancy from 2014 to 2019. Pregnancies >12 weeks gestational age were excluded. The emergency physicians included saw at least 15 cases of pregnancy loss over the study period. The primary outcome was obstetrical consult rates by male versus female emergency physicians. Secondary outcomes included rates of initial surgical evacuation via dilation and curettage (D&C) procedures, ED returns, returns to care for D&Cs and total D&C rates. Data were analysed using χ2, Fisher’s exact and Mann-Whitney U tests, as appropriate. Multivariable logistic regression models accounted for physician age, years of practice, training programme and type of pregnancy loss.
Results 98 emergency physicians and 2630 patients from 4 ED sites were included. 76.5% of the physicians were male accounting for 80.4% of pregnancy loss patients. Patients seen by female physicians were more likely to receive an obstetrical consultation (adjusted OR (aOR) 1.50, 95% CI 1.22 to 1.83) and initial surgical management (aOR 1.35, 95% CI 1.08 to 1.69). ED return rates and total D&C rates were not associated with physician gender.
Conclusion Patients seen by female emergency physicians had higher rates of obstetrical consultation and initial operative management compared with those seen by male emergency physicians, but outcomes were similar. Additional research is required to determine why these gender differences exist and how these discrepancies may impact the care of early pregnancy loss patients.
- obstetrics
- gynecology
- clinical care
- management
Data availability statement
No data are available.
Statistics from Altmetric.com
What is already known on this topic
Patients experiencing pregnancy loss frequently express disappointment with the care they receive in the ED.
The purpose of this study was to explore how emergency physician gender may be associated with this care.
What this study adds
This study highlights how pregnancy loss patients seen by female emergency physicians were more likely to receive obstetrical consults and initial operative management; however, ED return rates and total operative management rates within 7 days were similar.
How this study might affect research, practice or policy
We hope this study sets the stage for future qualitative research into why these gender-based differences exist and whether they influence patient satisfaction and outcomes.
Introduction
Pregnancy loss, also known as a miscarriage or spontaneous abortion, is common, affecting up to one in five pregnancies.1 Over 70% of patients experiencing pregnancy loss present to the emergency department (ED)2 with symptoms such as vaginal bleeding and/or abdominal pain.3 In the ED, pregnancy loss can be managed non-operatively through expectant or medical management.4 5 Alternatively, emergency physicians can refer these patients to the obstetrical team for surgical evacuation of the fetal tissue, most often through dilation and curettage (D&C).5 While surgical management was previously the standard of care, there has been a recent shift towards non-operative management due to its comparable rates of success, limited complications and preference by patients.6–8 However, patients experiencing pregnancy loss are often disappointed with the care they receive in the ED, citing a lack of emotional support and poor communication by staff.3 9 Patients experience considerable distress and grief following a loss of pregnancy,10 and thus it is pertinent to explore the variables contributing to these deficits in care, and how emergency physicians can improve these patients’ outcomes.
Evidence suggests that male and female physicians differ in the medical care they provide, which can impact patient care.11–16 Female physicians are more likely to have a patient-centred communication style,17 18 more frequently consult specialists,19 20 discuss preventative medicine21 and follow clinical guidelines,22 which often results in greater patient satisfaction.17 21 Studies have also reported that female surgeons and internists have lower rates of patient mortality and complications compared with their male colleagues.23 24 Despite these established differences, there is limited evidence on how patient management and outcomes differ as a result of emergency physician gender.
The goal of this study was to determine how emergency physician gender impacts the care of ED patients experiencing early pregnancy loss. Our primary outcome was rates of obstetrical consults for early pregnancy loss across emergency physician gender. Secondary outcomes included rates of operative management via D&C, ED returns, returns to care for D&C and total D&C rates. We hypothesised that because female physicians have a more patient-centred communication style17 18 and more frequently consult specialists,19 20 they would be more likely to consult their obstetrical colleagues.
