Article Text

Abstract
Aim To establish the national picture of prehospital anaesthesia in the UK and to reference practice against the Association of prior to Anaesthetists of Great Britain and Ireland safety guideline on prehospital anaesthesia.
Methods Lead clinicians were identified for all prehospital services in the UK that could potentially be performing prehospital anaesthesia and invited to complete a detailed online survey. The survey requested details on team structure, the process for prehospital anaesthesia, drugs and equipment used and training and governance arrangements.
Results 55 responses were received from 63 invitations sent (87.3%) yielding usable data for 47 services. 31 of the 47 services (70%) responded that they performed prehospital anaesthesia. All services performing prehospital anaesthesia utilised a doctor but only 18 services (58%) always utilised a trained assistant. 28 services (90%) maintained a database and over half of services (55%) performed less than 20 prehospital anaesthetics annually. 23 services (74%) had a designated lead clinician for prehospital anaesthesia and 25 (81%) had a written difficult airway plan. 19 services (61%) had mandatory continual training requirements.
Conclusions The majority of services are currently complying with the recommendations in the Association of prior to Anaesthetists of Great Britain and Ireland safety guideline. There are still areas of concern, particularly with regard to ongoing training and the high numbers of services that do not use a trained assistant for the process of prehospital anaesthesia.
Statistics from Altmetric.com
Introduction
Physician delivered prehospital care is a growing area of medicine within the UK. Historically, prehospital care in the UK originated as a voluntary service mainly delivered by general practitioners and other practitioners through schemes such as the British Association for Immediate Care (BASICS).1 Since the establishment of a Helicopter Emergency Medical Service in London in 1989, there has been a steady increase in the number of aeromedical systems in the UK able to provide physician delivered prehospital care.2 The recent NCEPOD (National Confidential Enquiry into Patient Outcome and Death) report ‘Trauma: who cares?’ recommended that trauma care in the UK needed to improve and that the concept of physician delivered prehospital care should be further developed.3 This view is fully supported by the Air Ambulance Working Group and the process is now underway to develop a curriculum with the view to creating a new medical subspecialty in the UK of prehospital emergency medicine.4 5
Prehospital trauma management however, remains an area of much controversy, especially with regard to issues such as time spent on scene, fluid resuscitation, team configuration and transport modality.6–9 One of the most controversial areas remains that of airway management and whether or not prehospital tracheal intubation, and specifically the use of drugs to facilitate tracheal intubation (variably termed rapid sequence intubation, drug assisted intubation or prehospital anaesthesia), is beneficial or harmful to the trauma patient.10 11 Additionally, there is conflicting evidence as to how, and by whom, this procedure should be performed.12 13 Carefully regulated randomised controlled trials in the prehospital environment are hugely challenging and consequently guidelines for prehospital practice are largely based on low grade evidence, consensus view and expert opinion.14–16 The recent publication in the UK of a safety guideline for prehospital anaesthesia by the Association of Anaesthetists of Great Britain and Ireland (AAGBI) has now established benchmark standards for performance of prehospital anaesthesia.17 This guideline uses the term prehospital anaesthesia to indicate the use of drugs to facilitate intubation in an out of hospital environment. Although recently published, we were interested in learning how many of the UK services undertaking prehospital anaesthesia are currently following the recommendations in this document.
We conducted a detailed survey of all services which potentially perform prehospital anaesthesia in the UK in an attempt to elicit which type of practitioner was doing prehospital anaesthesia, the processes and equipment being used and also the relative compliance with the recommendations in the new AAGBI safety guideline on prehospital anaesthesia.
Methods
This survey was anonymous and confidential, and no patient details were asked for or recorded. Ethics approval for the study was therefore not required, as per the COREC (Central Office for Research Ethics Committee) guidelines.
Initially we constructed a database of all services within the UK which could potentially provide physician delivered prehospital care. In England, Wales and Northern Ireland, we used the database of providers on the BASICS website (www.basics.org.uk) to identify all regional BASICS services in the UK. We also identified all air ambulance services in the UK as we felt that these services were the only likely services in which practitioners other than physicians might be performing prehospital anaesthesia. For each service we identified the lead clinician.
A detailed survey was constructed with questions relating to the performance by each service of prehospital anaesthesia, which we defined as the use of anaesthetic or other drugs to facilitate the placement of a tracheal tube in a patient outside of a hospital or healthcare facility. If the service responded that they never did prehospital anaesthesia, then the survey ended at this point. For services undertaking prehospital anaesthesia, there were further questions on the numbers of prehospital anaesthetics performed over a 12 month period, as well as the process, equipment and governance structure surrounding the performing of prehospital anaesthesia.
All questions were entered into a Survey Monkey online questionnaire (www.surveymonkey.com). An email invitation was sent to the lead clinicians for each service, requesting that they complete the survey on behalf of the service. The request specifically stated that the responses should represent those of the actual service and not the individual. We had previously identified that some lead clinicians worked for more than one service so we contacted these individuals to ensure that a separate response was completed for each individual service. If no response was received to the initial email request after 1 month, a further request was sent. Those services who did not respond to the second email request were contacted by telephone. If telephone contact revealed that the service no longer functioned, or that it did not perform prehospital anaesthesia, this was recorded and no further survey was sent.
No statistical analysis of the results was done and the results are presented in descriptive format.
Results
We identified 19 regional air ambulance services and 41 organised physician delivered, road based prehospital services in England and Wales. We identified one national air ambulance service and three road based services providing physician delivered prehospital care in Scotland as well as a secondary retrieval service which also provided aeromedical prehospital care. One road based service was identified in Northern Ireland, giving a total of 66 services.
Lead clinicians were identified for all 66 services but we were unable to make contact with three of the services. The survey was conducted over a 3 month period from June to September 2009, and invitations were sent to 63 of the 66 services (95.5%). A total of 55 complete responses were received from the 63 invitations sent (87.3%). Four services responded to say that their prehospital service was no longer in operation and in three cases there was a response from one individual regarding more than one service. No response was received from eight of the services and in one case the survey had been started but not completed thus leaving adequate completed data on a total of 47 prehospital services (figure 1).

