Article Text

Abstract
Background E-scooters have emerged as a frequently used vehicle in German cities due to their high availability and easy access. However, investigations about the causes and mechanisms of E-scooter incidents and their trauma-specific consequences are rare.
Methods We analysed all patients involved in E-scooter incidents from June to December 2019 who presented to four inner-city EDs in Berlin. The prospective data included patient-related and incident-related data, information on injury patterns and therapy, responses in a voluntary questionnaire concerning E-scooter use and general traffic experience.
Results 248 patients (129 males; median age 29 years (5–81)) were included: 41% were tourists and 4% were children. Most incidents (71%) occurred between July and September 2019, the majority occurring at weekends (58%). The injury pattern was mostly multifocal, affecting the lower (42%) and upper limbs (37%) and the head (40%). Traumatic brain injury was associated with alcohol consumption. Inpatient admission was recorded in 25%, surgery in 23%.
Conclusion This study has defined the incidence of injury related to E-scooter use in a major European city. Stricter laws governing the use of E-scooters, the wearing of helmets and technical modifications to the E-scooter platforms might decrease E-scooter-associated incidents and resulting injuries in the future.
Trial registration number German Clinical Trials Registry (DRKS00018061).
- trauma
- accidental
- emergency department
- musculoskeletal
Data availability statement
Data are available upon reasonable request. All collected data have been entered into an Excel data sheet and patient’s privacy information has been pseudonymised. The Excel document itself is password protected and saved upon a password-protected server of the Department of Emergency Medicine at Charité University Medicine Berlin with restricted access. Data protection is following the data protection declaration of the respective institution and will be available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this subject
E-scooters are an innovative and rising modality of mobility, especially in urban areas worldwide. Previous investigations have mainly described the numbers of E-scooter incidents and the related musculoskeletal injuries.
What this study adds
With this study, we not only identified injury patterns but also trauma mechanisms and risk factors of E-scooter-related incidents. As a result, we propose stricter regulations for the use of E-scooters. These should include the wearing of helmets, an age limit of 18 years, a ban on alcohol and a strict adherence to traffic regulations, such as avoiding driving on pavements. By performing technical modifications to the E-scooter platforms, providers can help to eliminate an additional source of injury.
Introduction
The desire for mobility as well as the recently increased awareness of the necessity for sustainability and environmental protection has sparked a growing interest in electric vehicles. In most larger cities, such vehicles are available from different providers through sharing concepts. The so-called free-floating concept allows customers to unlock vehicles with a simple smartphone app, to pay the rent electronically and to park them at any time within a certain area. E-scooters in particular have become popular in major European cities since their initial licensing in June 2019 and have immediately led to a change in the cities’ streetscapes.
With its 3.8 million residents and almost 14 million tourists every year,1 Berlin was chosen by many providers for testing and optimising new short-distance mobility concepts, known as micromobility. In September 2019, more than 11 000 E-scooters became available in Berlin.2 3 Movement profiles have shown increased usage of E-scooters in central districts where micromobility plays a decisive role. At the same time, motor vehicle traffic density is high in central areas, which yields an increased risk of incidents.
Many users indicate that E-scooters are a good alternative to cars in regard to covering short distances.4 Nevertheless, the lack of public awareness for the proper use of E-scooters and the consequences of incidents seem to be a problem. Data from the US National Electronic Injury Surveillance System showed a dramatic increase in injuries from E-scooter incidents after their introduction in 2017 and 2018.5 These data have been derived mainly from accounting data, especially from the state accident insurance.5 Although they provide information on the number of injured individuals, they give less information on clinical aspects such as injury patterns, causes of incidents, therapies and outcomes.
Large European studies describing E-scooter-specific injury patterns are still rare, mainly of retrospective nature and risk factors or trauma mechanisms have hardly been described. In a small retrospective case series, we were able to show that E-scooter-related incidents often occur due to inexperienced users, traffic violations and alcohol consumption as well as due to the vehicles themselves not being roadworthy.6 The aim of this large prospective study was to further investigate our previous findings on trauma mechanisms and injury patterns in order to identify risk factors and suggest improvements for the use of E-scooters.
Patients and methods
Data collection
We undertook a prospective observational multicentre study across four central EDs in the district of Berlin-Mitte: Charité Campus Mitte (CCM), Charité Campus Virchow-Klinikum (CVK), Bundeswehrkrankenhaus (BWK) and Evangelische Elisabeth Klinik (ELI).
