Article Text

Abstract
Background There has been a recognised trend of increasing use of emergency and urgent care and emergency departments (EDs) by older people, which is marked by a substantial evidence base reporting interventions for this population and guidance from key organisations. Despite this, outcomes for this population remain suboptimal. A plethora of reviews in this area provides challenges for clinicians and commissioners in determining which interventions and models of care best meet people’s needs. The aim of this review was to identify effective ED interventions which have been reported for older people, and to provide a clear summary of the myriad reviews and numerous intervention types in this area.
Methods A review of reviews, reporting interventions for older people, either initiated or wholly delivered within the ED.
Results A total of 15 review articles describing 83 primary studies met our content and reporting standards criteria. The majority (n=13) were systematic reviews (four using meta-analysis.) Across the reviews, 26 different outcomes were reported with inconsistency. Follow-up duration varied within and across the reviews. Based on how authors had reported results, evidence clusters were developed: (1) staff-focused reviews, (2) discharge intervention reviews, (3) population-focused reviews and (4) intervention component reviews.
Conclusions The evidence base describing interventions is weak due to inconsistent reporting, differing emphasis placed on the key characteristics of primary studies (staff, location and outcome) by review authors and varying quality of reviews. No individual interventions have been found to be more promising, but interventions initiated in the ED and continued into other settings have tended to result in more favourable patient and health service outcomes. Despite many interventions reported within the reviews being holistic and patient focused, outcomes measured were largely service focused.
PROSPERO registration number PROSPERO CRD42018111461.
- emergency care systems
- emergency departments
- geriatrics
Statistics from Altmetric.com
Key messages
What is already known on this subject
Emergency department (ED) care for older people can be complex. Those people living with frailty have poorer health outcomes.
Caring for increasing numbers of older ED attendees is a critical health service issue.
Numerous interventions have been trialled within emergency and urgent care.
What this study adds
Description and appraisal of healthcare interventions is inconsistent and therefore difficult to synthesise.
No individual intervention was found to be more beneficial for older people with emergency care needs.
Interventions initiated in the ED and continued into other settings tended to result in improved outcomes.
Most studies reported service metrics rather than person-centred outcomes.
Introduction
Background
Use of emergency and urgent care (EUC) and emergency departments (EDs) by older people is increasing. This has been variously attributed to the complex physical, social and mental health comorbidities that older people often live with, changes in the healthcare options available to patients, professional opinions on appropriate treatment and the capacity of individual care systems. Caring for those older people living with frailty presents an urgent national and international public health issue. Despite guidance developed by organisations such as the British Geriatrics Society, the Royal College of Emergency Medicine, the American College of Emergency Physicians, and the International Federation of Emergency Medicine, fast-flowing EUC systems are yet to fully integrate person-centred case management designed to best meet the needs of older people.1 Existing reviews report a large body of evidence describing interventions for this population. However, there is a need to identify consistent messages around proposed approaches to older people’s care in the ED, to ensure that care is sensitive, effective and efficient, encompassing individuals’ clinical and wider social needs. This study aimed to review the evidence for ED interventions for older people and the characteristics of that evidence base, in particular, the overlap in primary study coverage between reviews, the outcomes reported within reviews and the consistency of intervention reporting. The study aimed to identify whether the literature demonstrated any evidence of intervention effectiveness and to identify which ED interventions best meet the needs of older people.
Methods
A review of reviews (‘overview’) of systematic and non-systematic reviews was undertaken, including both qualitative and quantitative studies. This method was chosen due to the number of existing reviews in this field.2 3 Reviews of reviews offer benefits in that they ‘enable broader evidence synthesis questions to be addressed in a faster time frame’.4 In October 2018, the protocol was published on the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42018111461). The review was conducted and reported according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards.5
Inclusion criteria
Reviews were appraised for eligibility against pre-defined inclusion criteria. Criteria for reporting standards were based on the Cochrane Handbook definition of a systematic review and criteria developed by Brunton in Pollock.6 Reviews which met all of the inclusion criteria and three or more reporting standards criteria were included. These criteria are included in online supplemental material 3.
