Article Text

Abstract
Background Timely management of non-convulsive status epilepticus (NCSE) is critical to improving patient outcomes. However, NCSE can only be confirmed using electroencephalography (EEG), which is either significantly delayed or entirely unavailable in emergency departments (EDs). We piloted the use of a new bedside EEG device, Rapid Response EEG (Rapid-EEG, Ceribell), in the ED and evaluated its impact on seizure management when used by emergency physicians.
Methods Patients who underwent Rapid-EEG to rule out NCSE were prospectively enrolled in a pilot project conducted at two ED sites (an academic hospital and a community hospital). Physicians were surveyed on the perceived impact of the device on seizure treatment and patient disposition, and we calculated physicians’ sensitivity and specificity (with 95% CI) for diagnosing NCSE using Rapid-EEG’s Brain Stethoscope function.
Results Of the 38 patients enrolled, the one patient with NCSE was successfully diagnosed and treated within minutes of evaluation. Physicians reported that Rapid-EEG changed clinical management for 20 patients (53%, 95% CI 37% to 68%), primarily by ruling out seizures and avoiding antiseizure treatment escalation, and expedited disposition for 8 patients (21%, 95% CI 11% to 36%). At the community site, physicians diagnosed seizures by their sound using Brain Stethoscope with 100% sensitivity (95% CI 5% to 100%) and 92% specificity (95% CI 62% to 100%).
Conclusion Rapid-EEG was successfully deployed by emergency physicians at academic and community hospitals, and the device changed management in a majority of cases. Widespread adoption of Rapid-EEG may lead to earlier diagnosis of NCSE, reduced unnecessary treatment and expedited disposition of seizure mimics.
- neurology
- epilepsy
- emergency care systems
- emergency departments
- emergency department management
- critical care transport
- intensive care
Data availability statement
Data are available on reasonable request. The deidentified patient data have been shared with the sponsor and the investigators have access to it. This is not an open access data but we can work with our institutions to release data as needed.
Statistics from Altmetric.com
- neurology
- epilepsy
- emergency care systems
- emergency departments
- emergency department management
- critical care transport
- intensive care
Key messages
What is already known on this subject
Non-convulsive status epilepticus is an important cause of persistent altered mental status, especially after recent convulsive status epilepticus.
Limited access to electroencephalography (EEG) currently hampers timely diagnosis and treatment of non-convulsive seizures and status epilepticus.
Rapid Response EEG, an easy-to-use device that expands access to stat EEG, has been previously tested in critical care settings; however, its utility in the emergency department (ED) has not been described.
What this study adds
In this prospective pilot study, we found that the use of EEG in the ED using Rapid Response EEG has the potential to positively impact the clinical management of suspected non-convulsive seizures.
Introduction
Non-convulsive status epilepticus (NCSE) is a neurological emergency that is increasingly recognised as a cause of persistent altered mental status, especially after convulsive status epilepticus, as well as neuronal injury and long-term neurological disability.1–3 Timely diagnosis and treatment is warranted to prevent morbidity and mortality. However, NCSE can only be diagnosed with electroencephalography (EEG), which is often inaccessible in the emergency department (ED), and empiric treatment without EEG can be misguided.4
Rapid Response EEG (Rapid-EEG; Ceribell, Mountain View, California, USA) is a recently developed, FDA-approved EEG system designed for point-of-care evaluation in emergency and critical care settings that can be applied by any provider in under 5 min. Rapid-EEG is equipped with a display screen for visual review of brainwaves and a Brain Stethoscope function that sonifies EEG signals to facilitate non-expert detection of seizures and rhythmic discharges.5 In a prospective multicentre clinical trial, Rapid-EEG significantly improved physicians’ diagnostic accuracy and confidence.6 We designed the current pilot project to test the utility of Rapid-EEG in two different ED settings—an academic medical centre (Stanford Health Care (SHC)) and a community hospital (Episcopal Hospital (EH)).
