Article Text

Abstract
Objectives Our aim was to determine the incidence of traumatic brain injury (TBI) in older adults and investigate the relationship between injury characteristics and outcomes.
Methods Retrospective analysis of prospectively collected data submitted to Trauma Audit and Research Network (TARN) database for a major trauma centre in the West Midlands, UK, from 2008 to 2014. The Mayo Scale was used to categorise TBI. All patients were aged ≥65 years and were admitted with head or brain injuries meeting TARN inclusion criteria: injury resulting in immediate admission to hospital for 3 days, admitted to a high dependency area or death following trauma. We determined age, gender, mechanism of injury, Injury Severity Score, presenting Glasgow Coma Scale (GCS) and Mayo Score, and the association of outcome (Glasgow Outcome Scale (GOS)) with age and clinical presentation.
Results 4413 patients were admitted with trauma meeting TARN criteria: 1389 were ≥65 years and 45% (624) had TBI. For patients ≥65 years with TBI, mean age was 79 (range 65–99); 56% were men. Falls accounted for 85% of all TBIs. Most TBIs were moderate/severe (80%) by the Mayo criteria. Of the 279 patients with subdural haematoma, 28% had neurosurgery. Most patients survived TBI (78%); 57% had a good outcome on GOS at discharge (not requiring care package). Mortality was associated with increased age (17% in ages 65–74 years, 19% in 75–84 years, 30% in ≥85 years, p=0.03). Outcome was significantly associated with injury severity (p=0.0001).
Conclusions Patients with TBI represented 45% of all trauma cases meeting TARN inclusion criteria. Falls at home accounted for most TBIs. Most had moderate/severe TBI, yet over half made a good recovery on GOS. Our data indicate that injury prevention initiatives should focus on home safety. Further research is needed to examine rehabilitation and follow-up after hospital discharge.
- Trauma
- accidental falls
- emergency department
- geriatrics
- neurology
Statistics from Altmetric.com
Key messages
What is already known on this subject?
Traumatic brain injury is a common cause of admission to hospital in older adults, particularly due to falls.
Mortality rates after brain injury increase with age.
Head or brain injuries may be missed when other injuries are present, resulting in underestimated incidence rates.
What this study adds?
Traumatic brain injury (TBI) is associated with almost half of all admissions for major trauma in older adults.
The main cause of brain injury was a low level fall. Most of the injuries occurred at home.
Most patients had moderate or severe TBI, yet over half made a good recovery, as measured by the Glasgow Outcome Scale. Patients aged 85 years and over had poorer outcomes.
Subarachnoid haemorrhage and subdural haematoma are most common in this age group.
Introduction
Traumatic brain injury (TBI) is an important cause of hospital admission for older adults, and in the USA is responsible for over 80 000 emergency department visits annually.1 Adults aged 65 years and over made more than 3.5 million visits to emergency departments in England during the financial year 2012–2013.2 Emergency department attendances by this age group formed 19% of the 18.3 million emergency department attendances in England that year. In England in 2012–2013, there were 423 413 emergency department attendances with a primary diagnosis of head injury in all age groups. At the NHS provider level, the Health and Social Care Information Centre presents age in 10 year bands, so data are available for patients from aged 60 years upwards. At University Hospital Coventry and Warwickshire (UHCW) NHS Trust, there were 42 569 emergency department attendances among patients aged 60 years and over during the 1 year 2012–2013, 24% of the 175 351 total.2
Falls are the most frequent cause of hospital admission for older adults,3 and also the most common mechanism for TBI.4 ,5 Older age at injury is associated with worse functional outcomes after TBI, regardless of injury severity.6 ,7 Mortality resulting from TBI also increases with age, rising from 71% in 65–70-year-old patients to 87% for patients >80 years.8 There are currently over 11 million people aged 65 years and over in the UK, representing 17% of the population; this is estimated to rise to 25% by 2041.9 Consequently, numbers of older adults presenting with TBI are also likely to rise.
Although TBI in older adults is a significant public health issue, few studies have examined the relationship between clinical presentation and outcomes.10 In the UK, the Trauma and Audit Research Network (TARN) is dedicated to the collection and assessment of data on trauma and outcomes.11 Data are collected prospectively and submitted to TARN. In 2008, UHCW commenced data collection for TARN, and has a high data completeness record compared with other trauma receiving hospitals. In March 2012, UHCW became a Major Trauma Centre.