Supplemental material
Search approach
A comprehensive database search used existing strategies7 combining terms for EUC and for older people, limited by publication type (reviews), language (English Language studies only) and date (2000–2018). The search strategy for Medline (OVID SP) was developed by an information specialist and is reproduced in online supplemental material. This was adapted for other databases: Embase (OVID SP), CINAHL (EBSCO), Cochrane Library (Wiley Interscience), Web of Science Core Collection (Clarivate), SCOPUS (Elsevier) and AgeINFO (http://www.cpa.org.uk/). Further review sources were searched using an adapted database strategy: Joanna Briggs Institute (https://journals.lww.com/jbisrir/Pages/default.aspx), the Campbell Collaboration (https://campbellcollaboration.org/), Epistemonikos (https://www.epistemonikos.org/) and PROSPERO (https://www.crd.york.ac.uk/PROSPERO/). In addition, we undertook forward and backward searching of included reviews using reference lists and Google Scholar for citation identification. Topic experts were consulted to identify missing reviews. A search alert was set up to identify additional reviews published following the database searches.
Study selection
References were managed in Endnote V.8. Duplicates were removed prior to screening for inclusion at title and abstract level. This was undertaken by one first reviewer (JDvO or LP), with 50% from each first reviewer also screened by a second reviewer (SA). All remaining potentially eligible reviews were double screened at full text by LP and SPC. Reasons for excluding reviews were recorded. Figure 1 presents a PRISMA for Scoping Reviews flow chart of searching and study selection.
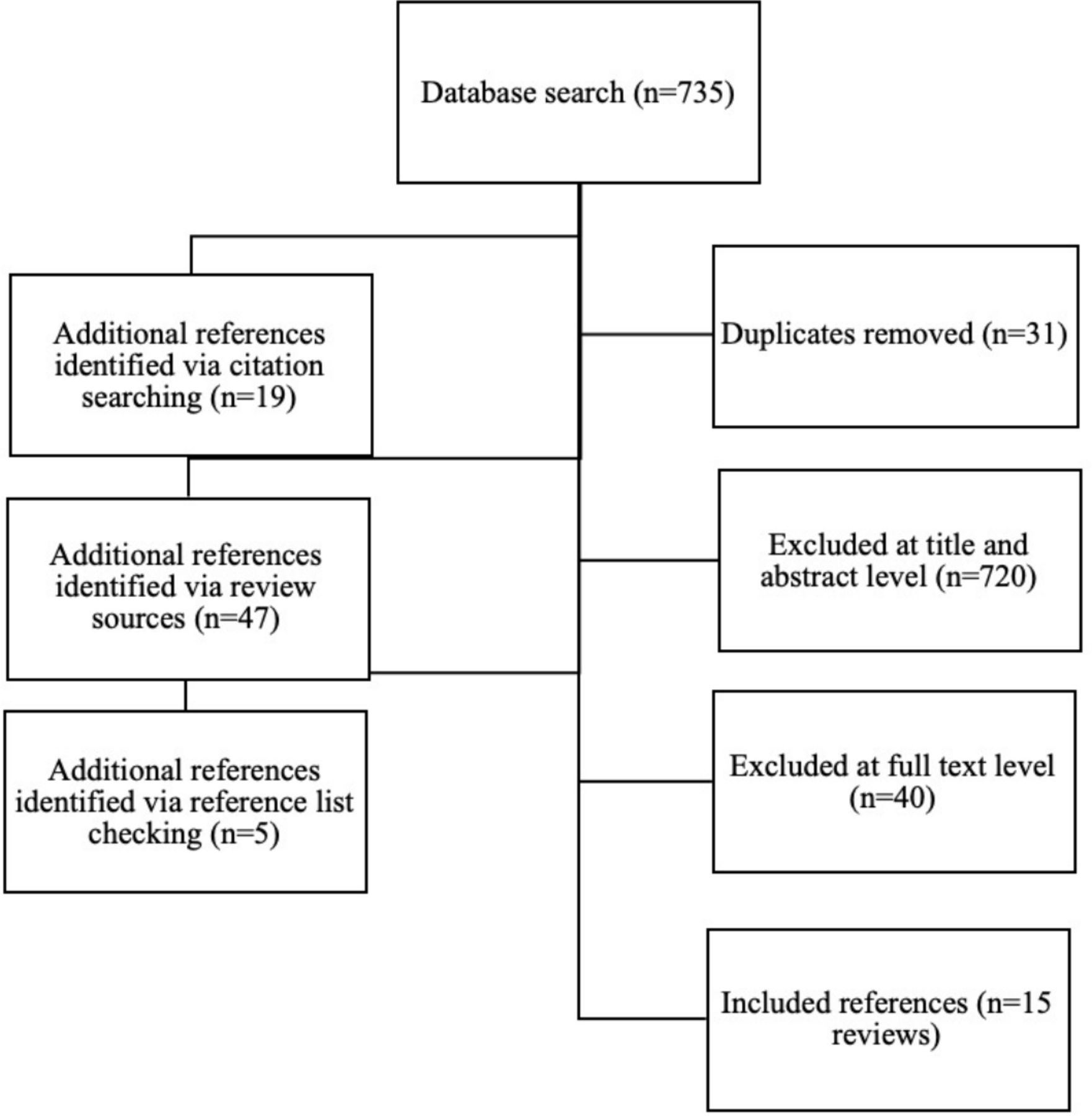
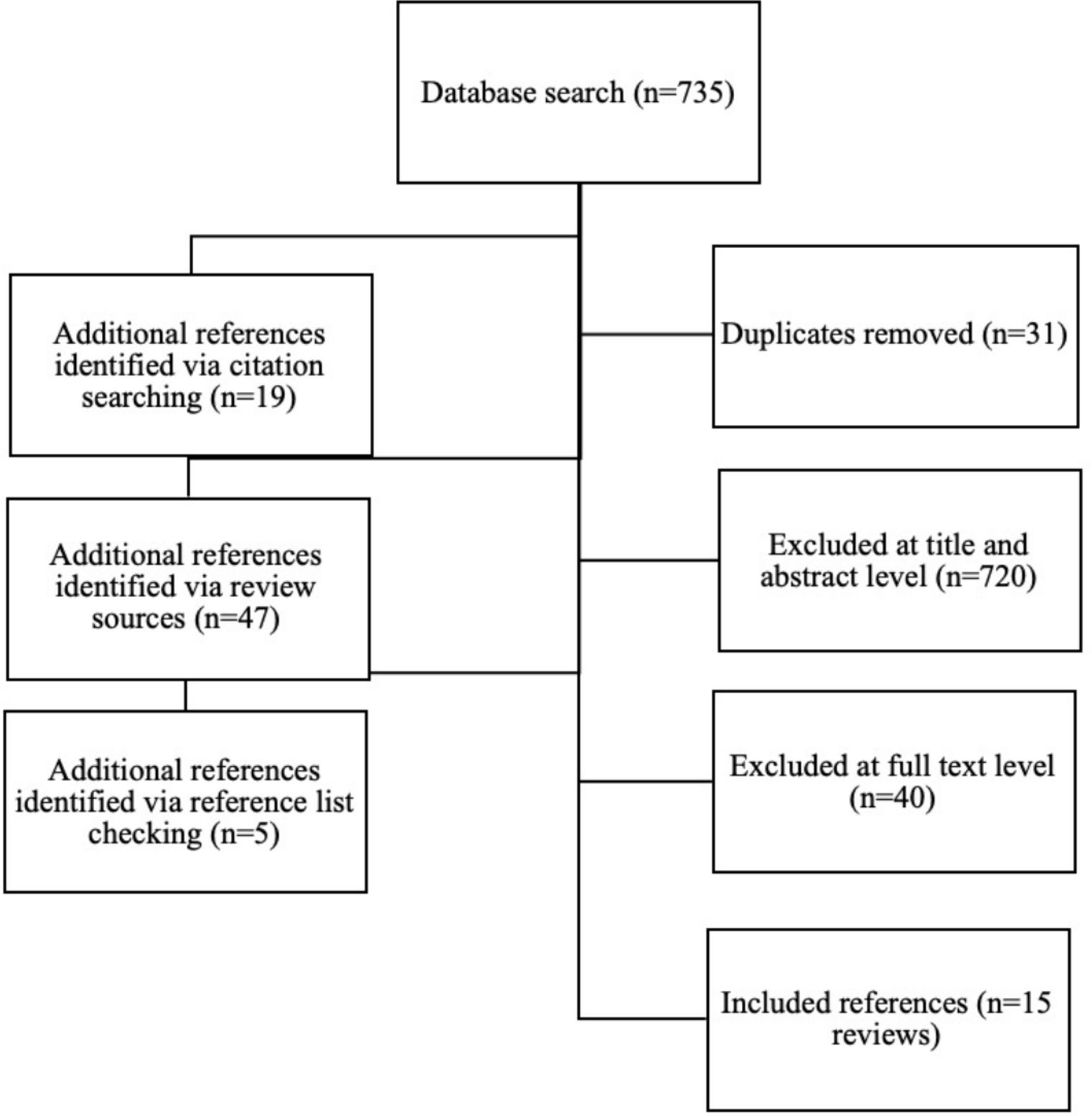{kind=link}
PRISMA-SR flow chart. PRISMA-SR, Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews.