Methods
Patient enrolment and clinical workflow
This project was designed as a quality improvement project at both sites and was granted exemption from review by the Institutional Review Boards of the participating institutions. We enrolled patients between August 2019 and February 2020 who met one of the pre-specified inclusion criteria (figure 1A, top). Each hospital employed its own clinical workflow for integrating Rapid-EEG into ED patient evaluation (figure 1B). We excluded patients with open head wounds as specified by Ceribell, and paediatric and pregnant patients since they were triaged to different locations in the hospital. At SHC, Rapid-EEG was set up by ED technicians and preliminary review was performed by the on-call EEG fellow, whereas at EH, emergency physicians applied the Rapid-EEG device themselves and used the Brain Stethoscope function to perform a preliminary review of the EEG sound.

Patient enrolment and Rapid-EEG clinical workflow. (A) Inclusion and exclusion criteria for patient enrolment (top) and patient flow diagram (bottom). (B) Clinical workflow for acquiring and interpreting Rapid-EEG at two ED sites—EH (community affiliate of Temple University in urban Kensington section of Philadelphia; annual volume over 46 000 ED visits) and SHC (academic medical centre designated as a Level 1 Trauma Center and a Comprehensive Stroke Center serving San Francisco Bay Area; annual volume over 78 000 ED visits). Emergency physicians at EH do not have access to either conventional EEG or consulting neurologists available on-site, and they performed their own preliminary interpretation of Rapid-EEG using the device’s Brain Stethoscope function and classified the sonified EEG as either seizure or non-seizure. At SHC, which has neurologists available 24/7 for on-site consultation and EEG technicians available on-site during the day and evening and on-call from home overnight, the on-call neurologist (EEG fellow) performed a preliminary interpretation of the first 15 min of recording. At both sites, an attending neurologist remotely reviewed the entire Rapid-EEG record within 24 hours. Prior to patient enrolment, staff completed online training on Rapid-EEG headband application and Brain Stethoscope interpretation. ED, emergency department; EEG, electroencephalography; EM, emergency medicine; EH, Episcopal Hospital; Rapid-EEG, Rapid Response EEG; SHC, Stanford Health Care.
Data collection and analysis
Our primary outcome was the impact of Rapid-EEG on clinical management, defined as the proportion of patients with a change in diagnosis, treatment or disposition that treating physicians attributed directly to the use of Rapid-EEG when they were electronically surveyed about their perceptions of Rapid-EEG’s impact on patient care. We also measured the sensitivity and specificity of emergency physicians’ EEG interpretations using Brain Stethoscope against attending neurologists’ diagnoses based on visual EEG review. Variability of measured proportions (including sensitivity and specificity) was reported using 95% CI. Rapid-EEGs were categorised based on attending neurologists’ clinical reports as seizures (status epilepticus or isolated seizure), highly epileptiform patterns (HEP; rhythmic and/or periodic epileptiform activity highly associated with seizures7), or non-epileptiform activity (diffusely slow or normal background).
Patient and public involvement
There was no patient or public involvement in this project.
Results
We consecutively enrolled 44 participants at the project sites; 38 patients (SHC, n=24; EH, n=14) were included in the final analysis after 6 patients at EH were excluded (figure 1A, bottom). Patient clinical characteristics are shown in table 1.
Patient cohort characteristics
Clinical events or abnormal movements preceded Rapid-EEG monitoring in 61% of patients; 82% of patients were admitted. Three patients (11%) were confirmed to have ongoing seizure or HEP using Rapid-EEG, and one patient (3%) was in NCSE; all four of these patients received antiseizure medications (ASMs) immediately following Rapid-EEG diagnosis. At EH, emergency physicians diagnosed two patients with seizures and ruled out seizures in 12 patients using Brain Stethoscope; neurologist visual review confirmed that one of the two seizure cases was in NCSE, while the other had diffuse slowing, and in the remaining 12 patients, unanimously agreed with emergency physicians’ non-seizure diagnoses. As such, emergency physician interpretation of sonified EEG using Brain Stethoscope was 100% sensitive (95% CI 5% to 100%) and 92% specific (95% CI 62% to 100%).