All patients who presented to these EDs between June and December 2019 after E-scooter incidents were included in this study. Patients either self-presented or were brought in by the ambulance service.
Patient-specific data as well as information on the severity, diagnosis and treatment of injuries were recorded prospectively in the hospitals’ electronic documentation system. Traumatic brain injury (TBI) was defined as head injury with resulting loss of consciousness reported by first helpers, the ambulance service or in case of patient’s amnesia. Patients received either ambulatory interventions like wound care and cast immobilisation or were admitted as inpatients for surgery, comprehensive monitoring or extensive wound management. In order to identify risk factors for E-scooter incidents, patients presenting to the EDs of CCM and CVK received a questionnaire asking for the cause of the incident, previous experience with E-scooters, possession of a driving licence, alcohol consumption and the wearing of a helmet. The completion of the questionnaire was carried out voluntarily after a declaration of consent had been given by the patient or their legal guardian. If alcohol consumption was indicated by the patient or otherwise presumed, an alcohol breath test was performed. Patients presenting to the EDs of BWK and ELI did not complete questionnaires so that only clinical data could be obtained.
Statistical analyses
The data analysis was carried out using Excel software (Microsoft Excel V.2016, Microsoft Corporation, Redmond, Washington, USA) and SPSS V.26.0. Descriptive analyses were reported as the means and SDs, medians and both quartiles and ranges, or absolute numbers and percentage referring to the study group.
For parameters with a Gaussian distribution, statistical significance was defined using Student’s t-test. Significant associations among categorial variables were investigated by the Χ2 test or Fisher’s exact test. For the convenience of the reader, we additionally performed McNemar tests to compare two correlated proportions considering the injury distribution to emphasise the most affected body regions and the most frequent type of injury. The ORs for the defined risk factors (previous experience with E-scooters, driving licence, alcohol consumption, wearing of helmet) and their association regarding inpatient admission and traumatic brain injury (TBI) have also been calculated. To show quantitative associations concerning non-normally distributed variables, the Mann-Whitney U test was performed. The statistical significance level was set at values of p<0.05. All p values provided in this paper are considered part of the exploratory analysis and have not been adjusted for multiple testing.
Results
Patient population
A total of 248 patients were admitted to the four EDs and included during the 6-month study period.
The demographic details are given in table 1.
Presentation of demographic parameters of patients after E-scooter incidents (n=248)
More than half of the patients (58%) were Berlin residents and 41% were tourists. In 20 patients (8%), the incidents happened on the way to or from work.
The survey regarding possession of a driving licence and previous experience with E-scooters was carried out exclusively at CCM and CVK, where 120 patients (48% of all patients) volunteered to answer the questionnaire.
Times of incident
The majority of E-scooter incidents (75%) occurred between July and September. Regarding the time of day, we noticed a peak of E-scooter incidents in the afternoon between noon and 18:00 (40%) and in the evening from 18:00 until midnight (29%). In addition, there was a notable increase of E-scooter injuries on weekends between Friday afternoon and Sunday night (58%) (figure 1).

Percentage distribution of the emergency admissions according to the months, the time groups and the day (weekdays: Monday–Thursday, weekend: Friday–Sunday). The numbers on top of the bars show the absolute numbers.
Causes of incidents
The causes of incidents are summarised in table 2. Most E-scooter riders reported that they fell off the vehicle because they had lost control due to inattention, single-handed driving for indicating a direction change, lack of practice or inappropriate speed. Another reason for incidents was collision with other vehicles or inanimate objects, like kerbs, road obstacles or tram tracks. Injuries caused from contact with the sharp edges or protruding screws of the E-scooter occurred mainly during the process of acceleration by pushing off from the ground or while trying to brake (figure 2). Pedestrians were injured in 12 cases (5%), either by getting hit by an E-scooter (n=9) or by tripping over a parked vehicle (n=3).

Soft tissue laceration at the medial malleolus of a 30-year-old female patient after hitting the rear screw while accelerating the E-scooter.