Data extraction and quality assessment
A data extraction sheet was designed in Microsoft Excel by LP and iteratively refined following piloting by SA and JDvO. Data were single extracted by one reviewer (LP, SA or JDvO). LP subsequently checked all extractions and a random sample of 10% were also checked by SA. Data were extracted on review type, review methods, description of included studies, all reported outcomes (including whether they had been synthesised or reported as individual studies) and a headline message or conclusion. We used the AMSTAR2 checklist (online supplemental material 1) to assess the quality of reviews. AMSTAR2 allows the appraisal of reviews that include non-randomised studies of interventions, in addition to randomised controlled trials (RCTs).8 The findings from our quality assessment are reported narratively.
Overlap within reviews
A citation matrix was drawn up.9 This matrix assessed overlap in the evidence base by mapping each included review against all cited primary studies.
Data synthesis
Extracted data were summarised and presented in tables with a narrative synthesis. Due to the heterogeneity between reviews, no further statistical synthesis was undertaken.
Patient and public involvement
Public involvement in the review of reviews was managed through the overall research project, of which the review was one workpackage. Patient experience of the ED informed the overall research questions and design of the study and continue to be involved in the overall project, including dissemination plans.
Results
Overview
A total of 806 articles were retrieved . From these, 15 eligible reviews were identified, published 2005–2019. These 15 reviews reported 83 unique primary studies (published 1994–2018). Of these 83 studies, 25 were included in more than one review, with the most frequently cited primary study included in 11 reviews.10 The review characteristics are presented in table 1. Quality assessment is summarised in online supplemental material 2.
Review characteristics
Population definitions
Most reviews defined older people as being aged over 65, although some11 ,12 included papers with populations aged 60 and older. Some reviews did not report a specific age, but rather reported interventions for participants who were ‘older’ or ‘elderly’. The majority of reviews reported ED care for a general population of older people, who were not stratified by condition or severity. However, Lowthian et al 13 included a population of ‘high risk’ participants; this may indicate that there was some prior screening of patients before they were included in the intervention.
Outcome measures
Table 2 lists all outcomes reported in the 15 included reviews, organised according to Parker et al.14 There was inconsistency in the reporting of outcomes between reviews. Some reviews synthesised papers by outcome measures. There was a clear preference to measure outcomes in terms of service delivery metrics as opposed to patient centred outcomes. Other reviews did not synthesise outcomes across included studies but reported these narratively on an article-by-article basis. There was a high level of variability in the length of patient follow-up from 0 days to 18 months. To some extent this depended on whether the intervention was wholly delivered in the ED or continued into other settings.
Outcomes
Intervention classification
Reviews of ED interventions were organised into four evidence clusters:(table 3) discharge intervention reviews,12 13 15–17 staff-focused reviews,11 18–21 population-focused reviews22 23 and intervention component reviews.23–25 Only 5 of the 15 reviews reported interventions delivered wholly within the ED—the remainder were continued into other settings.
Intervention cluster characteristics
Discharge intervention reviews
The reported discharge interventions included postdischarge follow-up of patients by ED or community-based care professionals, although these were often reported incompletely.
Conroy et al 15 reported interventions delivered within 72 hours of ED attendance. These were comprehensive geriatric assessment (CGA) interventions delivered either by nurses or geriatricians and were targeted at older people with frailty. The review by Hastings et al 16 looked at evidence for interventions to improve outcomes for older people discharged from the ED. Fourteen of the studies reported by Hastings and Heflin16 were of interventions either initiated or concluded in the ED. A wide variety of interventions were reported, from CGA to single screening and assessment interventions, delivered by single practitioners or multidisciplinary teams. Karam et al 17 limited inclusion criteria to interventions delivered within the ED and including CGA and other intervention types. Lowthian et al 13 reported on discharge interventions in the form of Community Transition Strategies from the ED. All of these strategies included geriatric assessment, but this was undertaken by a variety of professional groups including nurses, allied health professionals, and health visitors. Follow-up interventions either consisted of referral to community services or direct linkages including telephone/general practitioner follow-up. Nine of the 18 primary studies included in the review of interventions to reduce ED visits by McCusker and Verdon12 were delivered in the ED; all had an ED and post discharge component.
