Article Text

Abstract
Background Resuscitative endovascular balloon occlusion of the aorta (REBOA) can be used as an adjunct treatment in traumatic abdominopelvic haemorrhage, ruptured abdominal aortic aneurysms, postpartum haemorrhage (PPH), gastrointestinal bleeding and iatrogenic injuries during surgery. This needs assessment study aims to determine the number of patients eligible for REBOA in a typical Norwegian population.
Methods This was a retrospective cross-sectional study based on data obtained from blood bank registries and the Norwegian Trauma Registry for the years 2017–2018. Patients who received ≥4 units of packed red blood cells (PRBCs) within 6 hours and met the anatomical criteria for REBOA or patients with relevant Abbreviated Injury Scale codes with concurrent hypotension or transfusion of ≥4 units of PRBCs within 6 hours were identified. A detailed two-step chart review was performed to identify potentially eligible REBOA candidates. Descriptive data were collected and compared between subgroups using non-parametric tests for statistical significance.
Results Of 804 patients eligible for inclusion, 53 patients were regarded as potentially REBOA eligible (corresponding to 5.7 per 100 000 adult population/year). Of these, 19 actually received REBOA. Among the identified eligible patients, 44 (83%) had a non-traumatic aetiology. Forty-two patients (79%) were treated at a tertiary care hospital. Fourteen (78%) of the REBOA procedures were due to PPH.
Conclusion The number of patients potentially eligible for REBOA after haemorrhage is low, and most cases are non-traumatic. Most patients were treated at a tertiary care hospital. The exclusion of non-traumatic patients results in a substantial underestimation of the number of potentially REBOA-eligible patients.
- resuscitation
- trauma
- abdomen- non trauma
- assessment
- obstetrics and gynaecology
Data availability statement
Data are available on reasonable request. Data were obtained from blood bank registries, the Norwegian Trauma Registry and the electronic patient journal of Central Norway Regional Health Authority. The dataset consists of deidentified participant data. Because of the interconnection of data from multiple registries, the Norwegian Center for Research Data has concluded that the dataset in whole could indirectly identify specific patients. Therefore, the data are stored on protected servers owned by St. Olav Hospital Trust and is not made publicly open.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this subject
Resuscitative endovascular balloon occlusion of the aorta (REBOA) can be used to manage non-compressible torso haemorrhage.
REBOA-eligible patients include those with traumatic abdominopelvic haemorrhage, ruptured abdominal aortic aneurysm and others (eg, postpartum haemorrhage).
Multiple studies have assessed the potential use of REBOA following trauma, but none have assessed the potential use in non-trauma populations.
What this study adds
Interrogation of blood bank registries is an effective method to identify non-trauma REBOA-eligible patients.
The overall incidence of REBOA-eligible patients is low, and over three-quarters have a non-trauma aetiology.
Introduction
Haemorrhage is the leading cause of death in trauma patients during the first 24 hours after a trauma incident and the second largest cause of prehospital deaths after trauma to the central nervous system.1 2 Exsanguination is also a feared outcome of ruptured aortic aneurysms and postpartum haemorrhage (PPH).3 4
Resuscitative endovascular balloon occlusion of the aorta (REBOA) allows effective haemorrhage control in non-compressible abdominal and pelvic bleeding.5 6 The procedure is used as a bridge to definite treatment in exsanguinating trauma patients, and its application outside the hospital has recently been assessed.7 8
In 2019, the first Delphi process on REBOA was published to clarify indications.9 However, there is still no widespread consensus on the indications for REBOA in trauma care. A systematic review proposed that patients eligible for REBOA could be divided into three main groups: those with traumatic abdominopelvic haemorrhage, those with ruptured abdominal aortic aneurysms and those with other causes, including PPH, bleeding from the gastrointestinal tract and extensive bleeding during pelvic surgery.3 The authors reported that 90% of patients treated with REBOA due to trauma had established haemorrhagic shock (systolic blood pressure below 90 mm Hg).
Any new treatment modality should ideally be implemented based on a thorough analysis of its expected effectiveness, associated risks and cost–benefit ratio. It is currently not known if REBOA improves survival in any patient cohort,3 10 11 but ongoing studies will try to assess the effect of REBOA in trauma care.12 Multiple studies have assessed the need for REBOA in traumatic populations.13–16 However, there are no studies focusing on non-traumatic indications, resulting in a critical gap in the literature.
