Article Text

Abstract
Background Refugee children and young people have complex healthcare needs. However, issues related to acute healthcare provision for refugee children across Europe remain unexplored. This study aimed to describe the urgent and emergency healthcare needs of refugee children in Europe, and to identify obstacles to providing this care.
Methods An online cross-sectional survey was distributed to European healthcare professionals via research networks between 1 February and 1 October 2017 addressing health issues of children and young people aged <18 years fulfilling international criteria of refugee status, presenting to emergency departments. Survey domains explored (1) respondent’s institution, (2) local healthcare system, (3) available guidance and educational tools, (4) perceived obstacles and improvements required, (5) countries of origin of refugee children being seen and (6) presenting signs and symptoms of refugee children.
Results One hundred and forty-eight respondents from 23 European countries completed the survey, and most worked in academic institutions (n=118, 80%). Guidance on immunisations was available for 30% of respondents, and on safeguarding issues (31%), screening for infection (32%) or mental health (14%). Thirteen per cent reported regular teaching sessions related to refugee child health. Language barriers (60%), unknown medical history (54%), post-traumatic stress disorder (52%) and mental health issues (50%) were perceived obstacles to providing care; severity of presenting illness, rare or drug-resistant pathogens and funding were not.
Conclusions Many hospitals are not adequately prepared for providing urgent and emergency care to refugee children and young people. Although clinicians are generally well equipped to deal with most types and severity of presenting illnesses, we identified specific obstacles such as language barriers, mental health issues, safeguarding issues and lack of information on previous medical history. There was a clear need for more guidelines and targeted education on refugee child health.
- paediatrics
- emergency department
- global health
- mental health
- infectious diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this subject
Over the last few years, we have seen an increase in numbers of refugee children and young people entering the European Union, and they often arrive with complex healthcare needs.
Limited data exist detailing the acute healthcare needs of and acute healthcare provision for refugee children and young people across Europe.
What this study adds
This survey study amongst 148 respondents from 23 European countries showed a lack of preparedness for looking after refugee children and young people in urgent and emergency care. We identified obstacles which included language barriers, mental health issues, safeguarding issues and lack of information on medical history.
More guidelines and specific training on refugee child health are needed, with a focus on mental health issues, safeguarding, infectious disease screening and immunisations.
Introduction
Recent years have seen an increase in refugees entering the European Union. These refugees are often fleeing to an unfamiliar environment and they are at their most vulnerable after generally hazardous journeys. Addressing the healthcare needs of this refugee patient group poses challenges medically, politically and socially. Approximately one-third of these refugees are children and young people under the age of 18, many of them unaccompanied.1
Limited data exist on the healthcare needs of refugee children and young people, and the data mostly represent cohorts from refugee camps or selected populations such as children with rare and drug-resistant infectious diseases.2 3 A survey among primary care paediatricians highlighted the complexity of providing healthcare to refugee children, emphasising cultural and linguistic factors, a higher prevalence of chronic diseases, and a lack of guidance and educational resources.4 Several national and international child health societies have published statements on performing health assessments for refugee children.5–10 However, issues related to acute healthcare provision are poorly addressed and the existing guidance does not always account for the differences between health systems across Europe. It is, therefore, unknown what obstacles exist to providing urgent and emergency care to these vulnerable patients.
Understanding the preparedness of emergency care facilities to provide healthcare to refugee children and young people is essential in order to develop clinical guidance and training for front-line healthcare professionals. To inform these, it is important to understand how refugee children and young people present to emergency care facilities, what resources may be required to provide appropriate healthcare and any obstacles to doing so. This survey study, therefore, aimed to explore current practices and evaluate obstacles in urgent and emergency care of refugee children and young people across Europe, underpinned by a review of existing relevant guidance.