Outcomes were reported using meta-analysis15 ,13 and narrative synthesis.12 16 17 Conroy et al 15 found no clear evidence of benefit for CGA discharge interventions across all outcomes included in the review. Hastings and Heflin16 reported at the level of individual studies only across a wide variety of outcomes. Karam et al 17 developed themes for intervention types (referral, follow-up, integrated model of care) and identification of study participants (risk screening or no risk screening). They found that the most effective interventions extended beyond referral and used a clinical risk prediction tool to identify those who would most benefit from the intervention. In the review by Lowthian et al,13 four of the nine studies were included in a meta-analysis, which found no benefit of interventions in terms of ED reattendance, mortality and emergency hospitalisation. Individual studies were effective in reducing ED reattendance and nursing home admissions—Lowthian et al 13 attributed this potentially to the methods of telephone follow-up of discharged patients. The review by McCusker and Verdon12 found that there was limited evidence of benefit of discharge interventions (two studies of borderline statistical significance) on ED visits and there was evidence of short term only increase in ED visits as a result of the intervention.
Summary—Discharge interventions varied in their components but tended to employ improved linkages between the ED and the community, either through direct linkage or referral interventions. CGA was frequently used and involved a variety of professional groups. There was limited evidence for the effectiveness of these interventions—two meta-analyses found no benefit to these interventions, and narrative synthesis reported an increase in ED readmissions in the short term among patients who had received these interventions.
Staff-focused reviews
Interventions were generally delivered by ED physicians, geriatricians working within the ED, and nurses with or without an advanced role. There was also evidence of wider MDT led interventions in a number of reviews,12 13 16–19 22 26 where professionals included research assistants, occupational therapists, discharge coordinators, social workers, physiotherapists and health visitors. Study outcomes were reported narratively and using meta-analysis. There was moderate but inconsistent agreement across the studies for the effectiveness of nurse led interventions.
Fealy et al 11 described 11 nurse-led interventions which included assessment, postdischarge referral, patient education and follow-up. Five studies reported reduction in service use and three studies reported functional improvements. Three studies found no effect. Findings were contradictory—there was evidence of reduced service use in the ED leading to increases in primary care service use. The suggested characteristics of effective interventions included preintervention screening and better links with home care.
Graf et al 18 described eight nurse-led CGA interventions which included follow-up. They reported that nurse-led CGA was effective in improving functional outcomes. There was varying evidence on ED readmissions (both reduced and increased admissions) and nursing home admissions. Three studies found no effect, attributed partly to study design limitations.
Malik et al 20 reported three different types of nurse intervention: assessment using risk screening, CGA, and nurse-led case and discharge management. This meta-analysis of nine studies found that nursing interventions did not have a significant statistical impact on any of four outcomes (hospitalisation, readmissions, length of hospital stay and ED revisits). This study did not examine functional decline. The researchers contrasted these findings with previous reviews11 16 17 which had demonstrated reduced service use as a result of these interventions, and had also reported that ED risk screening led to reduced hospitalisation and nursing home admissions. These inconsistencies are attributed to methodological weaknesses in study designs, supporting an agenda for additional research on interventions that extend from the ED to the community.
Pearce et al 21 identified only two studies which evaluated patient focused outcomes. The interventions were related to physical equipment supplied by nurses. Findings indicated that both warming blankets and seating position had a positive impact on patient comfort and well-being. The researchers noted the paucity of research around patient-centred outcomes such as nutrition, hydration and communication.
Jay et al 19 reported reduced admissions rates (ranging between 2.6% and 9.7%). The evidence for length of stay and readmission rates was mixed. A number of their included studies also reported changes in admissions rates for the control groups, indicating that CGA may have altered culture and practices around the risks of admission versus discharge.
Summary—There was conflicting evidence around the benefits of nurse-led interventions for older people in the ED. Included reviews reported reduced service use and reduced functional decline, in contrast to evidence of increased service use as a result of interventions. The strongest evidence, in the form of meta-analysis, found no effect from nurse-led interventions. There was evidence of lowered admission rates following geriatrician led CGA interventions. There were common methodological limitations reported across studies.
Population-focused reviews
Schnitker et al 23 and Sinha et al 26 reported evidence for identification and management programmes which specifically targeted older people with cognitive impairment. Schnitker et al 23 also reported staffing interventions (team and individual changes to service delivery and staff training). Neither review reported patient or health service outcomes. Both reviews described intervention characteristics that report positive outcomes, but not the outcomes themselves. Both reviews summarised that interventions were poorly represented or described within the ED literature. There was more evidence from acute care settings, although transferability of these interventions to the ED is not well understood.