As such, the first aim was to assess the number of patients, traumatic and non-traumatic, eligible for REBOA in a typical Norwegian population. The second aim was to describe these patients’ demographics, physiology and fluid resuscitation.
Methods
Study setting
We performed a retrospective cross-sectional study based on patient data obtained from two data registries: the Norwegian Trauma Registry (NTR) and local hospital blood bank registries in central Norway. We included patients admitted to hospitals in the 2-year period from 1 January 2017 to 31 December 2018.
The hospital system in the geographical area under study comprises seven hospitals situated in Trondheim, Molde, Kristiansund, Orkdal, Levanger, Namsos and Tynset. St. Olavs University Hospital in Trondheim is a tertiary care hospital (TCH) and a major trauma centre, and the others are acute care hospitals (ACH). The area is mixed urban and rural, with an adult population (18 years or older) of approximately 468 000.17 The city of Trondheim and its surrounding area is regarded as urban.18 Currently, REBOA, as an in-hospital treatment, is routinely performed only by interventional radiologists at the TCH for PPH.4 However, individual surgeons at the ACHs may by chance be trained in the technique and can perform REBOA when indicated. Some patients were transferred from an ACH to the TCH. The level of care was recorded as the hospital that the patient initially presented to.
Prehospital critical care is provided by a two-tier system consisting of paramedics and primary care physicians who are on-call 24/7 (tier one) and four anaesthesiologist-staffed prehospital mobile units (tier two).
Because we expected a small annual number of REBOA-eligible patients, a 2-year period was chosen. The NTR is a national quality register hosted by Oslo University Hospital. These data are registered in a central database (Medical Registry System) that ensures data security and integrity. Trauma patients in the NTR are registered manually by local registrars. All registrars are certified and have completed specific coding courses.
All hospitals except one, Kristiansund Hospital, reported to the NTR during the period. Kristiansund Hospital is not intended to receive trauma patients as it is not included as a trauma-receiving hospital within the regional trauma system.
Data collection and processing
Patients were identified via interrogation of both the NTR and individual hospital blood bank registries (figure 1).

{kind=link}
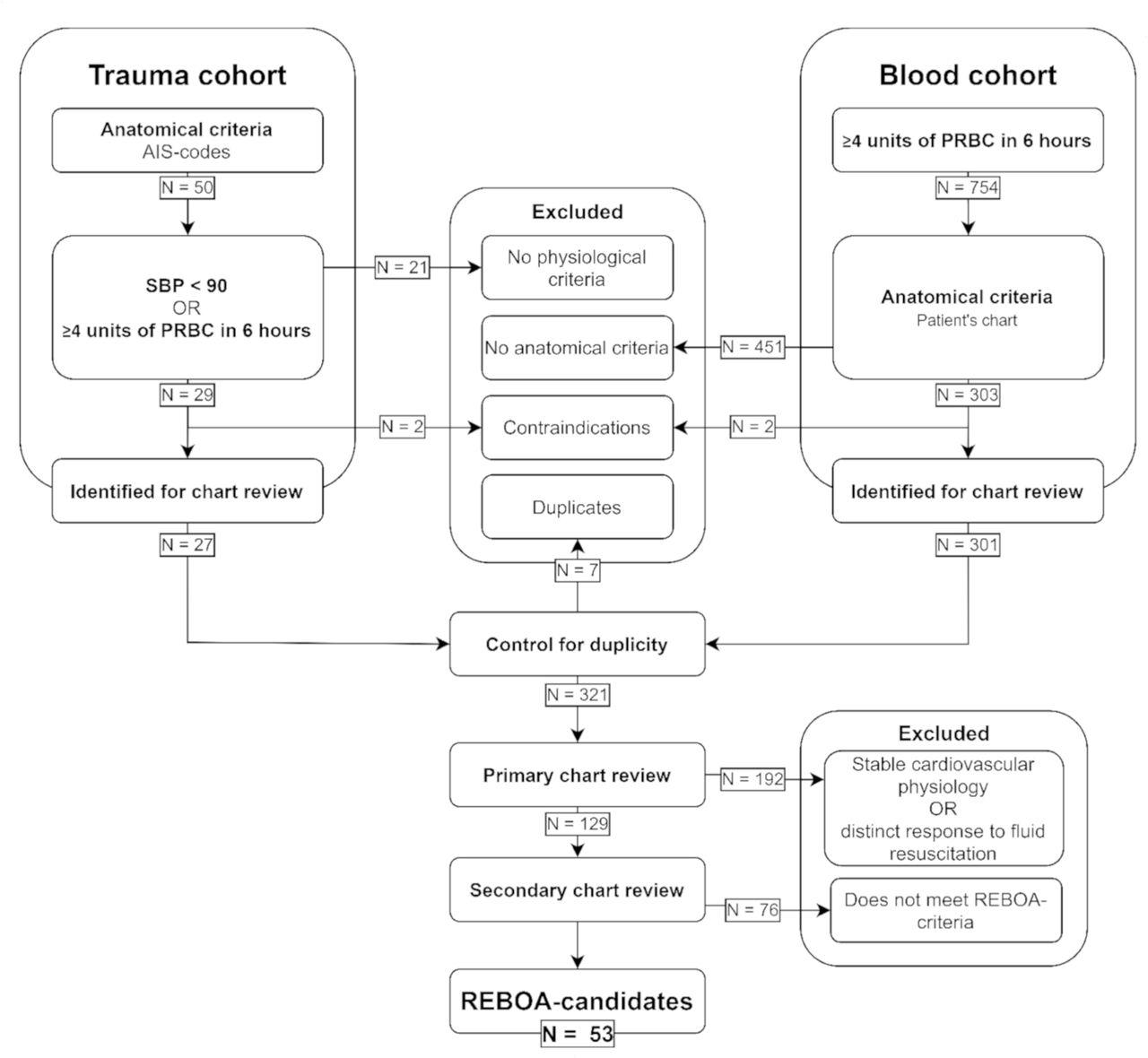
Flow chart of patient selection. Patients were identified through two different algorithm-based cohorts, which were followed by a two-step chart review. AIS, Abbreviated Injury Scale; PRBC, packed red blood cells; SBP, systolic blood pressure; REBOA, resuscitative endovascular balloon occlusion of the aorta.