Methods
Study design
An online survey was distributed via the Research Electronic Data Capture (REDCap) platform between 1 February and 1 October 2017.11 Potential participants were identified from the membership of national and international healthcare Colleges, Associations and networks including the Research in European Paediatric Emergency Medicine (REPEM) network, Paediatric Emergency Research in the UK and Ireland network,12 the Red de Investigación de la Sociedad Española de Urgencias de Pediatría/Spanish Paediatric Emergency Research Group network, the European Society of Paediatric Infectious Diseases (ESPID) and the Royal College of Paediatrics and Child Health (RCPCH). Participating REPEM member institutions were asked to distribute among other hospitals in their region not affiliated to the REPEM network. Each participating institution provided one response, completed by the most appropriate person with local knowledge of urgent and emergency care delivery to refugee children.
Survey development
The survey was developed according to best practice on survey methodology and iteratively by the study team, with input from clinical experts and the REPEM research committee.13 Prior to launch it was piloted in two hospitals (Germany and UK) for feedback and checking of hyperlinks. Survey domains were chosen based on expert consensus, RCPCH guidance7 and a systematic search of four databases (Medline, Embase, Cochrane, PubMed) and national society websites to identify existing guidelines or other resources on refugee child health in Europe (online supplementary appendix 1).
Supplemental material
The survey collected data related to urgent and emergency care of refugee children (including unaccompanied minors) encompassing (1) respondent’s institution, (2) local healthcare system, (3) available guidance and educational tools, (4) perceived obstacles and improvements required, (5) countries of origin of refugee children being seen, (6) presenting signs and symptoms of refugee children and young people. The survey explored broader health-related items including infection screening and immunisations, mental health, sexual health, safeguarding and social issues, and acute somatic symptoms. The population being described were defined as children and young people aged up to 18 years fulfilling refugee status as outlined in the 1951 Geneva Convention relating to the Status of Refugees (article 1A(2))14 15 and who presented to emergency departments (EDs); respondents were told that data pertaining to immigrant children who had been in the country >5 years should not be included as these were not considered to fulfil refugee status for the purposes of this study. At all times, the survey domains highlighted that they addressed the urgent and emergency care, and not the planned healthcare, of refugee children and young people. In the questions relating to the volume of attendances to the ED, respondents were advised that recorded numbers were preferable if available, but that estimates were acceptable.
Response options included, where appropriate, 5-point Likert-scale, multiple selections, single answer or free text. The survey also provided the option of uploading guidelines or other relevant documents; these data were stored in a secure database at the hosting universities and will be made available at request. The full survey is available in online supplementary appendix 2.
Supplemental material
Analysis
All descriptive analyses were performed using SPSS V.24, IBM. Results are presented as numbers and proportions for categorical variables, and means or medians (with SD or IQR) for continuous variables as appropriate. Differences in categorical variables between groups were calculated using the X2 test, with Fisher’s exact test used to account for cells with less than five cases. To better understand differences in preparedness between institutions, we performed subgroup analyses for institutions seeing >100 refugee children and young people per year versus institutions seeing <100 or nil refugee children and young people per year in their urgent and emergency care facilities.
Patient and public involvement
This study was developed in collaboration with experts (ie, general practitioners, family doctors and paediatricians) from Refudocs, a non-profit medical organisation based in Munich, Germany, which was founded in view of the increase in numbers of refugees into Germany in 2014 and which is dedicated to healthcare issues of refugees and asylum seekers. They provided feedback on the questionnaire and recruitment process, on a voluntary basis. No patients were directly involved in the design of this study.
Results
Respondents’ settings
One hundred and fifty-three surveys (75% of 204 which were started) contained sufficient data for analysis; five responses from outside Europe were excluded (figure 1). Responses came from 23 European countries; just over half of these responses came from three countries: the UK (47 responses), Spain (21 responses) and Germany (13 responses). Seven respondents worked outside hospital settings, of whom three worked in refugee healthcare services. The remaining 141 respondents were from 117 unique hospitals from 20 countries. Response rates varied for the different domains of the survey. We were unable to estimate accurate response rates for the various networks in which the survey was distributed due to methodological limitations; these limitations included issues of respondents being members of multiple networks, difficulties with determining the total number of institutions represented by the membership of various networks and the inability to calculate the precise number of members fulfilling criteria of the targeted group of respondents.