Causes of incidents and analysis of risk factors with regard to inpatient admission and TBI
Injury patterns
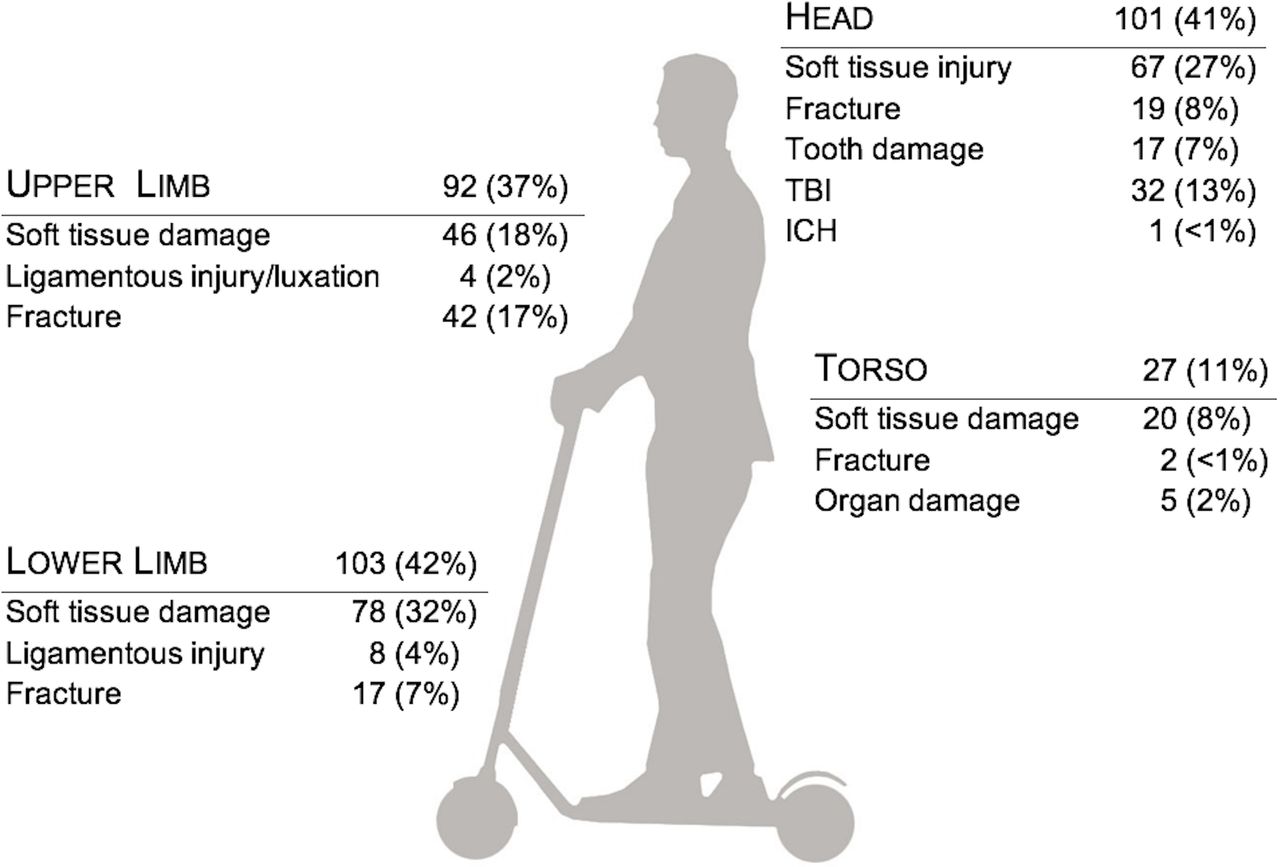
Injury patterns are summarised in figure 3.

Distribution of injuries with regard to body region. The numbers represent the number of patients suffering from each injury. Multiple localisations might be affected. A total of 136 head injuries occurred in 101 patients. Thus, multiple injury entities are possible per patient. ICH, intracerebral haemorrhage; TBI, traumatic brain injury.
Limb injuries were recorded in 178 patients and made up the majority of all injuries (72%). They were divided into soft tissue injuries, joint dislocations and fractures. The lower limbs were affected more frequently than the upper limbs (34% vs 30%, p=0.477). Seventeen patients (7%) suffered from injuries of the upper and lower limbs simultaneously.