Trauma cohort
Adult patients (18 years or older) registered in the NTR with an Abbreviated Injury Scale (AIS) code corresponding to a high-grade abdominopelvic injury were identified. We used the same anatomical indications for trauma patients as those published in earlier needs assessments of REBOA (table 1).13–15
Site or type of haemorrhage considered eligible for REBOA
Patients with a registered systolic blood pressure (SBP) <90 mm Hg or transfusion of four or more units of packed red blood cells (PRBC) within 6 hours, irrespective of admission, were included in the subsequent chart reviews. Non-compressible haemorrhage in the superior mediastinum, axilla, neck or face and aortic dissection are all regarded as contraindications to REBOA treatment. Patients with these contraindications were excluded.
Blood cohort
Data were obtained from the blood bank registry at each hospital. Adult patients (18 years or older) who were transfused with four or more units of PRBC in 6 hours were identified. PRBC is a unit of 200–300 mL erythrocyte concentrate with saline, adenosine, glucose and mannitol additive. Patients with anatomical indications for REBOA (table 1) were included in the subsequent chart review. Patients with the same contraindications as those used in the trauma cohort were excluded.
Processing
Duplicates in the two cohorts were removed. A primary chart review was performed by the first author (BNG) to exclude patients who were clearly not eligible for REBOA, those with stable cardiovascular physiology and those with distinct responses to crystalloid or blood resuscitation. The remaining patients were then subjected to a secondary chart review by two experienced consultant anaesthesiologists (JRB and AJK). All documentation on the acute incident registered in the electronic patient journal was assessed. The inclusion criteria were based on a consensus regarding indications from 20199: anatomical indications for REBOA (table 1), commencement of a massive transfusion protocol or transfusion of four or more units of blood products during the acute incident and patients registered as haemodynamically unstable in the patient’s medical record by the patient-responsible anaesthesia personnel or when organs were removed to enable surgical haemostasis. Patients who received REBOA or in whom REBOA was deemed necessary by the involved healthcare providers were also included. Patients with a high burden of comorbidities, those with a poor quality of life and patients in a state regarded as futile for treatment were excluded. Those patients evaluated as eligible by both reviewers were confirmed as eligible REBOA candidates. Disputed patient cases were discussed until agreement.