Overview of respondents in Europe.
Most respondents were consultant physicians (n=117/148, 79%) and most hospital-based respondents worked in tertiary medical centres (n=118, 84%) (table 1). Most often (n=104/117, 89%), children and young people were seen in (paediatric) EDs for their acute health problems; in a minority of hospitals this occurred in other clinical areas such as outpatient clinics or inpatient wards (table 2). The estimated number of refugee children and young people seen in emergency care ranged from none to >500 per year between institutions (table 2).
Overview of respondents and their institutions (total n=148)
Overview of current healthcare delivery systems of respondents
Local healthcare delivery systems
Urgent and emergency care was mostly provided by consultants and trainees in paediatrics and paediatric emergency medicine (table 1). Planned point of entry health screening occurred mainly in public health facilities (n=28/95, 29%), but no screening was undertaken in 25 instances (27%) (table 2). In several settings, other organisations provided healthcare to refugee children (57/103, 55%). Few respondents took part in regular discussions with public health organisations regarding refugee child health (n=17/97, 18%) (table 2).
Available guidance and educational tools
A majority agreed guidelines were needed to support health professionals dealing with refugee children (n=77/108, 71%) (figure 2). Only a minority of respondents had guidelines in place (table 2): immunisations and catch-up immunisation schedule (n=37/125, 30%), infection screening (n=40/125, 32%), safeguarding concerns and social care referral (n=38/125, 31%), mental health issues and symptoms of post-traumatic stress disorder (PTSD) (n=17/125, 14%) and managing refugee children in emergency care (n=22/125, 18%). Only a few institutions had regular teaching sessions on refugee child health (n=13/97, 13%). Available guidance identified in our systematic search, as well as documents uploaded by our respondents are provided in table 3 and online supplementary appendix 1.

Statements on needs for providing urgent and emergency care to refugee children and young people in hospitals. Statements on needs for providing urgent and emergency care to refugee children and young people in hospitals. Respondents were asked to indicate (on a 5-point Likert scale) to which degree they agreed with the posed statements.
Overview of (national) guidelines in Europe6–10
Perceived obstacles for providing urgent and emergency care to refugee children and young people
Of 110 responses to this section, the obstacles most frequently identified were language barriers (n=66, 60%), not knowing medical history (59, 54%), managing PTSD (n=57, 52%), mental health (n=55, 50%) and providing appropriate safety netting information (n=52, 47%) (figure 3, online supplementary appendix 3). Severity of illness (n=5, 5%), rare or drug resistant pathogens (n=14, 13%) and funding (n=22, 20%) were perceived as obstacles among less than one-fifth of the respondents.