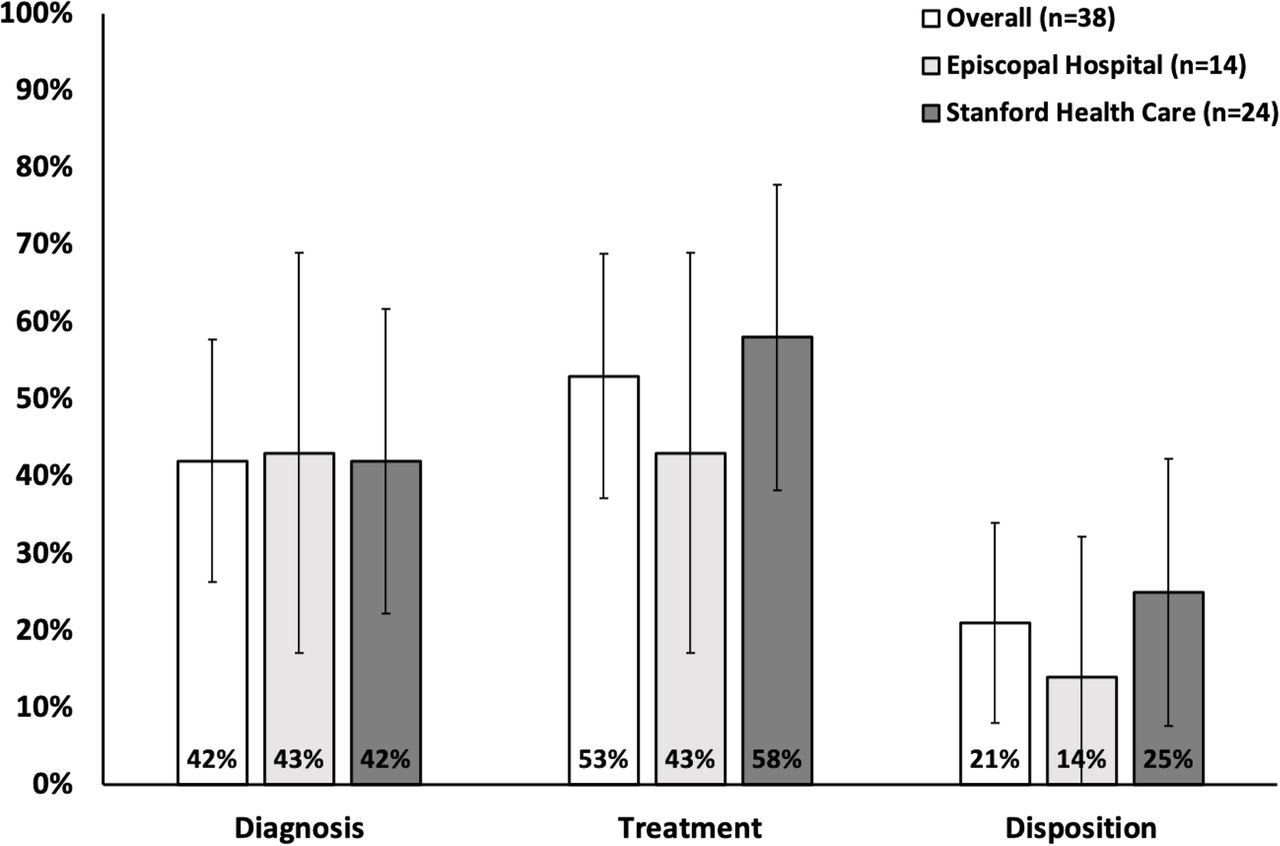
Across both sites, Rapid-EEG led to diagnostic confirmation (n=16; 42%, 95% CI 28% to 58%), change in clinical management (n=20; 53%, 95% CI 37% to 68%) and expedited disposition (n=8; 21%, 95% CI 11% to 36%) (one or more could apply to each patient). EH emergency physicians reported a change in treatment in six cases (43%, 95% CI 21% to 67%) based on their own interpretation of the Rapid-EEG sonified data; in these cases, emergency physicians reported giving fewer ASMs because their EEG interpretation using Brain Stethoscope did not confirm seizures in patients they would have otherwise empirically treated. At SHC, the median time from the start of EEG recording to preliminary diagnosis by the EEG fellow was 75 min; Rapid-EEG was reported as having expedited disposition in six cases (25%, 95% CI 12% to 45%) (figure 2).
