Article Text

Statistics from Altmetric.com
Clinical introduction
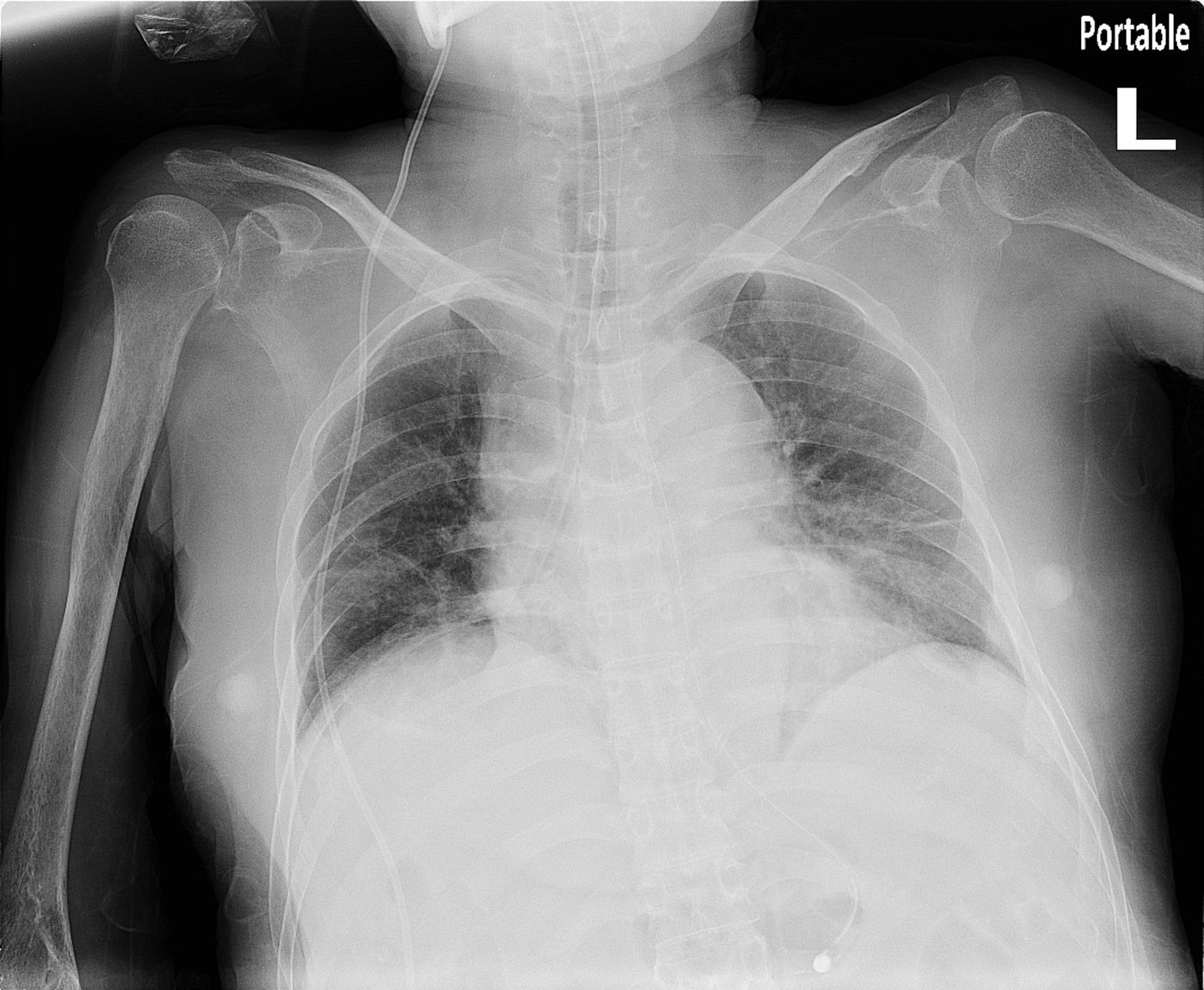
A 57-year-old woman nursing home patient with diabetes, hypertension, and a prior haemorrhagic stroke presented to our emergency department with progressive dyspnoea, cough with white sputum and low-grade temperature. On arrival, the patient was tachypnoeic, using accessory muscles and oxygen desaturation was noted. Physical examination showed no jugular vein engorgement, trachea was not deviated and auscultations revealed bilateral equal breath sounds with bi-basilar rales. Despite supplemental oxygen, the patient required intubation and was admitted to the intensive care unit (ICU). However, in the ICU, the patient’s saturation continued to fluctuate despite varying ventilation settings. The postintubation X-ray is shown (figure 1).

Postintubation X-ray.
Question
What is the most likely cause of respiratory failure in the patient?
Pulmonary oedema.
Pneumonia.
Pneumothorax.
Foreign body aspiration.
Answer: D
The foreign body was missed until the next day when the visiting ICU attending doctor reviewed the chest X-ray, The duty pulmonologist was immediately consulted and the foreign body was promptly removed from the right bronchus. The foreign body was later found to be a suction tube (figure 2) used by the nursing home, which we suspected had broken off at some point for unknown reason.

{kind=link}
{kind=link}
Foreign body indicated with a circle.
The foreign body might not have been missed if the physicians had used a standardised method of reviewing the X-ray. The ABCDEFGHI1 mnemonic is very useful: A stands for assessment of quality and airway. The X-ray here was a supine AP view, with poor inspiration of only six posterior rib visible, and reviewing the airway, there was no tracheal deviation, the endotracheal tube was in place but a suspicious object could be seen in the right bronchus. The rest of the mnemonic would be: B for bones and soft tissue (no bone fractures and no subcutaneous air). C for cardiac silhouette, D for diaphragm, E for effusion, F for fields, fissure and foreign body, (pneumonia, pulmonary oedema and pneumothorax) are not seen but there are three foreign bodies: the endotracheal tube, VP shunt and again, one in the right bronchus, G for gastric bubble and great vessels, H for hila and mediastinum and lastly I for impression. Using this standardised approach, we would have a greater chance of identifying the foreign body and thus provide more timely management for the patient.
Reference
Footnotes
Contributors All authors contributed equally.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.