Supplemental material
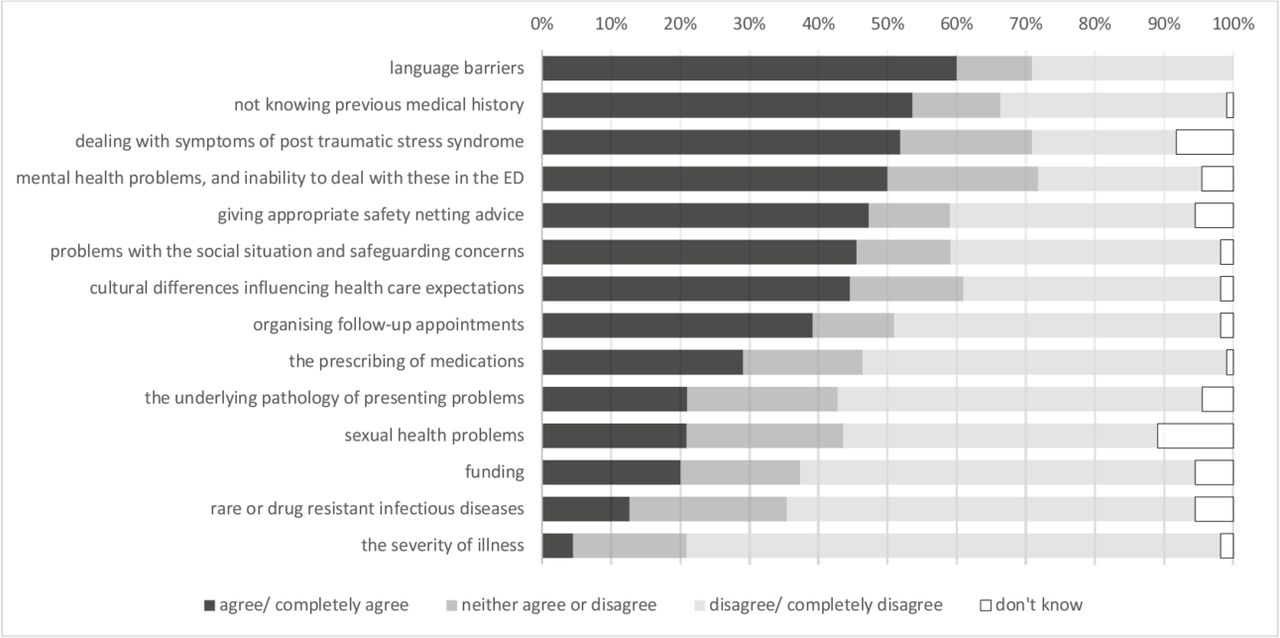
Perceived obstacles to providing urgent and emergency care to refugee children and young people in hospitals. Perceived obstacles to providing urgent and emergency care to refugee children and young children in hospitals. Respondents were asked to indicate if specified items were perceived as obstacles for providing urgent and emergency care to refugee children (on a 5-point Likert scale). ED, emergency department.
Statements on refugee child health needs
Views from 108 respondents on preparedness to meet healthcare needs of refugee children were split, with one-third (n=40, 37%) of respondents declaring a high level of readiness, and a further third disagreeing (n=36, 33%) (figure 2, online supplementary appendix 3). A large percentage of respondents stated that caring for refugee children was not part of their daily activities (n=58, 53%). Respondents indicated the need for better training in associated social problems (n=92, 85% agreed/completely agreed), mental health issues (n=78, 73%), underlying medical problems (n=65, 60%) and associated sexual health problems (n=59, 55%). Preparedness for dealing with refugee children and young people was generally better in institutions that provided emergency care to this group of patients more frequently (online supplementary appendix 4).
