Article Text

Abstract
The UK is currently in the process of implementing a modified response to chemical, biological, radiological and nuclear and hazardous material incidents that combines an initial operational response with a revision of the existing specialist operational response for ambulant casualties. The process is based on scientific evidence and focuses on the needs of casualties rather than the availability of specialist resources such as personal protective equipment, detection and monitoring instruments and bespoke showering (mass casualty decontamination) facilities. Two main features of the revised process are: (1) the introduction of an emergency disrobe and dry decontamination step prior to the arrival of specialist resources and (2) a revised protocol for mass casualty (wet) decontamination that has the potential to double the throughput of casualties and improve the removal of contaminants from the skin surface. Optimised methods for performing dry and wet decontamination are presented that may be of relevance to hospitals, as well as first responders at the scene of a chemical incident.
- major incidents, cbrn
- mass incidents
- toxicology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The deliberate use of toxic materials represents a serious threat to society. In particular, chemical warfare agents are indiscriminate weapons that can have a devastating impact when used on unprotected civilian populations, as recently evidenced in Syria.1 Any complacency based on the notion that chemical warfare agents are limited to politically unstable regions was recently dispelled by the use of a ‘novichok’ nerve agent in the UK.2 3 The current threat level for international terrorism in the UK is classed as ‘severe’.4
The UK approach for preparing and responding to the threat of terrorism has been developed over the last 15 years as part of the UK Government’s ‘CONTEST’ strategy.5 One outcome of this strategy was the development of the ‘Model Response’, which sets out the operational parameters for responding to the deliberate release of chemical, biological or radiological materials.6 Along with a corresponding investment in equipment and training, the Model Response has provided the UK’s emergency services with a range of bespoke resources and procedures for effectively dealing with chemical, biological, radiological and nuclear (CBRN) and hazardous material (HazMat) incidents.