Methods
Study design and setting
This was a retrospective cohort study of patients who presented to one of four Calgary EDs with non-viable pregnancy loss from 1 January 2014 to 31 December 2019. This 6-year time frame was chosen based on our prior clinical knowledge of the included sites and their corresponding patient volumes, informed additionally by administrative data. Based on this proposed timeframe, the sample size collected was deemed sufficient for our data analyses. An a priori sample size estimate was not completed. The reporting of this study conforms to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.25 Due to ethical concerns, individual patient data cannot be made publicly available for data sharing.
Participants
The four ED sites included in this study are high volume, with yearly ED visit numbers ranging from 71 040 to 82 789 in 2020.26 The model for Calgary EDs is that patients with known pregnancies ≥12 weeks gestational age are sent directly to the labour and delivery unit rather than being assessed in the ED. Therefore, the majority of ED patients included in this study would have been experiencing early pregnancy loss <12 weeks gestational age. Given the multitude of ways in which gestational age can be calculated (ie, ultrasound dating, last menstrual period, etc) and the inaccuracy of some of these markers in early pregnancy,27 gestational age was not available for all patients and therefore not able to be included in this study. However, human chorionic gonadotropin (HCG) is frequently used as a biomarker to assess for miscarriage or early pregnancy viability and is a marker for retained tissue in the uterus.27–29 Therefore, HCG was used as a proxy for gestational age and retained uterine tissue in this study cohort.
Patients coded with International Classification of Disease Tenth Edition (ICD-10) codes O03.4 (incomplete spontaneous abortion without complication) or O02.1 (missed abortion) were included. ‘Incomplete spontaneous abortion’ occurs when some, but not all, products of conception have been expelled.30 ‘Missed abortion’ is defined as fetal demise in the absence of uterine activity.30 Patients with multiple diagnoses on ED presentation, missing patient identification numbers, a Canadian Triage and Acuity Scale (CTAS) code of 1 (required resuscitation) or a complex admission status (not classified as admitted or discharged) were excluded. Multiple diagnoses were used as a proxy for complications. Patient identification numbers were required to confirm a unique patient visit. Patients with a complex admission status included those who left against medical advice or left without being seen.
The included emergency physicians saw at least 15 cases of pregnancy loss between 2014 and 2019. The goal of this minimum case requirement was to include physicians who had reasonable exposure to pregnancy loss and to establish a relatively homogenous case-mix sample of patients.
Variables and outcomes
Patient data were collected from Sunrise Clinical Manager (SCM), an electronic medical record system used across Calgary EDs. Patient variables including identification numbers, age, gender, haemoglobin (Hb), HCG, CTAS code, triage-to-physician assessment time, inpatient length of stay, obstetrical consults, D&C procedures and ED returns were collected. Some patients did not have Hb and/or HCG levels listed in SCM, reflected as different sample sizes in table 1. Physician data were collected from the Calgary Emergency Medicine administrative database, which links physician data from multiple systems for research and performance reporting. Physician identification numbers, age, gender, years of practice and training programme were collected. The breakdown of Calgary emergency physicians by gender and number of shifts was collected from this administrative database. All other patient and physician identifiers were removed prior to analysis for confidentiality. Data collection and statistical analyses were completed by separate individuals to minimise risk of confidentiality and bias.
Variables across emergency physician gender
Physician demographics
The primary outcome was the association between emergency physician gender and obstetrical consultation. Secondary outcomes included initial rates of D&Cs, ED returns, returns to care for D&C and total D&C rates. ED returns and returns for D&C were included if they occurred within 7 days of initial ED visit. All ED returns within 7 days were included, irrespective of chief complaint. Returns for D&C were included if they occurred at (a) one of the four major Calgary hospitals or (b) an ambulatory day surgery clinic in Calgary. Returns for D&C were used as a proxy for failed non-operative management.