Supplemental material
Presenting signs and symptoms
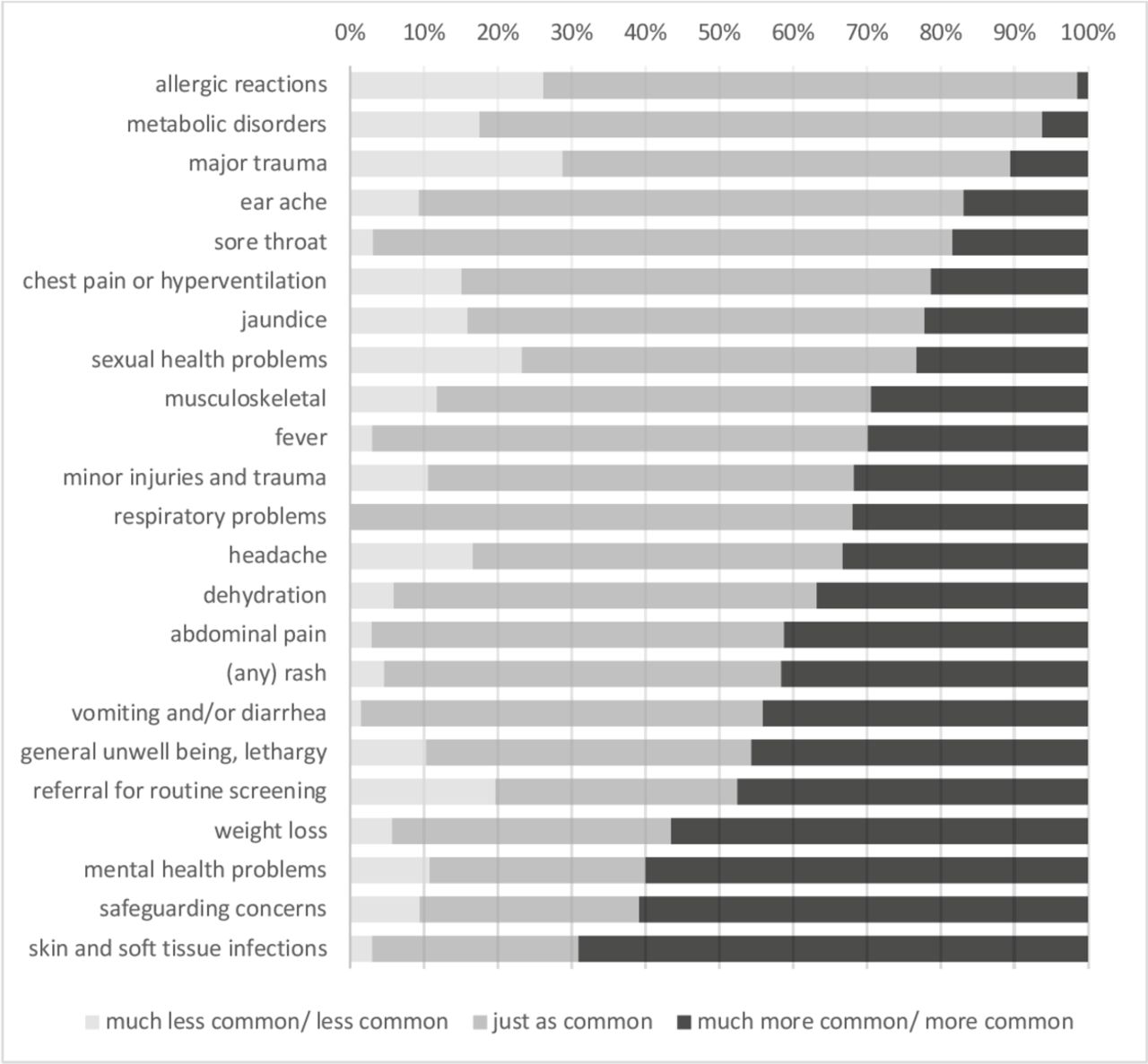
When asked if signs and symptoms were seen more or less commonly in refugee children in comparison with the local population, respondents indicated that skin and soft-tissue infections (mean score 3.78 on a 5-point Likert scale, SD 0.75), safeguarding concerns (mean score 3.64, SD 0.93), mental health issues (mean score 3.62, SD 0.95), and weight loss (mean score 3.58, SD 0.78) were seen more commonly in refugee children (figure 4, online supplementary appendix 3). Allergic reactions (mean score 2.71, SD 0.58) and major trauma (mean score 2.76, SD 0.84) had the lowest mean scores.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Presenting signs and symptoms of refugee children and young people to emergency care facilities. Respondents were asked if signs and symptoms were seen more or less commonly in refugee children and young people in comparison with the local population (on a 5-point Likert scale). Metabolic disorders: such as exacerbated type I Diabetes Mellitus, including ketoacidosis; musculoskeletal problems: non-traumatic, for example, limp, joint swelling, back pain; referral for routine screening: referral by other healthcare professional.