On the lower limbs, we observed significantly more soft tissue injuries than fractures (31% vs 7%, p<0.001). Soft tissue injuries were contusions, abrasions, bruises, grazes and lacerations, which were often observed at the medial malleolus resulting from pushing off the ground to gain speed (figure 4). A total of 17 patients had a fracture of the lower limb, with the need for surgical treatment in 13 patients. Figure 5 presents an overview of the localisation and the frequency of extremity fractures. Eight patients (3%) had ligamentous or meniscal damage, mainly to the knee, without a fracture.
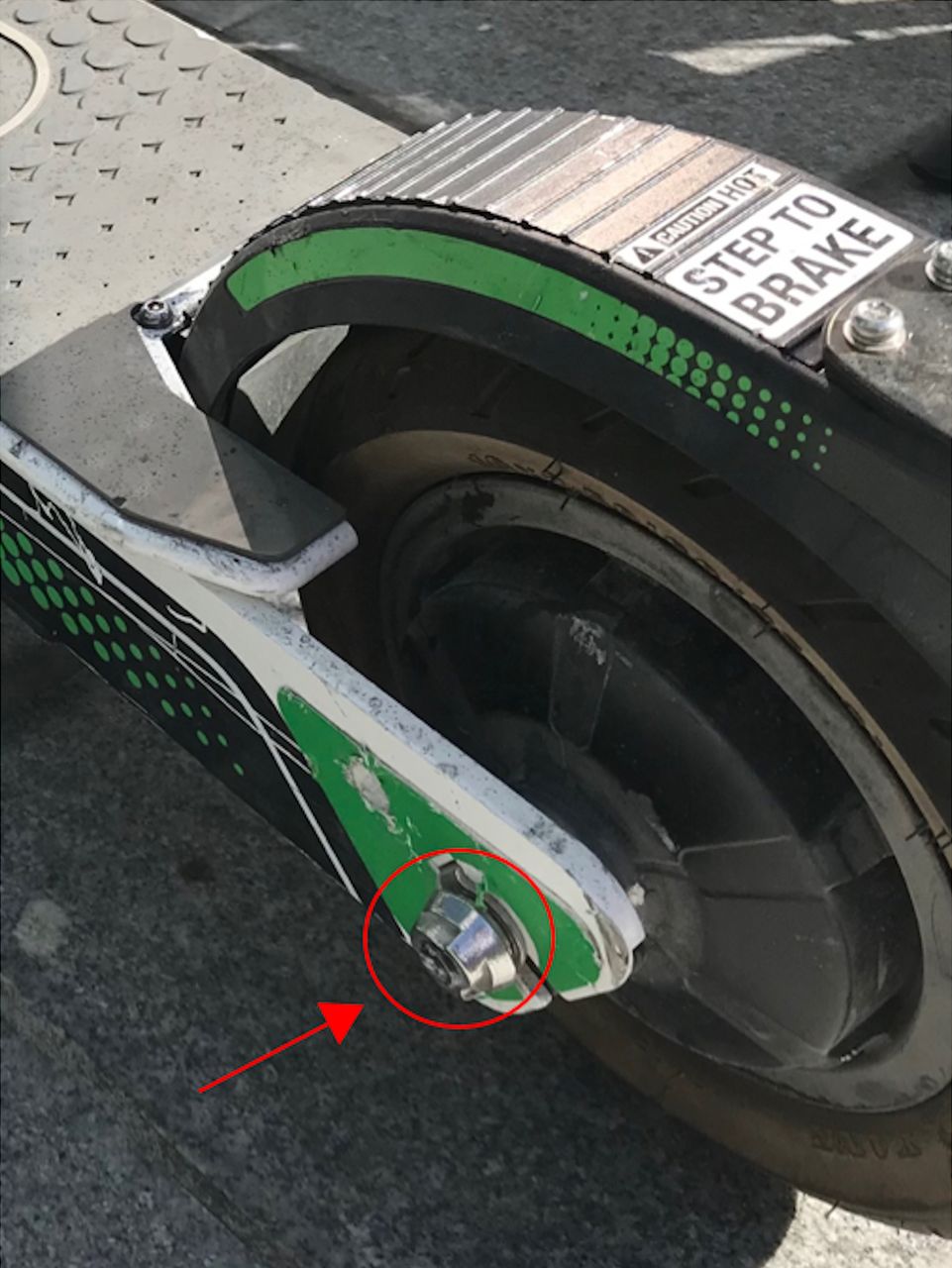
Screw at rear wheel of an E-scooter.