The Model Response was based on delivering specialist assets directly to the scene of an incident. This includes the deployment of trained responders with appropriate protection and detection capability, medical countermeasures and bespoke disrobe and decontamination facilities. Clearly, such an approach is dependent on the timely arrival of assets on-scene. For incidents involving the release of biological or radiological materials, a short delay in the deployment of specialist resources may not have significant health consequences for exposed individuals. However, this may not be the case for chemical agents, particularly those with a rapid onset of action, such as hydrogen cyanide or nerve agents.7
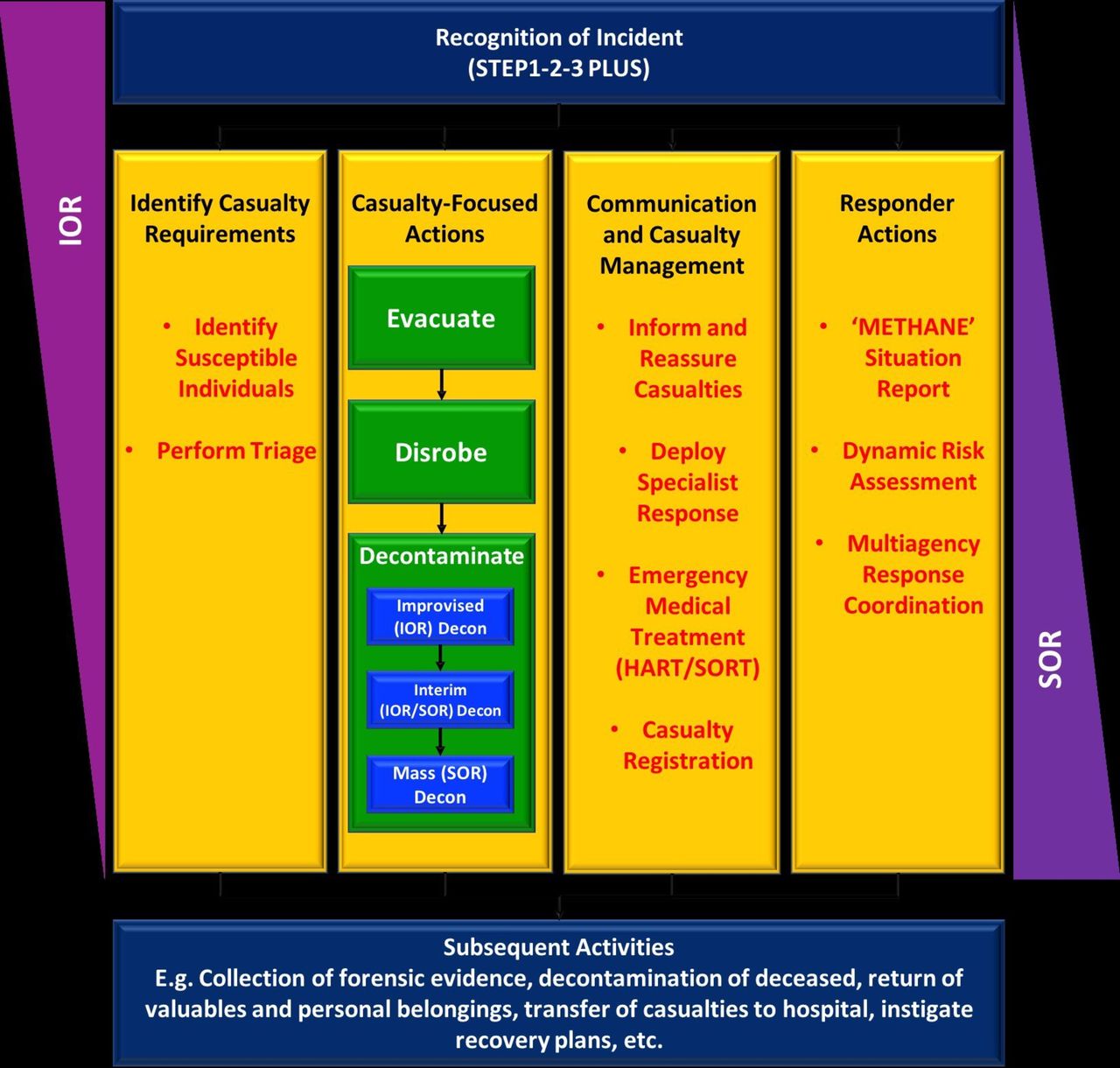
A series of research projects were commissioned from 2008 to evaluate various aspects of the Model Response.8 9 These primarily focused on issues relating to the rapidity of the response and optimisation of the existing mass casualty disrobe and decontamination process. The initial research trials were performed as part of a programme of work known as Optimisation through Research of CHemical Incident Decontamination Systems (‘ORCHIDS’). The outcome of the ORCHIDS projects led to a number of recommendations on how the Model Response could be optimised to improve casualty management and has led to the implementation of a revised process that entails an initial and specialist (or strategic) operational response (IOR and SOR, respectively; figure 1).10 Subsequent work has confirmed the effectiveness of this approach and has extended the scope of evidence to include hair decontamination.11 A detailed description of the IOR and SOR processes would be outside the scope of this review, which will focus on aspects of disrobe and decontamination.

Summary of operational response to chemical or HazMat incidents indicating the tapering elements of the initial operational response (IOR) and specialist operational response (SOR) and main associated tasks. Note that the list of tasks is not exhaustive and is for indication only. HazMat, hazardous material. HART = Hazardous Area Response Team. SORT = Special Operations Response Team.