Discussion
Principal findings
Our survey with responses from 23 European countries describes the healthcare needs of refugee children and young people presenting to urgent and emergency care across Europe, and the obstacles to providing this care. In our sample, some respondents had a considerable caseload of refugee children and young people in their emergency care facilities, whereas others were not or infrequently exposed to the challenge of dealing with refugee children and young people in emergency care. In general, it appeared that emergency care clinicians were well equipped to deal with the majority of clinical problems they were confronted with, and that these were comparable to the clinical problems seen in the local population. Moreover, unusual clinical presentations, such as rare or drug resistant infectious diseases, were infrequent and were not perceived as a major obstacle in delivering urgent and emergency care. Common obstacles in providing this care included language barriers, safeguarding issues, mental health issues and the lack of available information on medical history. Our respondents indicated a need for guidelines and tailored education covering topics such infectious disease screening and immunisations, mental health, sexual health and social care issues.
Comparison with literature
There are few studies describing signs and symptoms of acute medical needs of refugee children in high-income countries.17 Aligned with our findings, reports from refugee camps suggest that type and severity of acute illness are similar to that experienced in non-refugee populations attending primary or secondary care.18 19 In particular, respiratory and gastrointestinal disease, nutritional deficiencies (eg, anaemia and vitamin D deficiency), and dental issues were often encountered.2 18 20 21 These problems are well within the clinical remit of emergency care clinicians to deal with. However, additional training might be needed for conditions encountered less commonly in non-refugee populations such as PTSD, varying types of injuries and infectious diseases such as tuberculosis (TB) and malaria.2 18 20 21
Healthcare needs of refugee children and young people are complex and multifaceted.22 For example, health assessment clinics reported high rates of mental health problems, sleeping disorders and sexual health issues.23 These will not always be straightforward to address in EDs, and will often need more structured and long-term healthcare solutions. However, many European countries do not provide for chronic and complex health issues in a structured or timely manner, and this care is often not funded by the government.24 25
A majority of presenting symptoms are related to infectious diseases,18 and the emergence of unusual and drug-resistant organisms in refugee and asylum seeking children has been reported.26 However, our data suggest that this is not a predominant problem in emergency care, but rather of more specialised hospital care and public health. Yet, the high reported rates of hepatitis B, active and latent TB and incomplete vaccination status in many of these children, raise the issue of screening for these infections and providing catch-up immunisations in emergency care facilities.27–29 Similarly, sexual health problems were not perceived as a major obstacle, whereas reproductive health issues, sexually transmitted diseases and sexual abuse, in particular among girls of reproductive age, are frequent,30 perhaps suggesting that some important problems are currently being underidentified in emergency care.
Strengths and limitations
While designing the survey, we set out to illustrate the current situation of managing refugee children and young people presenting to urgent and emergency care facilities across Europe. We, thus, aimed to collect a reliable and representative sample of respondents working in urgent and emergency care from across Europe. The sample of respondents from multiple centres in 23 European countries is testament to this, and gives a representative picture of the current situation including data not previously obtained. We chose to collect in-depth data from a clearly defined target population of respondents. As a result, this comprehensive survey might have proven too time consuming for some potential respondents, which is reflected in the number of respondents starting but not fully completing the survey. Our sample size was too small to perform additional subgroup analyses, and the stratified analysis to show differences in preparedness between institutions seeing high and low volumes of refugee children and young people showed trends, but yielded minimal statistically significant differences owing to small numbers. One major strength of this study is the endorsement by several international and national societies, ensuring relevant professional networks for distribution as well as additional quality control. The survey was accessible for a fairly long period of 8 months to allow for distribution among these networks. Notably, whereas recently published guidelines mainly relied on expert opinions and national healthcare polices,5 7 our survey is an attempt to present real-life data, hence substantiating our identified areas for improvement. Limitations of this survey include issues with representation and generalisation. A few countries were clearly over-represented while other areas were not represented. As with any survey, the data generated only reflect the actual responses, and are likely to represent a selected sample of physicians with a special interest in the topic. Moreover, our cohort mostly, yet not exclusively, included tertiary care clinicians, suggesting a selected sample of physicians most likely to be associated with international networks. Furthermore, one-quarter of the respondents worked in a hospital located in the vicinity of a refugee camp. This may have biased the results towards a better preparedness of the included emergency settings. Additionally, it proved difficult to report accurate response rates as a result of the involvement of multiple networks, which would have strengthened the validity of this study. Nevertheless, this work represents valuable and not previously published data in this area to date.