Distribution of the fractures and their location at the upper extremities (left) and at the lower extremities (right) (n=number of patients). One patient suffered from fractures at upper and lower limbs (fracture of the thumb and pertrochanteric femur fracture on same side).
On the upper limbs, the numbers of soft tissue injuries and fractures were nearly the same (18% vs 17%, p=0.749). The upper limbs were significantly more often affected by fractures than the lower limbs (17% vs 6%, p=0.001). Fractures of the upper limbs occurred mostly at the elbow joint or more distally, and 21 patients (8%) required surgery. Four patients had shoulder dislocations without any fracture.
Only one patient suffered from fractures of both lower and upper extremities.
In total, 135 head injuries were recorded in 101 patients. All head injuries were divided into soft tissue injuries (27%), fractures (19%) and tooth damage (17%). Fractures affected the midface or mandible with the exception of one skull fracture. One patient had an intracerebral haemorrhage.
Among all patients, 32 (13%) had concomitant TBI of mild severity and 22 of them (9% of all patients) required hospital admission and monitoring for at least 6 hours due to their symptoms.
Trunk injuries were rare and mainly affected the soft tissue (figure 3). Severe injuries occurred in a total of six patients: a liver and a spleen laceration, a unilateral and a bilateral pneumothorax, a haemothorax and a stable vertebral body fracture. Figure 6 illustrates the distribution of the injury entities for the entire study population.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Total distribution of injury types. Soft tissue damage including bruises, grazes, laceration and other wounds. Ligamentous damage occurred especially in combination with luxation or in case of clinically suspected.
Ambulatory and inpatient treatment
A total of 122 patients (49%) required a surgical intervention either ambulatory or as inpatients. Ambulatory treatment was performed in 65 patients (26%) and included wound care, suturing and cast immobilisation. Sixty-one patients (25%) were admitted as inpatients, 57 of them (23%) underwent surgery. The median hospital stay was 3 days (1–12 days). Patients with TBI were hospitalised for a median of 1 day (1–6 days) compared with the remaining hospitalised patients who stayed for a median of 4 days (1–12 days; p<0.001). One patient had to be transferred to another hospital due to a large skin defect. No patient died.
Risk factors
Table 2 summarises the risk factors for the incidence of E-scooter injuries. Of the 120 patients who participated in the voluntary survey, 82 had a driving licence (68%), and 58 participants (48%) reported having had previous experience in riding E-scooters.
In 49 patients (20%), the alcohol breath test was positive. Among patients with alcohol consumption, 15 patients had TBI (31%). A positive alcohol test was associated with a fivefold increase in the odds of TBI (p<0.001) and a twofold increase in the odds of inpatient admission (p=0.033) (table 2). Fifty-eight patients had previous experience with E-scooters but showed a threefold increase in the odds of TBI (p=0.042).
Of note, within the 15 patients who had a positive alcohol test and TBI, 12 patients stated that they had previous experience with E-scooters.
Only 1% of the E-scooter riders wore a helmet.
Discussion
This study shows that E-scooter riders were mainly aged 18–40 years. The lower limbs were affected the most, mainly with soft tissue damage, followed by head injuries. Fractures requiring surgery occurred more frequently in the upper limbs. E-scooter incidents occurred mainly in the afternoon and evening, and rather on weekends than on weekdays. They were often caused by a violation of traffic regulations, the user’s inattentiveness or a risk-taking driving style such as one-handed driving, jumping over kerbs and alcohol consumption.
Driving under the influence of alcohol yielded a significantly higher risk of TBI, even if the riders were experienced in handling E-scooters. This is important to note, because the permitted blood alcohol limit for E-scooter driving in Germany is at 0.05%, and exceeding this limit is subject to a fine and may be a criminal offence.7 Other international studies confirm our results by revealing that positive blood alcohol tests occur in up to one-third of E-scooter incidents.8–14
Trivedi et al were the first to investigate the consequences of E-scooter injuries within 1 year after their registration in California. They noted that there were more E-scooter injuries at the ED than in cyclists or pedestrians during the same time period.15 Other studies published similar results with an incidence of up to 60 per 100 000 E-scooter rides within 6 months, resulting in a short-term ban of E-scooters in selected cities.8 9
Frequently discussed risk factors for E-scooter injuries are the young age of the riders, a lack of experience in handling E-scooters and the absence of a driving licence. Under German law, E-scooters can be driven from the age of 14 years and hence a driving licence is not required. However, according to our study, neither the possession of a driving licence nor the previous experience with E-scooters prevented incidents. In contrast, TBI occurred more frequently in patients with previous experience and young age seems to be a more relevant risk factor, because at least one-third of E-scooter incidents involved children.5 12 13 15–18 Consequently, the Californian government introduced an age limit of 18 years and a driving licence requirement for renting E-scooters.