Evidence base
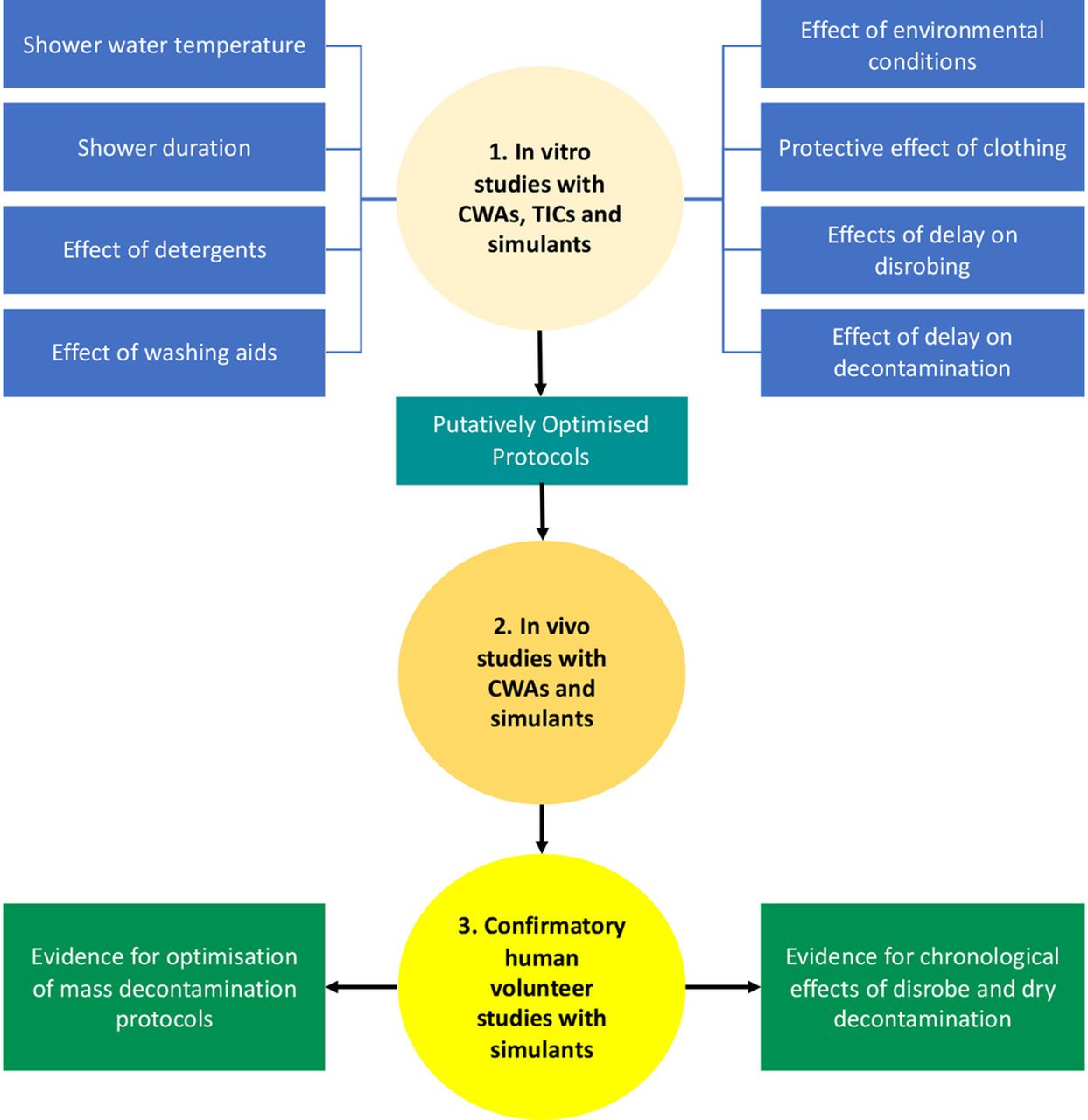
The IOR and SOR build on scientific evidence derived from a series of in vitro, in vivo and human volunteer studies (figure 2). Initial (in vitro) skin absorption studies focused on the effects of individual decontamination parameters, such as the duration of decontamination and the protective effects of normal (civilian) clothing against chemical warfare agents, toxic industrial chemicals and simulants. The outputs of the in vitro studies included a putatively optimised mass casualty decontamination (MCD) protocol and information on the temporal effects of disrobing and decontamination. The combined outputs of the in vitro study were subsequently confirmed in a series of in vivo (animal) studies prior to a final series of human volunteer studies using two relatively non-toxic simulants: fluorescent particles to model a biological or radiological agent12 and methylsalicylate, previously used as a simulant for chemical warfare agents.13 14 Collectively, these studies resulted in a number of evidence-based recommendations, including: (1) the need to introduce an ‘emergency disrobe and decontamination’ stage prior to the arrival of bespoke MCD units and (2) the optimisation of MCD through adoption of the ‘ORCHIDS Protocol’, namely a shower duration of 90 s with water at a temperature of 35°C and a washing aid such as a face cloth.7 Overall, the ORCHIDS projects indicated that, while the effectiveness of MCD can be substantially improved by relatively simple and cheap interventions, there is a need to improve the rapidity of the response to make it more patient oriented and to maximise the use of time during the earliest phases of an incident, hence the introduction of the IOR. This approach has since been adopted in the UK15 and within US Federal Guidance.16

Outline of ORCHIDS projects illustrating a three-tier approach based on in vitro, in vivo and human volunteer studies. Simulants were fluorescent particles and methylsalicylate. CWAs, chemical warfare agents; ORCHIDS, Optimisation through Research of CHemical Incident Decontamination Systems; TICs, toxic industrial chemicals.