The purpose of this study was to analyse data for UHCW submitted to TARN over a 6 year period to identify all adults aged 65 years and over admitted with head, brain or skull injuries. The study objectives were (a) to describe the epidemiology of older adults presenting with TBI and (b) to examine variables which may be predictive of short term outcome, as measured by the Glasgow Outcome Scale (GOS).
Method
Data were collected from TARN documentation over a 6 year period, from 13 September 2008 to 26 September 2014. Patients of any age with brain or skull injuries are recorded in TARN if their length of stay (LOS) is 3 days, they are admitted to a high dependency area or they die following trauma. For this study, only patients aged ≥65 years were included.
Study inclusion criteria were patients aged ≥65 years and recorded on TARN with definite, probable or possible TBI. (For comparisons between numbers of younger and older adults recorded on TARN, all adults aged 16 years and over were counted.)
Exclusion criterion was no evidence of head or brain injury.
TARN records age, gender, Glasgow Coma Scale (GCS), Injury Severity Score (ISS), location of incident, injury cause, injury description, brain imaging results, comorbidities, treatment, LOS, discharge destination and survival outcomes. The GCS is usually taken on arrival at the emergency department, except when the patient is intubated in which case the GCS at the scene is used. ISS is calculated by TARN from data supplied. It is based on the three highest Abbreviated Injury Scale scores for three separate body regions. These three figures are squared and added together to give ISS.11
Definition of TBI
The Mayo classification system for TBI severity was used to define TBI for the following two reasons.12 (1) It allows injury severity to be calculated using clinical descriptions instead of relying on GCS alone. Many patients recorded in TARN had a GCS of 15 with accompanying clinical data, suggesting an injury more serious than minor. (2) It allows injury severity to be calculated for patients with missing GCS data. The Mayo system classifies TBI as moderate–severe (definite), mild (probable) or symptomatic (possible).
Moderate–severe (definite) TBI if one or more of the following criteria apply:
Death due to this TBI.
Loss of consciousness ≥30 min.
Post-traumatic amnesia ≥24 hours.
Worst GCS full score in first 24 hours <13 (unless invalidated due to sedation, for example).
One or more of the following present: intracerebral haematoma, subdural haematoma, epidural haematoma, cerebral contusion, haemorrhagic contusion, penetrating TBI (dura penetrated), subarachnoid haemorrhage or brain stem injury.
Mild (probable) TBI if one or more of the following criteria apply:
Loss of consciousness of momentary to <30 min.
Post-traumatic amnesia of momentary to <24 hours.
Depressed, basilar or linear skull fracture (dura intact).
Symptomatic (possible) TBI if one or more of the following criteria apply:
Blurred vision; confusion; dazed; dizziness; focal neurologic symptoms; headache; or nausea.
In addition to the Mayo Scale, for patients with GCS recorded TBI was categorised as mild (GCS 13–15), moderate (GCS 9–12) or severe (GCS 3–8).13
Probability of survival (PS) rates are also calculated by TARN. Calculations of PS have changed during the 6 year data collection period as the PS model, currently PS14, is regularly revised.11 PS is currently based on age, gender, GCS, ISS, comorbidities and outcome at 30 days.
For TARN, outcome is traditionally measured as mortality/survival at 30 days or at discharge. Recently, there has been an emphasis on the quality of survival, hence inclusion of the GOS in TARN. Therefore, in this study, outcome was determined using GOS at discharge, which ranged from death to good recovery (no care package).
Statistical analysis
SPSS V.22 was used for both descriptive statistics and exploratory analysis. For comparison, age was divided into three categories 65–74, 75–84 and ≥85 years. Mechanism of injury, age at injury, clinical presentation and outcomes were examined using frequencies.