Statistical methods
Associations between categorical variables were assessed using χ2 test or Fisher’s exact test, as appropriate. Associations between physician gender and continuous variables were assessed using Mann-Whitney U tests. Univariate and multivariable logistic regression models were employed to assess associations between physician gender and the primary and secondary outcomes. Any variables which were found to be significantly different across physician gender (p<0.05), were controlled for in our multivariable logistic regression models. Analyses were conducted using IBM SPSS Statistics for Windows, V.26.0 (IBM, Armonk, New York, USA).
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
Participants
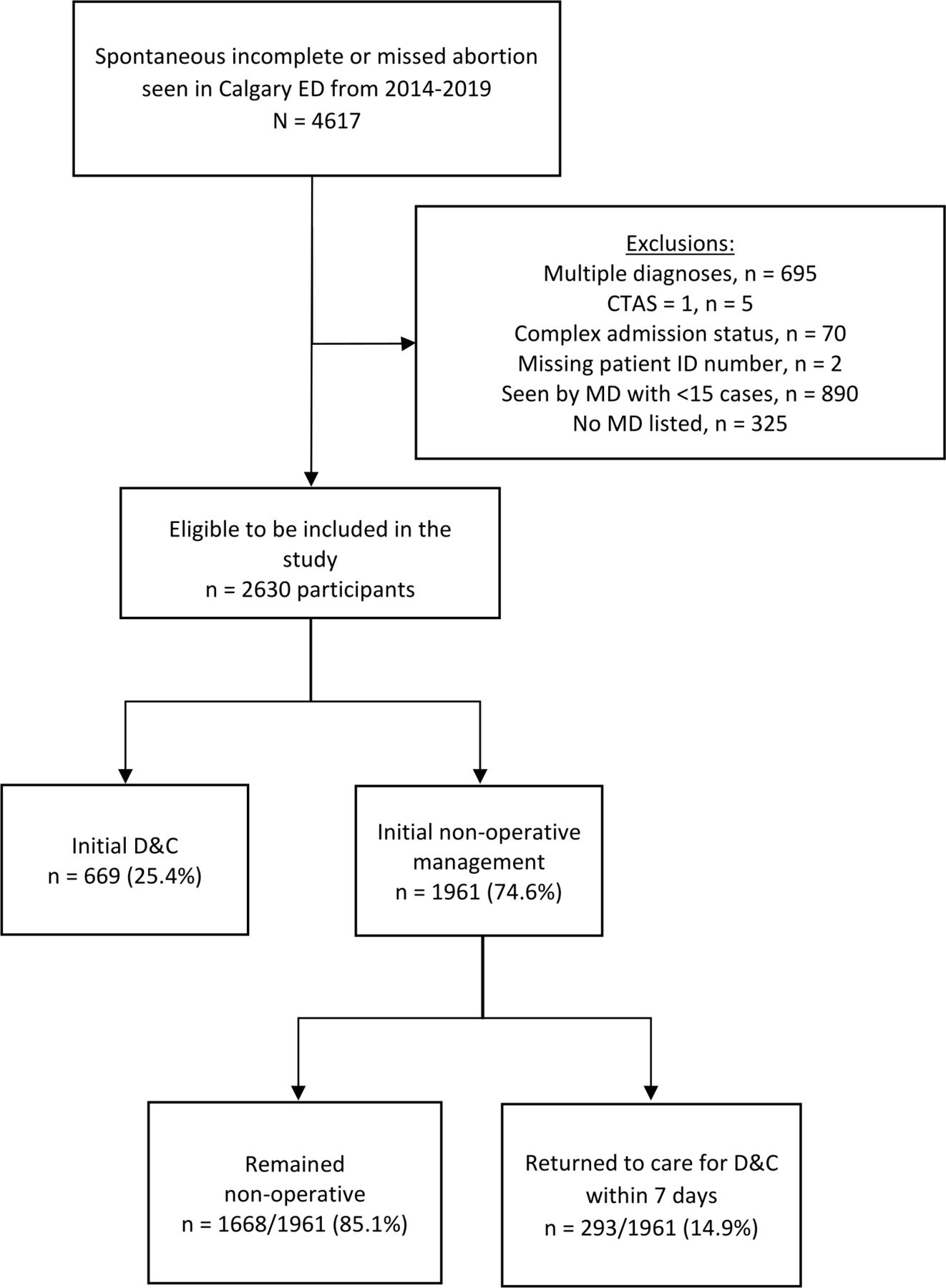
From 2014 to 2019, 4617 patients presented to one of four Calgary EDs with an incomplete spontaneous abortion without complication (ICD-10 code O03.4) or a missed abortion (ICD-10 code O02.1). After excluding patients who were ineligible (figure 1), 2630 patients were included in this study. Ninety-eight emergency physicians accounted for these 2630 patients, 75 (76.5%) of which identified as male physicians (table 2). Of the 98 included physicians, the mean age was 49.4±9.1 years and the mean duration of practice was 15.4±8.7 years. Fifty-six (57.1%) physicians completed their training through the Canadian College of Family Physicians-Emergency Medicine (CCFP-EM) programme and the remaining 42 (42.9%) physicians trained through the Fellow of the Royal College of Physicians of Canada programme. The median number of cases for all the included physicians was 22, with female physicians seeing a median of 20 cases and males seeing a median of 23 cases over the 6-year study period. Based on administrative data, approximately 70% of Calgary emergency physicians from 2014 to 2019 were male and they accounted for 74% of emergency shifts at the four ED sites (data not shown).
{kind=link}
Flow diagram of study cohort. ED, emergency department; MD, medical doctor; CTAS, Canadian Triage and Acuity Scale; D&C, dilation and curettage.
Of the 2630 included patients, the mean age was 32.8±5.9 years (table 1). The percentage of patients seen by female versus male physicians did not significantly change from 2014 to 2019. One thousand six hundred seventy-two (63.6%) patients had an incomplete spontaneous abortion and the remaining 958 (36.4%) had a missed abortion. There were no significant differences in patient age, triage-to-physician assessment times, CTAS scores, Hb levels, HCG levels (used as a proxy for early gestational age and retained uterine tissue) or inpatient length of stay based on physician gender. Six hundred ninety-six patients did not have Hb levels and 1220 did not have HCG levels associated with their initial ED visit.