Implications for practice, health policy and future research
Our findings clearly demonstrate the need for improved guidance, educational tools and a platform for shared learning on managing refugee children and young people in urgent and emergency care. Currently, the sparsely available resources mostly apply to routine screening rather than emergency care.5 7 Thus, there lies an opportunity for international networks to work together on collating evidence and formulating best care recommendations for delivering urgent and emergency care. Major difficulties will be posed by the large variety in healthcare delivery systems and differences in healthcare funding. However, these difficulties should not interfere with an individual’s healthcare needs, independent of where refugee children will be seen and by which specialist. The availability of easily accessible translation services will be pivotal in this process of improving urgent and emergency care.31 32
Our results suggest that healthcare professionals need to collaborate with health policy makers in order to sustainably address the issues identified in this study. As a next step, prospective individual patient data on healthcare needs of refugee children and young people, for example, by means of a prospective European registry, are needed. A significant issue with such data collection will be traceability of patient identifiable data and the need for a consenting procedure. That said, our survey joins forces with only very few other studies in reporting original data on how refugee children are being cared for across Europe. Thus, these data may contribute to developing uniform guidelines in a process that will include opinion leaders, policy-makers and scientific societies in a joint endeavour to eventually improve and standardise care for refugee children in Europe.
Conclusion
Many hospitals are not adequately prepared for providing urgent and emergency care to refugee children and young people. We identified specific obstacles to providing care to this vulnerable group of patients such as language barriers, mental health issues, safeguarding issues and lack of information on medical history. This study offers an incentive for improving clinical guidance and education. However, care pathways vary greatly between different countries, making uniform guidance challenging, and requiring increased efforts for international collaborations between relevant policy-makers and medical scientific bodies.
Acknowledgments
Foremost, we would like to thank all respondents for their contributions. We are grateful to Mathias Wendeborn and other experts from RefuDocs for providing critical feedback on the survey design. We would also like to thank ESPID and its scientific committee, for awarding a small grant award and allowing distribution among its members. Similarly, we are thankful for the support of RCPCH, and in particular Angela Mensah, and several national societies in the UK and Ireland (PERUKI), Germany, and Spain (RISEUP-SPERG).
References
Footnotes
Handling editor Simon Carley
Twitter @rgnijman, @mdlyttle
Contributors RGN and UvB were responsible for the conception of the study, for obtaining funding, and writing of study protocol. JK was responsible for data collection and data analysis. SM, MDL, IKM and CB were responsible for scientific input, study design and the support and distribution across networks. RGN wrote the first draft of the manuscript, and was responsible for data quality control and data analysis. All authors have contributed significantly to the drafting and revising of the manuscript. All authors have approved the manuscript as submitted, and they are willing to take responsibility for the reported research. Main authors and guarantors of this paper are RGN and UvB.
Funding This project was awarded a small grant award by the European Society of Paediatric Infectious Diseases (ESPID). RGN was awarded an academic clinical fellowship (ACF-2015-21-016) and an academic clinical lectureship (CL-2018-21-007) in paediatrics funded by the National Institute of Health Research (NIHR), UK. UvB was awarded a clinical leave fellowship funded by the German Centre for Infection Research (DZIF), Germany.
Disclaimer The funders had no role in study design, data analysis, or decision to publish this manuscript. RGN and UvB had full access to all data.
Map disclaimer The depiction of boundaries on the map(s) in this article does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. The map(s) are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval This survey sought responses from healthcare professionals via collaborative networks and societies and did not contain any patient identifiable data; ethics approval was therefore unnecessary as confirmed by the Health Regulation Authority research decision tool.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplementary information. Requests for data sharing will be considered by the authors of this study: relevant and anonymised data can be made available on reasonable request to the corresponding author.
Press release Yes.