The introduction of an early ‘emergency disrobe and decontamination’ stage requires the use of dry, absorbent materials for decontamination that may be more readily available at the scene of an incident than warm, soapy water. Moreover, there is a growing recognition that dry decontamination may offer other advantages over aqueous (shower based) decontamination. For example, dry decontamination does not lead to the generation of large volumes of contaminated waste, does not cause transfer and spreading of contaminants through clothing and is not associated with the ‘wash-in’ or ‘rinse-in’ effect, where the dermal absorption of certain chemicals may be transiently increased by washing with water.17–20
Recent work has demonstrated that a variety of absorbent materials (particularly those that are readily available in a clinical environment (such as an ambulance or hospital) could be used for emergency decontamination.21 22 Such materials include absorbent tissue paper, incontinence pads and absorbent wound dressings, as well as domestic products such as cotton wool, kitchen paper, nappies (diapers) and toilet paper. Above all, the ad hoc nature of disrobe and dry decontamination means that the process can be instigated within seconds or minutes of exposure. This is a critical feature, since the effectiveness of disrobe and decontamination decreases exponentially with time.7 23 It should be noted that the emergency disrobe and dry decontamination element of the IOR is specific to non-corrosive, liquid contaminants. The efficacy of dry decontamination is substantially reduced if the contaminant is a solid, such as a powder.21 Moreover, the cooling effects of water may be more appropriate for treating skin contamination with corrosive chemicals, although dry decontamination may be of clinical benefit in reducing exposure until a source of water becomes available.