Data were analysed to test the hypothesis that TARN injury variables are related to outcome at discharge. We used χ2 cross tabulations to explore the relationships between categorical variables. In the analyses, predictor variables were age, TBI severity (Mayo Scale), GCS, ISS, PS, LOS and LOS in critical care (LOSCC). Outcome was measured by the GOS. Non-parametric statistics were used where the assumptions of parametric statistics were not met. The independent samples t-test was used to compare means where data were normally distributed. The Mann–Whitney U test was used to compare the distribution of values between independent groups. The independent samples Kruskal–Wallis test was used to examine the relationship between continuous variables (ISS, PS, GCS, LOS, LOSCC, age) and GOS. The significance level was set at 0.05. Additionally, the characteristics of those who had neurosurgery were compared with those who did not (t-test, Mann–Whitney U test, χ2 test), and LOS was compared between age groups (medians and IQR). The prognostic ability of the two injury severity scales (Mayo and GCS) were compared using receiver operating characteristic (ROC) analysis using the optimum cut-off for each test (the point on each curve that is closest to the upper left hand corner).
Results
From September 2008 to September 2014, 4413 adult patients aged 16 years and over were admitted by UHCW for trauma injury and recorded on the TARN database. Of these, 1389 patients (31.5%) were aged ≥65 years, and 624 patients in this group (44.9%) had a head or brain injury. Of the 3020 patients aged 16–64 years, 1122 (37.2%) had a head or brain injury. All 624 older adults had a Mayo score recorded, 579 also had a GCS recorded, and GOS outcome was obtained for 609. Table 1 shows year by year comparisons of numbers and proportions of patients recorded on TARN with and without head trauma. The number of older adults admitted with head trauma on TARN almost trebled from 59 in 2009 to 168 in 2013 at our emergency department. However, the percentage of elderly patients with head trauma remained at a similar level over time.
Patients recorded on TARN with and without head trauma. Comparison of older and younger patients by year of admission
There were no significant differences in admissions for each month of the year, although there were slight peaks in June, August and September. There were no differences in monthly admissions when analysed by gender or age group.
Older adults
Most patients (505, 80.9%) were direct admissions from the field to the emergency department and not transferred to or from another hospital. Mean age was 79.2 years (SD 8.7), range 65–99 years and 55.9% were men. The three age groups had similar numbers of patients: 65–74 years (n=206, 33.0%), 75–84 years (n=227, 36.4%) and ≥85 years (n=191, 30.6%).
Among the 624 patients aged ≥65 years with TBI, falls accounted for 527 (84.5%) injuries and 378 (60.6%) of these were low level falls of <2 m. Road traffic accidents accounted for 85 head injuries (13.6%), and 12 ‘other’ categories (assaults or struck by object) accounted for the rest. There was a significant difference in injury mechanism for men and women (p<0.001, Pearson χ2=16.6, df=3). Men had more high level falls (>2 m) and road accidents. There was also a significant difference in injury mechanism between age groups (p<0.0001, Pearson χ2=46.0, df=6). Table 2 shows the mechanism of injury stratified by age. The incidence of low level falls increased with age and there were more road accidents among younger (65–74 years) adults.
Injury mechanism by age group
Almost two thirds of head/brain injuries took place in the home (402, 64.4%); only 43 (6.9%) took place in an institution (hospital or nursing home). Eighty-five injuries took place on a road (13.6%) and 79 took place in another public area (12.7%).
Previous medical history was recorded for 505 of 624 patients; only 7 (1.1%) patients had no pre-existing medical condition, while for the remaining 498, the most common medical conditions were hypertension (113, 22.7%), dementia (57, 11.4%), diabetes (41, 8.2%), arthritis (36, 7.2%), heart disease (33, 6.6%), cancer (27, 5.4%), chronic obstructive pulmonary disease (22, 4.4%) and asthma (20, 4.0%). Past medical history was either unknown (28 patients, 4.5%) or not recorded (91 patients, 14.6%).
Injury type and severity
A total of 4135 patients had a CT scan, of whom 96.3% had a head CT scan; 145 patients had no CT scan and 44 died before a CT was performed. Table 3 shows the most significant head or brain injury for all patients, stratified by age. There was no significant difference in type of head or brain injury between age groups (p=0.3, Pearson χ2=9.7, df=8). A total of 265 patients (63.2%) with a head CT had more than one area of brain injury. A subdural haematoma was taken to be the worst injury, so when a patient had both subdural haematoma and subarachnoid haemorrhage, the subdural haematoma was recorded as the most significant. Subarachnoid haemorrhage was also examined separately, and was present in 206 patients (33.0%).