Summary—There was limited evidence for population-focused interventions. The reporting of evidence made any comparison between reviews challenging. It was not possible to summarise ED interventions for older people with cognitive impairment.
Intervention component reviews
Three reviews reported on the core components of successful interventions and their outcomes. Fan et al, 24 Hughes et al 25 and Sinha et al 26 considered the key components or elements of effective interventions in addition to the overall effectiveness:
Core operational components of interventions and the role of these components in the success of interventions.26
Key elements of effective interventions.24
Intervention components and intervention strategies adopted.25
In terms of intervention effectiveness, the case management interventions reported by Sinha et al 26 were reported as having positive effects (not statistically significant) on satisfaction levels, ED reattendances, admission rates (immediate and longer term), and nursing home admissions. Negative results included a small but significant negative effect on ED reattendances26 and higher ED use.24 There was a statistically significant outcome of lowering ED use or length of stay in five of 20 studies.24 Hughes et al 25 found a small positive effect of ED interventions on functional status.
Table 4 reports components that were associated with interventions found in reviews to be effective. There was considerable overlap between the three reviews, indicated by shading.
Effective components of interventions
Summary—There was considerable agreement across three reviews for the components of successful interventions. Effective interventions: integrated strategies for social and medical care involvement; included screening and assessment; initiated care in the ED and bridged this with follow-up; monitored and evidenced successful practices. Care quality indicators tended to focus on care processes rather than structures or outcomes and were generally lacking in evidence and limited in testing.
Discussion
This review of reviews summarised evidence on interventions to improve outcomes for older people (including those with frailty related conditions) attending an ED. Overall, the evidence base was inconsistent. Across the reviews, there was incomplete reporting of interventions—a feature of reviews in which data lose details through abstraction from primary studies. In addition, there was high variability in the standards to which reviews were conducted and reported. Our findings are limited to each review authors’ interpretation of primary evidence. Some reviews reported primary studies by intervention type and others by their outcome, and this limits the potential for further synthesis of data. The evidence was broadly US focused and relatively old in terms of the studies included in the reviews. Summaries commonly featured calls for more primary research using rigorous evaluation methods, and also acknowledged the challenges of researching a vulnerable population in a fast moving and high pressured environment.
The evidence for CGA and related multidisciplinary interventions has been widely studied, but inconsistent reporting makes definitive conclusions difficult. Despite this, there was some evidence for effectiveness. In particular, geriatrician-led CGA appeared to have stronger effect on reducing admission rates than nurse-led interventions. Following CGA, however, ED reattendance rates may be unchanged or even increased, particularly in the short term. This may reflect the evidence for continuous rather than brief interventions: holistic, person-centred management plans take time to implement and to yield benefit, and there may be a short-term incidence of rebound problems for people while they adjust to change. Studies with a longer follow-up period may be required to understand whether this is the case.
There was a lack of evidence appraising targeted interventions for older people with cognitive impairment attending EDs. There was widespread evidence of holistic interventions being undertaken, including CGA. However, despite being a holistic and person-centred intervention, the effectiveness of CGA tended to be measured with service-related metrics (such as mortality and admissions) as opposed to patient centred metrics (such as pain and quality of life). Future research and quality improvement innovations should ensure that patients are consulted on the outcomes of importance.
Successful interventions integrated social and medical care, included screening and assessment, were initiated in the ED and bridged to other settings with follow-up, and monitored and evidenced successful practices. This has far reaching implications for service delivery and reconfiguration. There is a need for robust, multicentre controlled studies (eg, cluster RCT) that examine CGA-based interventions in the ED, focusing on patient-centred outcomes.
Ethics statements
Patient consent for publication
Ethics approval
No ethical approval was required for this review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Mary Dawood
Twitter @LouisePreston13, @J_vanOppen, @ProfSueMason
Contributors SPC and SMM conceptualised the study, SPC, SMM and LP obtained research funding for the study. LP, SPC, SMM, JDvO, SA and HW developed the protocol. HW ran the literature searches. LP, SA, SPC and JDvO undertook screening of the included studies, data extraction and quality assessment. LP drafted the manuscript and all authors contributed.
Funding This research was funded by the National Institute for Health Research, Health Services and Delivery Research - 17/05/96, £931 653.
Disclaimer The views expressed are those of the author(s) and not necessarily of the NIHR or the Department of Health and Social Care.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.