Comparison of IOR/SOR and Model Response
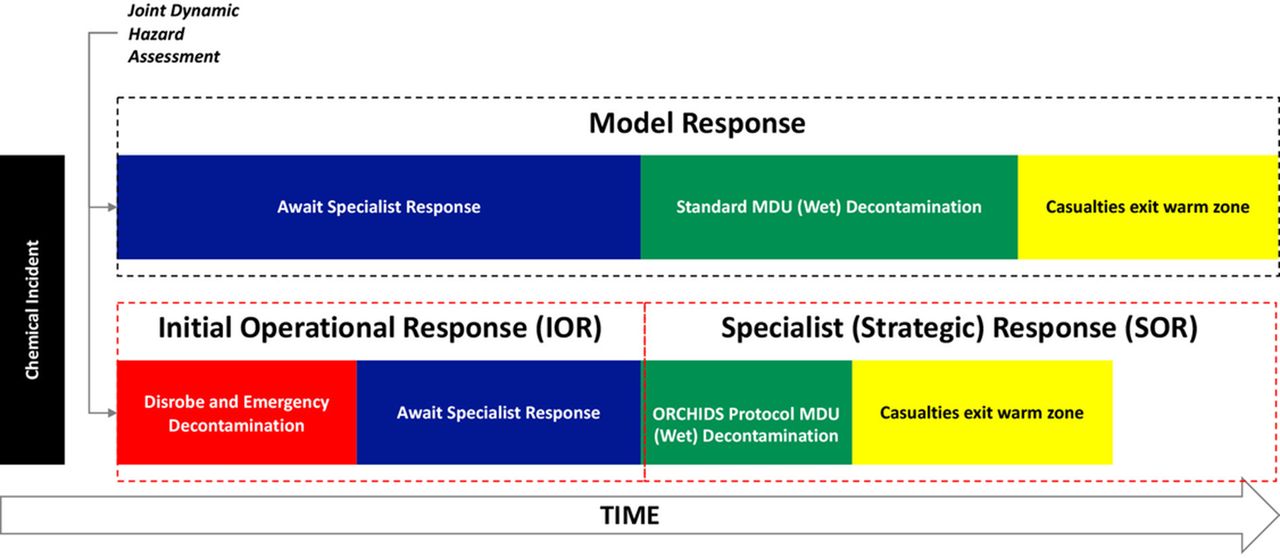
The main feature of the new response process is the introduction of an ‘emergency disrobe and decontamination’ stage at the earliest possible opportunity (figure 3). This new step allows the instigation of these potentially life-saving processes to be performed as soon as readily practicable rather than after the arrival of specialist resources. A second major improvement is the utilisation of the ‘ORCHIDS’ showering protocol, which may halve the time taken to process casualties through mass decontamination units (MDUs).
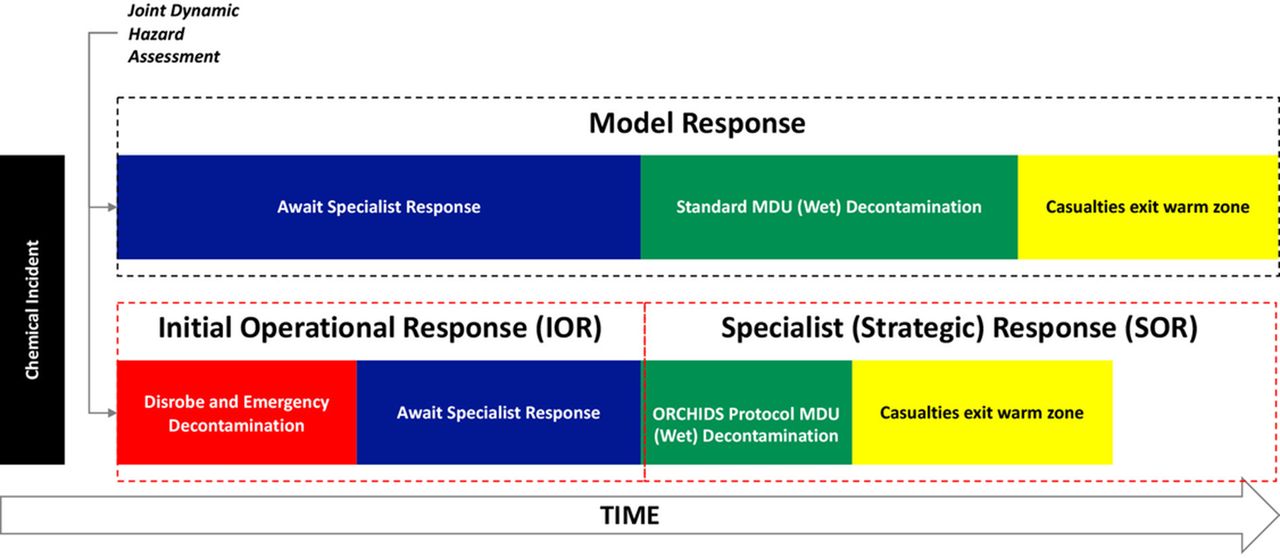
Salient features of the original Model Response in comparison with the new initial operational response (IOR) and specialist operational response (SOR). The IOR, which is essentially a form of first aid, leads into the SOR, where additional resources are made available, such as mass decontamination units (MDU). ORCHIDS, Optimisation through Research of CHemical Incident Decontamination Systems.