Categories of brain injury by age group
ISS was available for all patients and ranged from 2 to 75, with a mean of 20.7 (SD 9.1). A PS score was available for 614 TBI patients. These ranged from 1.3 to 98.6, with a mean of 75.0 (SD 24.6).
The Mayo score was calculated for all patients: 502 (80.4%) had a moderate or severe TBI, as measured by the Mayo Scale (502, 80.4%) a further 34 (5.4%) had a mild, probable TBI; and the remainder (88, 14.1%) had a mild, possible TBI. For the 579 patients with GCS scores, the majority (439, 70.4%) had a mild injury defined by GCS 13–15 (abnormal CT results were not taken into account). There was no significant difference in severity between age groups using either classification (GCS: p=0.4, Pearson χ2=4.0, df=4; Mayo: p=0.06, Pearson χ2=9.0, df=4), (table 4).
Injury severity by age group
Treatment and management
Most TBI patients aged ≥65 years were treated conservatively; 483 patients (77.4%) had no operation. Ninety-four patients (15.1%) had a neurosurgical intervention, most commonly burr hole of the cranium (51, 8.2%) or craniectomy (28, 4.5%).
Of the 279 patients with subdural haematoma, 77 (27.6%) had a neurosurgical intervention. Patients who received neurosurgery were younger (t=−2.1, p=0.04, mean age 77.6 (SD 7.7) years compared with 80.0 (SD 8.9) years), and were more likely to be men (p<0.02, Pearson χ2=5.8, df=1). The majority of patients receiving neurosurgery (70, 90.9%) had no other significant injuries (p<0.009, Pearson χ2=6.8, df=1). Outcomes for those having neurosurgery were not significantly better (18.2% mortality) than for those without surgery (27.2% mortality) (p=0.1, Pearson χ2=2.5, df=1). Patients receiving neurosurgery had higher ISS scores (Mann–Whitney U, p=0.01), but there was no difference for GCS scores (Mann–Whitney U, p=0.3).
Median length of hospital stay was 13 days (range 1–262 days, IQR 21). Median LOSCC was 0 days (range 0–60 days, IQR 0). Patients aged ≥85 years had the longest median LOS (16 days, range 1–104, IQR 23) and patients aged 65–74 years the shortest (11, range 1–195, IQR 15). Patients aged 75–84 years had a median stay of 14 days (range 1–262, IQR 25). There was little difference between age groups regarding LOSCC—median values were 0 for each age group (65–74 years: range 0–60, IQR 3; 75–84 years: range 0–29, IQR 1; ≥85 years: range 0–13, IQR 0).
Outcomes at discharge
A total of 143 (22.9%) elderly head injured patients died following admission to UHCW. There was a significant association between age group and outcome, with the ≥85 year age group showing the highest mortality (32.5%) (p<0.03, Pearson χ2=17.4, df=8). Table 5 shows GOS scores at discharge stratified by age group. Younger patients were more likely to make a good recovery, and the oldest patients had almost double the mortality rate of 65–74 year olds.
Glasgow Outcome Scale at discharge, and discharge destination by age group
Of the 609 patients for whom GOS was obtained, 493 presented with moderate/severe TBI according to the Mayo Scale. In this group, 136 (27.6%) died, 26 (5.3%) had severe disability, 53 (10.8%) had moderate disability and 278 (56.4%) made a good recovery (table 5). GOS was significantly associated with Mayo injury severity (p<0.0001, Pearson χ2=39.4, df=6). There were more deaths in the moderate/severe group (136, 27.6%) and more good recovery in the mild, possible TBI group (63, 74.1%).
Among those who had a GCS assigned, 567 had a GOS. Of the 136 patients with moderate or severe TBI by GCS, and a GOS obtained, 80 (58.8%) died, 14 (10.3%) had severe disability, 10 (7.4%) had moderate disability and 32 (23.5%) made a good recovery. GOS was also significantly associated with GCS severity (p<0.0001, Pearson χ2=183.5, df=6). There were more deaths in the severe TBI group (59, 75.6%) and more good recovery in the mild TBI group (306, 71.0%).