{kind=link}
{kind=link}
Impact of Rapid-EEG on clinical management of suspected NCSE. Emergency physicians reported the perceived impact of rapid response EEG on diagnosis, treatment and disposition of patients with suspected NCSE. Error bars represent 95% CI. EEG, electroencephalography; NCSE, non-convulsive status epilepticus.
Discussion
Our pilot project adds to prior studies of EEG in the ED, which have largely relied on the use of conventional EEG or simplified EEG devices that rely on neurologist interpretation, by expanding the literature on Rapid-EEG from critical care to emergency care settings.8–10 Emergency physicians attributed changes in diagnosis, treatment or disposition to Rapid-EEG in at least 53% of patients, and their use of Rapid-EEG’s Brain Stethoscope function at the bedside was highly accurate in diagnosing and ruling out seizures. These preliminary findings support the claim that point-of-care seizure detection technology can expedite appropriate diagnosis and management of NCSE in the ED.
Limitations
Our pilot project was limited by its small sample size and its use of outcomes based on clinical judgments of emergency physicians that must be validated against objective measures. We did not perform follow-up after patients were discharged from the hospital since this was beyond the scope of this pilot project. At the time of this study, evidence supporting the use of Brain Stethoscope to confirm psychogenic seizures was limited; therefore, our physicians did not use the Brain Stethoscope for this indication. Future large-scale studies of Rapid-EEG in the ED may overcome many of these limitations.
Conclusion
Rapid-EEG was successfully deployed by emergency physicians at academic and community hospitals, and the device changed management in a majority of cases. Widespread adoption of Rapid-EEG may lead to earlier diagnosis of NCSE, reduced unnecessary treatment and expedited disposition of seizure mimics.
Data availability statement
Data are available on reasonable request. The deidentified patient data have been shared with the sponsor and the investigators have access to it. This is not an open access data but we can work with our institutions to release data as needed.
Ethics statements
Patient consent for publication
Ethics approval
This project was designed as a quality improvement project at both sites and was granted exemption from review by the Institutional Review Boards of the participating institutions.
Acknowledgments
We would like to thank our research coordinators (Rosen Mann and Anita Visweswaran), emergency department technicians and RN leadership (Patrice Callagy and Karen Stuart) as well as the Stanford informatics team, Stanford Emergency Department Management Council and Temple University Hospital Physicians and Staff for assistance in implementing this project in the emergency departments.
Footnotes
Handling editor Ed Benjamin Graham Barnard
Twitter @NinaGentileMD, @PrashaG2017
NMKW and ESM contributed equally.
Contributors PG, ESM, DI, MPJ and NTG conceived and designed the project. PG and NMKW obtained research funding. PG and NG provided statistical advice on project design and analysed the data. NMKW and ESM drafted the manuscript, and all authors contributed substantially to its revision. PG takes responsibility for the paper as a whole.
Funding This project was partially funded by Ceribell (at Stanford University) and the SAEM/RAMS Resident Research Grant (RF2019-009).
Competing interests KG serves as a scientific advisor and consultant to Ceribell Inc., which is commercialising Rapid Response EEG for clinical use.
Provenance and peer review Not commissioned; externally peer reviewed.