The addition of an emergency disrobe and decontamination step necessitates a joint dynamic hazard assessment (JDHA) to ensure the safety of emergency responders when issuing verbal instructions at the scene of the incident.10 The JDHA is performed by senior members of the emergency services prior to implementing the emergency disrobe and decontamination process. The IOR includes an emphasis on the importance of effective communication for the success of emergency disrobe and decontamination. Responders should seek to foster public trust and confidence by communicating what they know about the incident, why and how casualties need to be disrobed and decontaminated, providing demonstrations of disrobe and decontamination when practical and encouraging mutual assistance. These communication strategies are likely to improve the efficiency and experience of undergoing disrobe and decontamination for affected casualties.24
Guidance assumptions and limitations
The following guidance makes the assumption that established procedures for identifying and responding to a chemical incident have been implemented. For example, the ‘STEP 1-2-3 PLUS’ protocol for determining the appropriate response and the ‘METHANE’ situation report for communicating information back to control centres.10 It is imperative that emergency responders maintain an awareness of the situation and do not put their own safety at risk. It is also important to note that the following protocols relate to casualties who are able to understand and perform instructions: guidelines for non-ambulant casualties are currently under development. The IOR guidance reported here is specifically for dealing with non-corrosive, liquid chemical contamination and not powders or biological/radiological contamination.
The IOR disrobe and dry decontamination protocol
The mnemonic ‘EMERGENCY’ may provide an aide-mémoire for the disrobe and dry decontamination protocol (table 1).
The salient features of the disrobe and dry decontamination process are available in video format produced by the National Ambulance Resilience Unit and NHS England.25 A pictogram demonstrating the dry decontamination process is presented in figure 4. The dry decontamination stage can be repeated (subject to availability of absorbent material) until MDUs become available. This will help to engage and focus casualties and will further improve decontamination effectiveness.

Pictogram demonstrating the blot and rub method for performing dry decontamination on casualties with scalp hair. Following disrobe, use a ‘blot then rub’ technique to apply the decontamination material. Clean the face first to remove contamination from around the eyes, nose and mouth. The hands should be cleaned next, followed by any other skin areas that may not have been initially protected by clothing. Head hair should be contaminated last, as hair provides a high degree of protection against chemical contaminants. Repeat steps 3–6 as necessary. Use clean decontamination material for each step (if available in sufficient quantity). Used decontamination material should be placed by the casualties into a suitable waste receptacle (eg, clinical waste bag and bin liner) immediately after use. Casualties with no appreciable head hair should be instructed to decontaminate the scalp skin immediately after the face, using clean decontamination material.
The SOR disrobe and wet decontamination (‘ORCHIDS’) protocol
The ‘ORCHIDS protocol’ is designed for use in MDUs that may be deployed by the fire and rescue service at the scene of an incident or available at designated NHS hospital EDs. Such units generally comprise a three-chamber tent (disrobe, shower and rerobe areas), a boiler pump (to deliver warm shower water), sump pumps (to remove waste water from within the MDU) and may also include warm air blowers (for heating), bund tanks (to collect waste effluent) and the provision of ‘re-robe’ packs.7 26 It is important to note that MDUs do not normally incorporate air handling units and so adequate steps to maintain good ventilation should be taken to prevent the accumulation of gas, vapours and aerosols during and after use by casualties. It is essential that MDUs and designated operators are regularly exercised to maintain a state of readiness. The ORCHIDS protocol is twice as fast as the previous (Model Response) method but at least as effective.27
In the case of exposure to non-caustic liquid contaminants, casualties should undergo disrobe and dry decontamination before proceeding to wet decontamination. This will reduce or eliminate the risk associated with the wash-in effect, where the dermal absorption of certain chemicals may be significantly enhanced by the presence of water, particularly organophosphorus compounds28 and sulfur mustard.29
Following disrobing (if casualties are still clothed), the ORCHIDS showering protocol follows the ‘WASHED’ mnemonic (table 2).