The ability of the Mayo and GCS severity scales to predict mortality were compared using ROC analysis (figure 1). Although the area under the curve was higher for GCS (0.71, CI 0.66 to 0.77) than for Mayo (0.60, CI 0.55 to 0.64), Mayo showed greater sensitivity (0.95) than GCS (0.63). However, GCS had higher specificity (0.80) than Mayo (0.24).
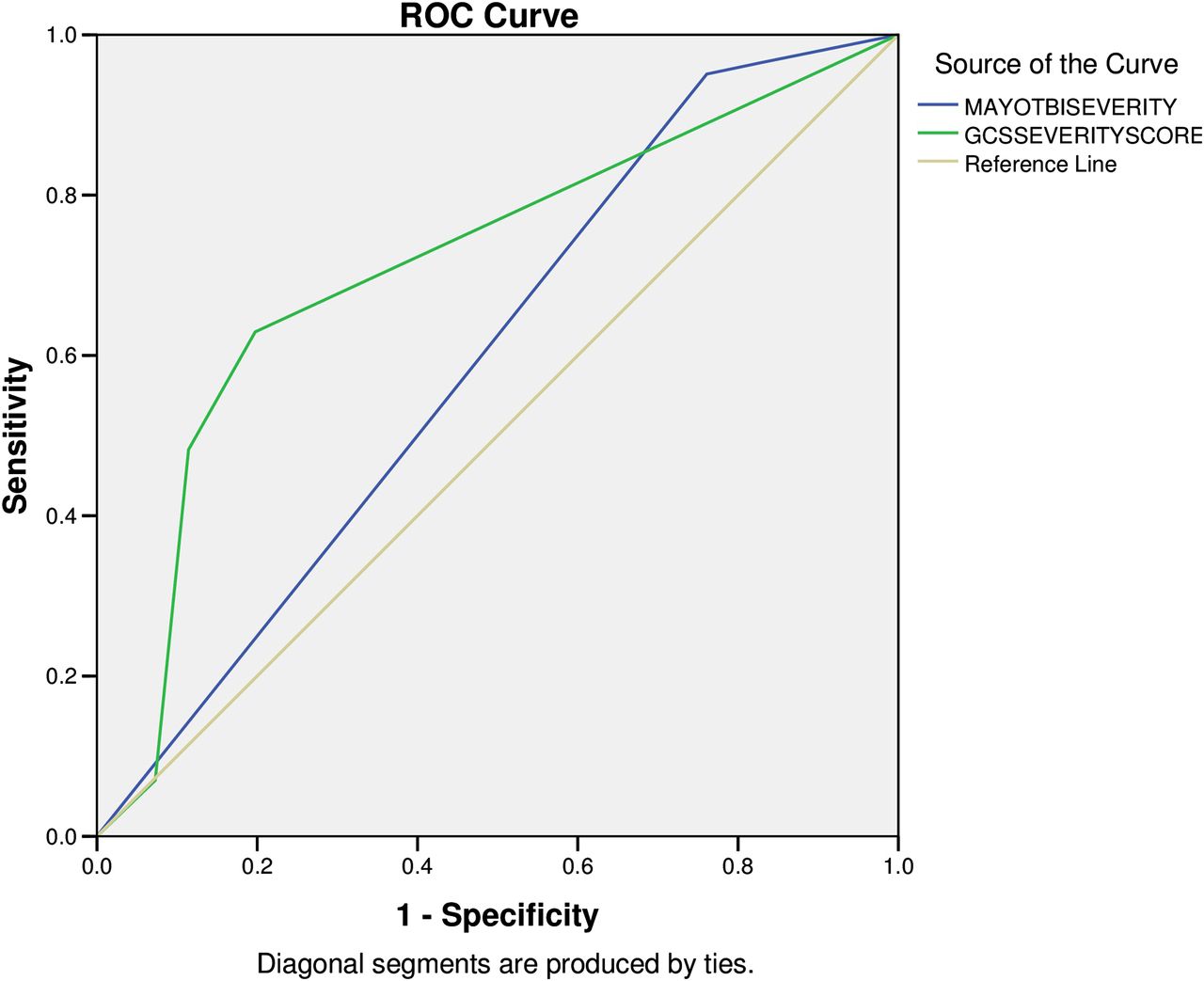
Receiver operating characteristic (ROC) curve comparing Glasgow Coma Scale (GCS) and Mayo severity scores against Glasgow Outcome Scale mortality outcome (likelihood of death).