E-scooters are often compared with bicycles, and although the injury patterns resulting from incidents are in fact similar, their causes are different. A study on bicycle incidents in Muenster (Germany) reported collisions with motorised vehicles as the major cause of incidents, especially in younger patients.19 20 In contrast, most E-scooter incidents occur without external influence and are related to inattention of the E-scooter users or violation of traffic regulations. Although E-scooters are only allowed to be used on cycle paths and roads, up to one-quarter of E-scooter incidents take place on pavements, often injuring pedestrians.8 12 13 15 Typically, the riders lose stability when hitting the kerb to get onto the pavement, because the E-scooter front wheel is rather small in diameter and thus acts as a fulcrum. Furthermore, the narrow E-scooter wheels are prone to get stuck in the tram tracks.
In contrast to cyclists, E-scooter riders hardly ever wear a helmet, which is confirmed by several international studies.8 10 12–14 18 21–23 In Germany, helmets are mandatory for riders of most motorised vehicles; for E-scooters however, they are only recommended.
While the Muenster bicycle study and the European Commission for Monitoring Road Safety identified head injuries in 25% of bicycle incidents,19 20 ours and other studies reported considerably higher rates in E-scooter incidents, reaching up to 58%.5 8 10 12–15 17 18 21 23 Thus, an obligation for E-scooter riders to wear a helmet seems inevitable to improve safety. In this context, a study from Brisbane showed a significant reduction in head injuries with the introduction of mandatory helmets and the simultaneous handing out of helmets by E-scooter distributors.15 Nevertheless, it should be noted that in this investigation and in almost all international studies, approximately one-quarter of severe head injuries were severe midface fractures, which would most likely not have been prevented by classic bicycle helmets.5 8 10 12–15 17 18 21 23 24
Two international studies have described the musculoskeletal injuries after E-scooter incidents as the second most frequented cause in trauma surgery in 2019.16 17
In this study, fractures of the lower extremities were surprisingly rare; instead, soft tissue lacerations of the medial malleolus were frequently observed, which have not yet been described in the literature. These lacerations were caused by hitting the sharp-edged platforms or the protruding screws of the E-scooter’s rear wheel and could be reduced by technical modifications on the vehicle, such as rubber covers.
This study reports the largest cohort of patients involved in E-scooter incidents in Europe. Nevertheless, minor injuries may be under-represented because some patients were treated by general practitioners or did not demand medical care at all. The study was located in EDs in the Berlin city centre. Thus, different numbers and causes of incidents or injury patterns might be present in outlying districts. Also, the voluntary questionnaire was only handed out in two EDs and may show different results if given to a larger cohort.
Our results present the most frequent and serious injuries after E-scooter incidents. An obligation for E-scooter riders to wear a helmet, strict controls on rider’s alcohol consumption, the introduction of an age limit for riders and technical modifications to E-scooters should be considered in order to reduce incidents and injuries in the interest of all traffic participants.
Data availability statement
Data are available upon reasonable request. All collected data have been entered into an Excel data sheet and patient’s privacy information has been pseudonymised. The Excel document itself is password protected and saved upon a password-protected server of the Department of Emergency Medicine at Charité University Medicine Berlin with restricted access. Data protection is following the data protection declaration of the respective institution and will be available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the ethics committee of the Charité (EA2/171/19). Within the scope of patient registration and further analyses, compliance with ethical aspects and data protection regulations was ensured.
Footnotes
Handling editor Jason E Smith
Correction notice This paper has been updated to amend author name 'Martin Möckel'. The author Undine Gerlach has also been updated to include the middle initial A.
Contributors DU and UG contributed to the study conception and design, analysis, interpretation of data and writing of the manuscript. TL, MD, JWB, KB, AS and FJ participated in the acquisition and analysis of data. CW and MM contributed to the analysis and interpretation of data, the study conception and the critical review of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.