A final consideration is the finite capacity for rerobing within MDUs. Use of the shorter ORCHIDS protocol may cause a ‘bottleneck’,30 so plans should be in place to provide additional areas for casualties to rerobe.
Dry or wet decontamination?
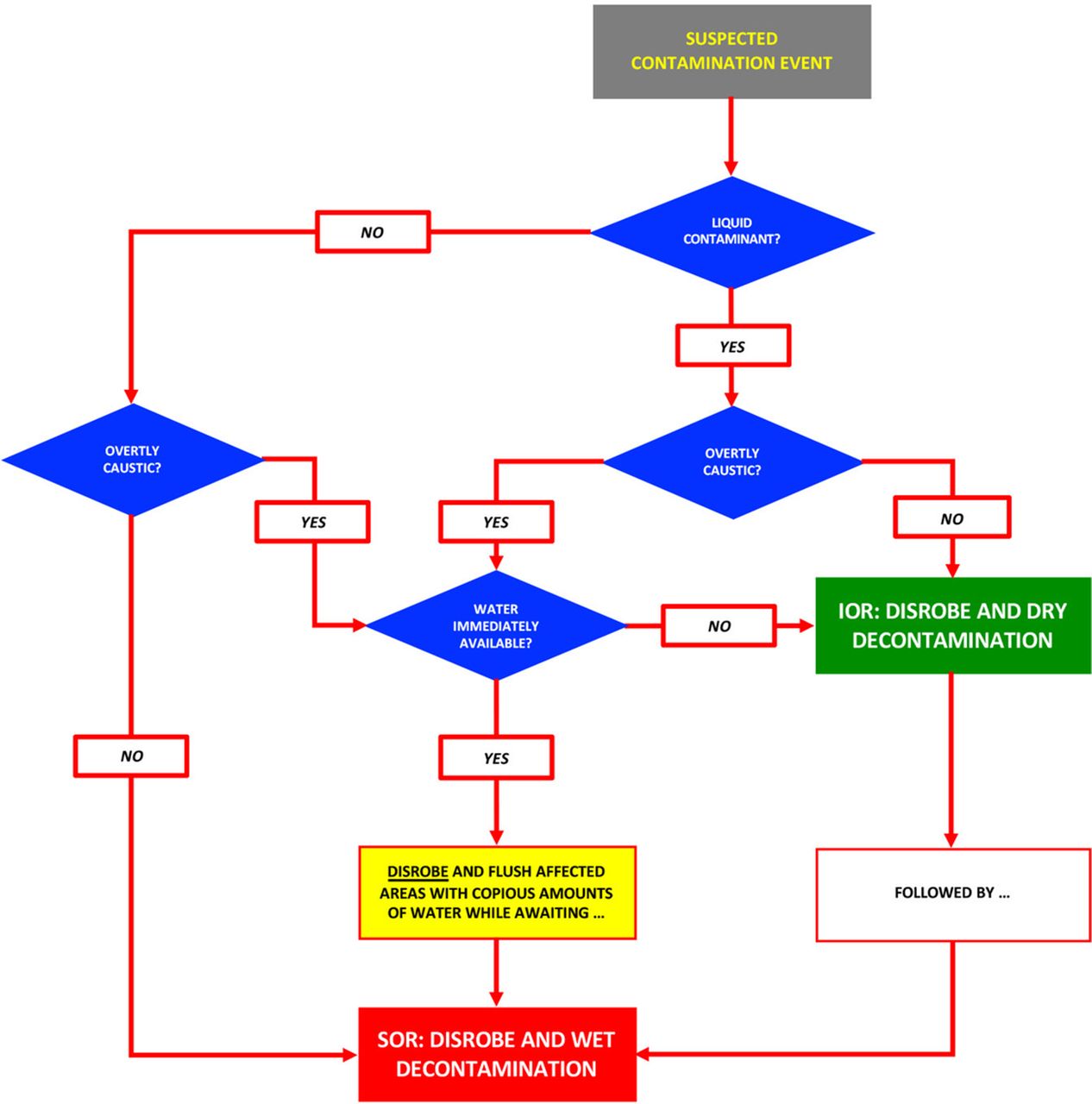
To reiterate, dry decontamination of liquid chemicals is at least as effective and is generally safer than wet decontamination. Therefore, dry decontamination should be the default incident response option. However, there are certain circumstances where wet decontamination may be preferable. A decision flowchart (eg, figure 5) can be used to determine the most appropriate course of action. It can be readily ascertained from the flow chart that any non-corrosive liquid contaminant (such as sulfur mustard, all nerve agents or solutions containing pesticides or cyanides and so on) should be treated by dry decontamination. The use of any form of wet decontamination (including the standard NHS ‘rinse-wipe-rinse’ method) for such materials is contraindicated due to the potential for enhanced dermal absorption. In contrast, solid forms of toxic, radioactive or biological contaminants should be subject to wet (SOR) decontamination. The only scenario that does not follow this simple binary decision process is exposure to corrosive liquids (eg, strong acids or oxidising agents), where disrobe and immediate flushing of affected areas with any available source of water is an urgent requirement. However, if water is not immediately available, disrobing and dry decontamination should be performed to reduce dermal exposure.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Basic flow chart for determining the appropriate response for managing contaminated casualties. IOR, initial operational response; SOR, specialist operational response.
Hair contamination
While wet and dry decontamination may reduce or eliminate the risk of a secondary contact hazard, some contaminants may diffuse into the hair fibres. This could potentially limit the effectiveness of decontamination and may provide a reservoir for subsequent evaporation (‘off-gassing’). In such instances, removal of contaminated hair should be considered to ensure the safety of casualties and medical staff.