Discharge destination
Most patients were discharged to their home or usual place of residence (343, 55.0%). Thirty-four patients (5.4%) were discharged to a different hospital and 48 patients (7.7%) were discharged to a nursing or care home. Only 36 patients were discharged to an external rehabilitation facility. Table 5 shows destination at discharge by age group. There was a significant difference in discharge destination between age groups: more patients aged ≥85 years died, fewer patients aged ≥85 years were referred for rehabilitation, fewer aged ≥85 years were discharged home and more aged ≥85 years were discharged to a nursing/care home (p<0.0001, Pearson χ2=50.3, df=10). Thirty-six patients (5.8%) were readmitted to UHCW within 30 days of admission.
There was a significant association between Mayo severity score and discharge destination (p<0.0001, Pearson χ2=72.68, df=10). Most patients with mild, possible TBI (61.4%) were discharged to their usual place of residence compared with 53.8% of those with moderate/severe TBI. Twenty-seven patients (5.4%) in the moderate/severe group were referred for rehabilitation compared with 4 (11.8%) in the mild, probable group and 5 (5.7%) in the mild, possible group.
Prediction of outcome in TARN
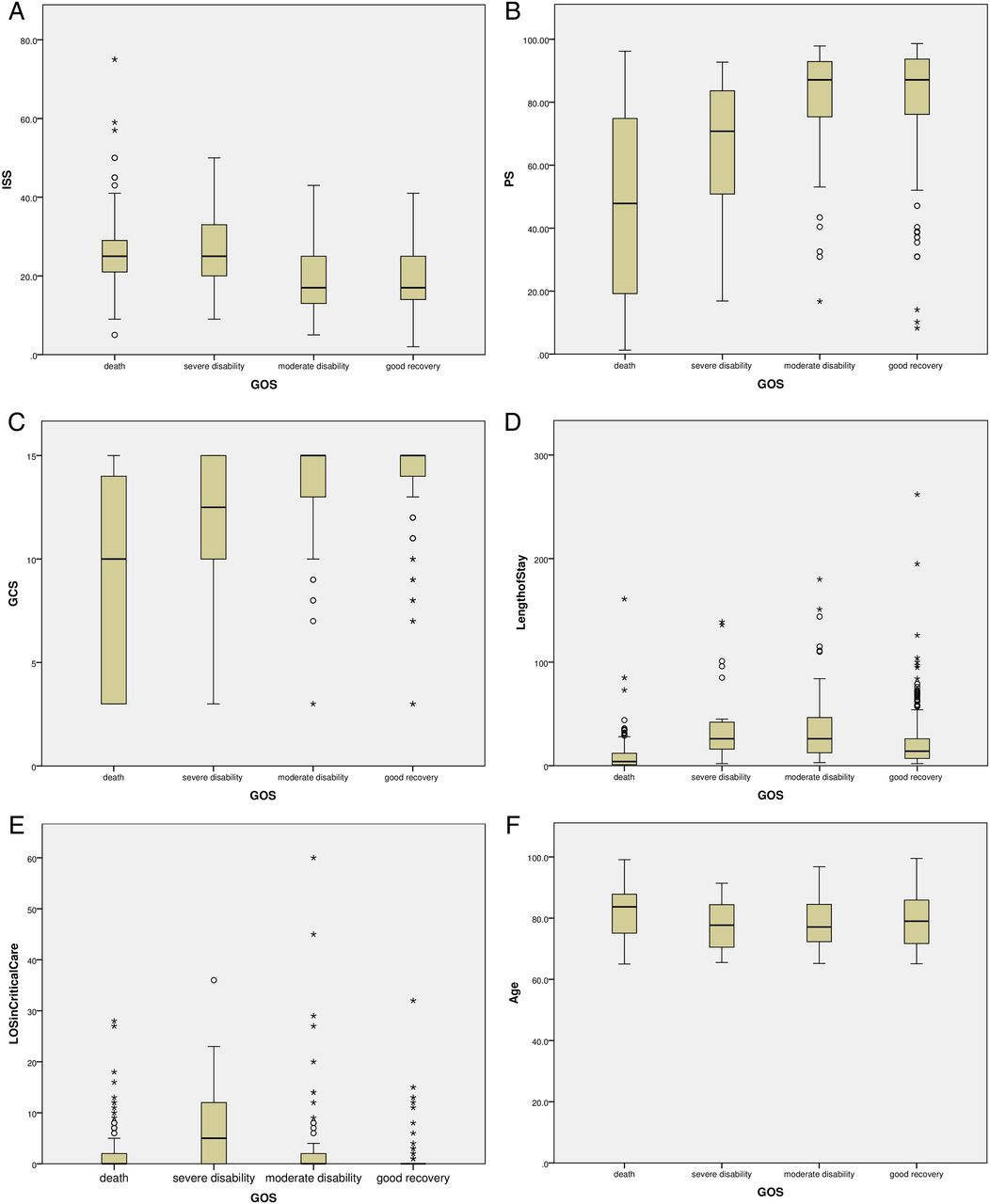
GOS outcomes at discharge were compared with predictor variables (ISS, PS, GCS, LOS, LOSCC, age). There were significant relationships (p=0001) between GOS scores and all predictor variables. GOS scores were worse in patients with higher ISS, PS and age, and better in those with higher GCS. LOSCC was associated with worse GOS whereas patients with the lowest overall LOS were more likely to have a good recovery (figure 2A–F).