For eligible REBOA candidates, we extracted the lowest registered SBP prior to treatment, heart rate at the lowest registered SBP, total volumes of fluids, hospital, age, sex, survival status (dead/alive) until discharge, site of bleeding and AIS codes. The number of fluid transfusions reported during the acute incidence was defined as those administered during the period from injury or the start of decompensation until definitive treatment or death. Any difference in fluid resuscitation between TCH and ACH was assessed.
Statistical analysis
Statistical analysis was performed with SPSS, V.25.0 (2017) (IBM Corporation, Armonk, New York, USA). Continuous variables are reported as medians with IQRs. Categorical variables are described as counts and/or proportions (%). Incidence is presented as the rate with 95% CI. Comparisons of medians between groups with non-normal distribution of data were performed with the Mann-Whitney U test. Comparisons of proportions were performed with the Fisher’s exact test. A P value of <0.05 was regarded as statistically significant.
Ethical review
A Data Protection Impact Assessment was performed to identify and minimise the data protection risks of the study.
Patient and public involvement
This study was conducted without direct patient involvement. The patient’s and public’s interests were maintained by the involvement of Data Protection Officers of local health trusts.
Results
Initially, we identified 804 cases in the two cohorts (figure 1). The blood cohort consisted of 754 patients who received four or more units of PRBC in 6 hours. Of these, 303 had anatomical indications for REBOA. The trauma cohort consisted of 50 patients with anatomical indications for REBOA. Of these, 29 fulfilled the physiological criteria for REBOA. Four patients, two from each cohort, were excluded because of aortic dissections. Seven patients were found in both cohorts. Duplicates were removed from further analyses. A total of 321 patients were evaluated in the primary chart review. One hundred and ninety-two patients were regarded as clearly not eligible in this phase, leaving 129 patients to be evaluated in the secondary chart review. This process resulted in 53 patients being regarded as potentially REBOA eligible (table 2).
Demographics, presenting physiology, fluid resuscitation, level of care, type of haemorrhage and mortality in potentially eligible REBOA candidates
There were no differences in physiological parameters, or the volumes of fluids used in resuscitation between the group of potentially eligible patients who received REBOA and those who did not (table 3).
Comparison of the subgroups of potentially REBOA-eligible patients who did and did not receive REBOA
Comparison of fluid resuscitation conventions at the TCH and ACHs
The TCH and ACH fluid resuscitation conventions differed only regarding platelets, with median values of 500 mL and 250 mL, respectively (p=0.029). There were no significant differences in the provision of PRBC, plasma or crystalloids (table 4).
Fifty-three patients with a REBOA-amenable injury or condition in an adult population of 468 000 indicates an estimated incidence of 5.7 (95% CI 4.3 to 7.4) per 100 000 adult population/year. Of the 2210 trauma patients in the area over the 2-year period, 0.4% (n=9) were regarded as potentially eligible for REBOA as an adjunct treatment.
Discussion
This study finds that most patients eligible for REBOA as an adjunct treatment have non-traumatic aetiology. This is perhaps in contrast to current practice, where seemingly traumatic aetiology dominates. Our results estimate an incidence of 5.7 per 100 000 adult population/year.
Approximately one-third of the REBOA-eligible patients actually received REBOA, and most of these were due to PPH. This may reflect a specifically good collaboration between interventional radiologists and gynaecologists at the TCH.4 Regardless, it indicates that non-traumatic aetiology should not be overlooked. Patients registered at the TCH might have been eligible for REBOA earlier in the chain of care, during transfer, at an ACH, or even prehospital if it had been available.
Norwegian data show a low incidence of life-threatening trauma as well as low severity after trauma.18 Hence, our results may not translate to larger cities or urban areas where the trauma burden is more severe. However, we believe this study provides a realistic assessment of need in our area, as well as other Scandinavian or European areas with similar population densities. For example, we found the same estimation of trauma patients to be potentially REBOA eligible as a recent Swedish needs assessment.16 The design of our study was based on previously published studies, which focused solely on traumatic patients even though the literature describes other utilisations for the procedure.3 9 By adding the use of blood transfusions as a primary input, we were able to identify patients with non-traumatic indications for REBOA, and this greatly increased the number of REBOA candidates.