Non-ambulant decontamination
The new IOR and SOR processes described above have been developed specifically for ambulant casualties, that is, individuals who can both understand instructions and perform self-decontamination with minimal assistance. Work is currently in progress to develop optimised methods for dry and wet decontamination of non-ambulant casualties.31
Summary
The UK is in the process of implementing a modified response to CBRN and HazMat incidents that introduces an IOR to complement the SOR. The IOR provides a capability for the rapid disrobe and dry decontamination of chemically contaminated casualties and thus provides an early, practical and effective clinical intervention while the arrival of specialist resources is awaited. For all incidents involving exposure to non-corrosive liquid contaminants, dry decontamination is the default response protocol.
Acknowledgments
The authors wish to thank the following government departments and agencies for their sponsorship of the original research projects: Department of Health (England), European Union (Executive Agency for Health and Consumers), UK Home Office and US Department of Health and Human Services (Office of the Assistant Secretary for the Preparedness and Response, Biomedical Advanced Research and Development Authority).
Footnotes
Contributors All authors contributed to the writing of this review article.
Funding The original research projects described in this practical review article were sponsored by the Department of Health (England), European Union (Executive Agency for Health and Consumers), UK Home Office and US Department of Health and Human Services (Office of the Assistant Secretary for the Preparedness and Response, Biomedical Advanced Research and Development Authority).
Disclaimer The opinions expressed in this article are those of the authors and do not necessarily reflect the policies, opinion or guidance of the UK or US governments.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.