{kind=link}
{kind=link}
(A) Box plot of Glasgow Outcome Scale (GOS) and Injury Severity Score (ISS). (B) Box plot of GOS and probability of survival (PS). (C) Box plot of GOS and Glasgow Coma Scale (GCS). (D) Box plot of GOS and length of stay. (E) Box plot of GOS and length of stay (LOS) in critical care. (F) Box plot of GOS and age.
Discussion
Almost half of all trauma patients aged ≥65 years have TBI. Most TBIs were moderate/severe (80%) according to the Mayo Scale. Increased age was associated with higher mortality and greater disability among survivors. Just over half of the patients with TBI were men. Falls accounted for 85% of TBIs. For patients ≥aged 85 years, a low level fall was the most common cause of brain injury. Most brain injuries occurred in the home. The most frequently occurring brain injury for all age groups was a subdural haematoma. Most patients were discharged to their usual place of residence, most frequently their own home. Only 5.8% were discharged to an external rehabilitation facility. ISS, LOS, LOCC, PS, Mayo and GCS scores were associated with GOS scores at discharge.
Strengths
This study used data collected over a 6 year period for an unselected patient group and is thus able to identify admission trends over time. TARN data are subject to quality control and data checks to ensure consistency in recording and data accuracy. UHCW has high data completeness compared with other trauma receiving hospitals contributing to TARN.
Limitations
We identified all patients on TARN who had head trauma. Some patients with mild TBI may have been recorded on TARN because of additional serious injuries or another acute medical condition. There are also likely to be many older patients with mild TBI who are not recorded on TARN, so we have not identified all older patients admitted to UHCW with head trauma.
Only since November 2014 have TARN followed patients post discharge by obtaining final outcome details via linkage with the Office of National Statistics data, and therefore long-term outcomes are unknown for this study period. Here a good outcome was recorded when the patient was discharged without a care package arranged by the hospital. When a patient was discharged back to a nursing home, the hospital did not normally arrange a care package, and thus although a ‘good’ outcome was recorded the patient is likely to have had significant care needs.
Comparison of findings with previous studies
We found an increasing number of hospital admissions for TBI among older adults. This finding is consistent with previous studies.10 ,14 In the USA, the age adjusted rate of hospitalisation for adults aged ≥65 years is reported as 156 per 100 000, more than double the rate of 60.6 for the general population.15 In high income countries, the absolute incidence of TBI in older adults has been steadily increasing as a result of increased life expectancy and greater mobility.16 ,17
In this study, falls were found to be the most common mechanism of injury. Previous research has identified falls as the leading cause of TBI in older adults.4 ,10 ,18 We found low level falls to be most common in the oldest age group. Similarly, Sterling et al 4 reported that ‘same level’ falls result in serious injury 30% of the time in patients aged ≥65 years compared with 4% in patients aged <65 years. They also found that for patients aged ≥65 years, same level falls were 10 times more common as a cause of death than for patients <65 years.