Female physicians saw a higher proportion of incomplete spontaneous abortions (68.0%) compared with male physicians (62.5%, p=0.019, table 1). Male physicians were more likely to be trained through a family medicine programme (CCFP-EM, p<0.001), older (p<0.001) and have more years of practice compared with female physicians (p<0.001).
Primary and secondary outcomes
One thousand one hundred eighty-two (44.9%) patients received an obstetrical consult at their initial ED visit (table 3). Six hundred sixty-nine (25.4%) patients underwent a D&C at their initial visit and the remaining 1961 (74.6%) patients were managed non-operatively (figure 1). Two hundred ninety-three of these 1961 non-operative patients (14.9%) returned to care for a D&C within 7 days (table 3). Five hundred thirty-seven (20.4%) patients returned to the ED within 7 days.
Management of pregnancy loss across physician gender
Using multivariable regression models, the odds of receiving an obstetrical consult were higher for patients seen by a female emergency physician (adjusted OR (aOR) 1.50, 95% CI 1.22 to 1.83, table 3). Patients seen by a female physician were also more likely to receive an initial D&C (aOR 1.35, 95% CI 1.08 to 1.69) and were less likely to return to care for a D&C (aOR 0.67, 95% CI 0.46 to 0.97). There were no significant differences in rates of ED returns or total D&C rates (combining both initial and return D&Cs). These multivariable regression models accounted for physician age, years of practice, training programme and type of pregnancy loss (ie, incomplete spontaneous abortion vs missed abortion).
Discussion
Interpretation of findings
In this multisite retrospective cohort study, we found there to be variation in the management of early pregnancy loss based on emergency physician gender. Patients seen by female physicians were more likely to receive an obstetrical consultation, initial operative management and were less likely to return for operative management within 7 days of their initial presentation. There was minimal variation in rates of ED returns or total D&C rates across physician gender. Patient demographics, acuity, laboratory values, and physician wait times were similar across physician gender. Significant differences in physician age, years of practice, training programme and type of pregnancy loss were controlled for using multivariable regression models.