One needs assessment at a major trauma centre reported that 45% of the patients identified through an algorithm with anatomical and physiological criteria were regarded as truly REBOA eligible after chart review.14 In comparison, we found that only 17% were eligible. We believe that the use of blood transfusions as a primary input increases the necessity of a subsequent chart review, and in contrast to Dumas et al,15 we describe the inclusion/exclusion criteria of these reviews. One can argue that disputed patients who were initially regarded as eligible by only one investigator might not be clear-cut REBOA candidates. However, the subsequent joint chart review of these patients provides a plausible basis to regard them as eligible. It also demonstrates the complexity of real-life decision making in these patients.
We did not observe any difference in physiology or fluid resuscitation between those that did and did not receive REBOA. This increases the plausibility that all these patients were REBOA eligible. There was a small, non-significant difference in survival between the group that received REBOA and the group that did not. There was no difference in volumes of fluids used in resuscitation at ACHs and the TCH, except for transfusion of platelets. This is most likely due to differences in the availability of platelets between hospitals. Also, we observed that a high volume of crystalloids was used relative to blood transfusions.
The detection of possible differences in factors like postoperative morbidity, length of surgery, length of stay at hospital or the need to remove organs to enable surgical haemostasis between the two groups was beyond the scope of this study. Such outcome measures, combined with survival and fluid resuscitation requirements, would probably be the best endpoint in future studies.
REBOA is a highly invasive procedure that demands technical skill and is only achievable through considerable practice in the Seldinger technique and the use of ultrasound.8 19 20 A training programme designed for prehospital anaesthesiologists has been previously reported.21 Our findings suggest that at ACHs, fewer than one patient per year is potentially REBOA eligible. There might therefore be a need for REBOA competence at TCHs, but our findings question the need for REBOA competence at ACHs. However, our study does not include potential cases where REBOA could have been used in out-of-hospital non-traumatic cardiac arrests or patients eligible for early femoral arterial access.22–24
Limitations
This study has several limitations. First, the specificity of the algorithm used to identify REBOA candidates decreases when a blood cohort is added, increasing the necessity of chart review. Second, we admit that the chart review would have been more reliable if it was performed by reviewers not directly involved in the study. However, we report the inclusion/exclusion criteria that were used to ensure a transparent decision process. Third, the volumes of fluids reported were extracted from the charts and blood bank registry. These values were not always in agreement, possibly due to the use of emergency blood immediately available in the resuscitation room or errors in registration. When different values were found, the highest value was reported as we regarded lack of registration as more likely than too many registrations. Finally, manual registrations in the NTR allows for erroneous inputs. However, due to certifications and specific coding courses, the numbers of mistakes expected in the data input are low.
Conclusions
This analysis of national trauma registry data and the novel use of blood bank data constitutes the first needs assessment of REBOA including non-traumatic aetiology, as well as the first needs assessment of REBOA in patients with major haemorrhage in Norway 24. The number of patients eligible for REBOA after haemorrhage is low, and most cases are non-traumatic. We find that excluding non-traumatic patients greatly underestimates the number of potentially REBOA-eligible patients. This finding is important for future implementation of REBOA in clinical practice.
Data availability statement
Data are available on reasonable request. Data were obtained from blood bank registries, the Norwegian Trauma Registry and the electronic patient journal of Central Norway Regional Health Authority. The dataset consists of deidentified participant data. Because of the interconnection of data from multiple registries, the Norwegian Center for Research Data has concluded that the dataset in whole could indirectly identify specific patients. Therefore, the data are stored on protected servers owned by St. Olav Hospital Trust and is not made publicly open.
Ethics statements
Ethics approval
The study was approved by the Regional Committees for Medical and Health Research Ethics (reference 2019/793/REK-Midt) and the Data Protection Officer in every health trust was involved.
Acknowledgments
We would like to thank the members of the Norwegian Trauma Registry, the information and technology administrators of the blood banks, the involved Data Protection Officers, Nord-Trøndelag Hospital Trust, Møre og Romsdal Hospital Trust, Innlandet Hospital Trust and St. Olav Hospital Trust.
References
Footnotes
Handling editor Ed Benjamin Graham Barnard
Twitter @BredeJostein, @andreasjkruger
Contributors JRB and AJK conceived the study idea. All authors contributed to the design of the study. BNG collected the data and performed the analyses. All authors discussed the results and contributed to the final manuscript.
Funding This study was funded by the Norwegian University for Science and Technology. The contributions from other personnel were agreed on without any financial compensation.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.