Several studies have identified increased age as a factor prognostic of mortality following TBI.18–22 In our study, mortality after TBI was highest in patients aged ≥85 years at 32%, almost double the rate among 65–74 year olds. However, in our group of patients with TBI of any severity, mortality was unsurprisingly much lower than the 87% reported by Patel et al among patients recorded on TARN with severe head injury (GCS <9).8
We found almost equal numbers of men and women with TBI, which differs from epidemiological studies of younger adults and children. However, other studies of TBI in older adults have reported a similar gender split—for example, 55% men by Utomo et al in Australia, and 50% men by Susman et al in the USA.7 ,18
Forty-five per cent of patients in our study had subdural haematoma. Most patients had at least one comorbidity, and many are likely to have been taking medications for pre-existing conditions which may have increased their risk of haemorrhagic contusions and subdural haematomas.17 One third of our patients had a subarachnoid haemorrhage. The presence of subarachnoid haemorrhage or subdural haematoma is associated with elevated mortality rates.23 ,24
Just over a quarter of patients with subdural haematoma received neurosurgical intervention; they were more likely to be men and in the younger age groups. As increased age is a strong predictor of mortality in prognostic models of outcome, it is likely that neurosurgery was offered to those patients thought most likely to benefit.8 ,19 ,22 However, the finding regarding a gender difference needs further exploration. While we found no significant difference in outcome among those with or without neurosurgery, the study was not powered for this outcome, nor were potential confounders assessed.
Implications of the study
The silver tsunami is coming. The number of elderly trauma patients is on the increase. These patients can present with serious injuries from seemingly benign mechanisms. In this study, it was clear that low level falls caused most injuries. Most of this trauma occurred at home. Home safety and education for falls prevention is of paramount importance in reducing such serious injuries. These measures will save lives and be cost effective compared with the lost lives and LOS in hospital. In the USA, it has been estimated that fall related medical costs among people aged ≥65 years amounted to 19 billion US$ for non-fatal and US$ 0.2 billion for fatal injuries in 2006.25 Our findings are generalisable to other hospitals in developed countries with aging populations.
The GCS score that guides clinicians to perform a CT scan after head injuries appears to be an unreliable tool for older patients, as many had abnormal findings despite a presenting GCS of 15 or 14. The accuracy of GCS to reflect the severity of injury in older patients has recently been questioned, and there have been calls for modification of GCS severity criteria for elderly patients.26 ,27 Swann and Teasdale reported that the risk of an intracranial haematoma in patients with GCS 15 increases from 1 in 31 300 if there are no other clinical features, to 1 in 29 if accompanied by skull fracture and post-traumatic amnesia.28 In this study, the Mayo severity scale proved to be a more sensitive measure of outcome than the GCS severity scale and will be a useful tool in planning discharge, rehabilitation and care facility following discharge. It will also be useful in enabling clinicians to better advise patients and their families about future limitations and disabilities. However, ROC analysis showed that GCS has greater specificity than Mayo in predicting death from TBI, and thus GCS may be more useful in informing clinicians at an early stage about which patients will benefit from surgery or intervention versus those who should be treated conservatively when the PS is low.
This study has highlighted the importance of clinicians remaining vigilant when dealing with elderly patients presenting with trauma as many patients had serious brain injuries after low level trauma. Falls are a major cause of TBI in the elderly, most taking place at home. Falls prevention strategies should target these high risk groups.
Future research
This study examined short term outcomes but future research should follow-up older patients after hospital discharge as sequelae from brain injury can be long lasting. The support offered to older people after brain injury should be investigated as this study found that few were referred for rehabilitation. Awareness of brain injury among staff in nursing and care homes should be explored.
References
Footnotes
Contributors CH and MS designed the study. CH analysed the data and wrote the paper. JS collected the TARN data. SS collected additional data. All authors contributed to and commented on the final manuscript. CH and MS are guarantors. This article conforms to the STROBE V4 checklist (http://www.strobe-statement.org/index.php?id=strobe-home).
Funding SS received a bursary from the University of Warwick under the University Research Scholarship Scheme. The researchers are independent of the above funding.
Competing interests None declared.
Ethics approval TARN already has ethical approval (ECC 7-05(g) 2011) for research on the anonymous data recorded in TARN.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement TARN data are available at a national level from TARN.