Comparison with previous studies
Similar to our findings, previous studies have reported that female physicians consult specialists more frequently than their male colleagues and have a lower tolerance of risk.19 20 This may have contributed to the higher consult rates and fewer trials of non-operative management observed in this study. However, studies have also shown female physicians have lower rates of patient mortality23 24 and greater patient satisfaction17 21 suggesting this lower risk threshold may be beneficial for patients. Another hypothesis is that given female physicians’ greater emphasis on patient-centred care,17 18 female physicians may have consulted obstetrics more frequently if they believed these consults would provide greater patient comfort and satisfaction. In addition, female physicians may have been more likely to have their own personal experiences with pregnancy loss which could have influenced their clinical decision making. More research into the rationale behind these gender-based differences is required.
As D&Cs are performed by obstetricians and therefore require an obstetrician consult, higher consult rates by female emergency physicians resulted in a higher proportion of their patients receiving operative management and subsequently fewer returns for D&Cs. However, ED return rates and total D&C rates were similar across physician gender which is surprising given that non-operative management is normally associated with a higher risk of unplanned hospital admissions.6 These results may suggest that female physicians are better predictors of patients who require a D&C initially, which would explain their increased obstetrical consult rates and decreased D&C return rates. Regardless, pregnancy loss patients appear to have similar outcomes when seen by a female versus male emergency physician. Given these similar outcomes, patient preference should be considered and emphasised. Additional variables including patient mortality, complications and satisfaction were not addressed and should be included in future studies.
Strengths and limitations
This is a multisite study of four urban tertiary centres serving the Calgary zone and surrounding areas. This may limit generalisability of our findings to other communities or levels of care. ED returns and returns to care for D&Cs may have been underestimated as these outcomes were only assessed up to 7 days following initial ED visit. As well, patients could have returned to alternative care providers not included in this study such as EDs outside the Calgary area or family practitioners. We did not differentiate medical versus expectant management in the non-operative group, which may have elucidated further results. While we discuss physician gender as a dichotomous variable, we appreciate that gender identity is a spectrum which was not adequately addressed in this study. Gestational age was not available in this study, however given the focus of this study on first trimester pregnancy loss, as per the care model of the included ED sites, we believe HCG to be an appropriate correlate for gestational age given its use as a proxy for retained uterine tissue and as a biomarker for miscarriage and early pregnancy viability.27–29 Data on parity were not available and therefore were not included in this study. Despite controlling for potential confounders, we cannot rule out the possibility of residual confounders such as patient preference, physician practice and/or system-level factors which were not captured in this study.
Clinical implications
The results of this study have important implications both for emergency physicians and patients experiencing pregnancy loss. We hope this study will prompt physicians to reflect on their own practices and how their gender identity may be impacting the care they provide to patients. There are several studies focusing on the differences between male and female physicians, but limited research on emergency physicians specifically. Considering the diversity of patient presentations in the ED, we hope this study will provoke additional research on how emergency physician gender may influence patient care.
Conclusion
In summary, emergency physician gender was associated with the management of early pregnancy loss patients who presented to the ED, although this was not associated with ED return rates or total D&C rates. Greater understanding of physician decision making as well as patient preferences in these cases is needed.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
The current project was reviewed and approved by the Conjoint Health Research Ethics Board at the University of Calgary (REB20-2189). This study involves human participants.
References
Footnotes
Handling editor Mary Dawood
Contributors AS: data analysis, manuscript writing/editing. MW: developing the project proposal and protocol, manuscript writing/editing. FZ: manuscript writing/editing. KL: collection and organisation of dataset, manuscript editing. PB: developing research questions/protocol, manuscript editing. EL: developing research questions/protocol, planning data analysis, manuscript writing/editing, guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Commentary