Responses to survey invitation.
All aeromedical services responded to the questionnaire and a total of 27 of the remaining 43 road based services (62.7%) for whom we had contact details responded. Thirty-one of the 47 services who responded (66%) reported that they performed prehospital anaesthesia at least some of the time during which the service operated, with almost one-third (10 of 31) having the capability to do prehospital anaesthesia at all times which the service operated.
Fifteen of the services undertaking prehospital anaesthesia responded only by road, three responded only by air and 13 responded by both road and air. Fourteen of the 20 air ambulance services in the UK (70%) undertook prehospital anaesthesia at least some of the time during which the service operated.
Team configuration
Eight of the 20 air ambulance services (40%) always carried a physician as part of their prehospital response, with a further six services (30%) carrying a physician for some of the prehospital missions. Of the 15 road based services who undertook prehospital anaesthesia, 12 always carried a doctor, with three only sometimes having a doctor aboard. Only two of these 15 services (13%) were able to carry out prehospital anaesthesia at all times that the service operated, with the remainder depending on the skill mix available.
The majority of services able to undertake prehospital anaesthesia utilised doctors from a background of anaesthetics and emergency medicine (87.1%). Twenty-two services (80%) utilised general practitioners, with a smaller number of services utilising doctors from surgical (eight services) or medical (three services) specialties. No service employed practitioners who solely did prehospital care.
Eighteen services (58%) always utilised a trained assistant as part of the prehospital anaesthesia process; four had a trained assistant some of the times and nine services (29%) did not utilise a trained assistant. The type of practitioner used as the trained assistant by each service is shown in table 1.
Type and frequency of assistant for prehospital anaesthesia used among the services that utilise assistants (n=22)
Process of prehospital anaesthesia
The number of prehospital anaesthetics undertaken by each service is illustrated in figure 2. Twenty-five services (80.6%) used written guidelines for the process of prehospital anaesthesia and 22 (71%) used specific written indications for prehospital anaesthesia. Twenty services (64.5%) employed a checklist immediately prior to prehospital anaesthesia. Twelve services (38.7%) allowed non-physicians to intubate during prehospital anaesthesia. Cricoid pressure was routinely used by 29 (93.5%) services.

Annual number of prehospital anaesthetics carried out per service.
Drugs
Anaesthetic drugs carried by each service are summarised in table 2. The majority of services (64.5%) responded that the most commonly used anaesthetic induction agent was etomidate. The majority of services used a combination of midazolam and opioid for maintenance of anaesthesia (table 2). For the vast majority of services, the drugs were drawn up at scene prior to the emergency anaesthesia with only eight services (25.8%) drawing the drugs up at the start of each shift.
Anaesthetic drugs in prehospital services
Equipment and monitoring
All services carried some form of supraglottic rescue device, with the majority of services using a standard laryngeal mask airway LMA (90.3%). A small number of services carried I-gel supraglottic airway device (eight services) or LMA Proseal (five services) either instead of or in addition to a standard LMA. Two services utilised a Combitube and one service carried an intubating LMA. All services carried a gum elastic bougie and the majority (83.9%) also carried a stylet. Fifteen services (48.4%) had a written policy mandating the use of a bougie for prehospital anaesthesia. All services carried the necessary equipment to perform a surgical cricothyroidotomy, with eight services (25.8%) utilising a commercial kit and 23 (74.2%) carrying individual items. Eleven services (35.5%) carried a video or indirect view laryngoscope.
All services used ECG, SpO2 and non-invasive blood pressure monitoring, with the majority of services monitoring end-tidal CO2 both during (83.9%) and after (96.8%) prehospital anaesthesia. Eighteen services (58.1%) routinely used a colorific CO2 detector device. A total of 23 (74.2%) services utilised a mechanical transport ventilator after intubation.
Governance and training
Twenty-eight services (90%) maintain a database of all prehospital anaesthetics undertaken and 23 (74.2%) have a designated lead clinician for prehospital anaesthesia. The vast majority of services, 25 of 31 (80.6%), have a written difficult airway plan.
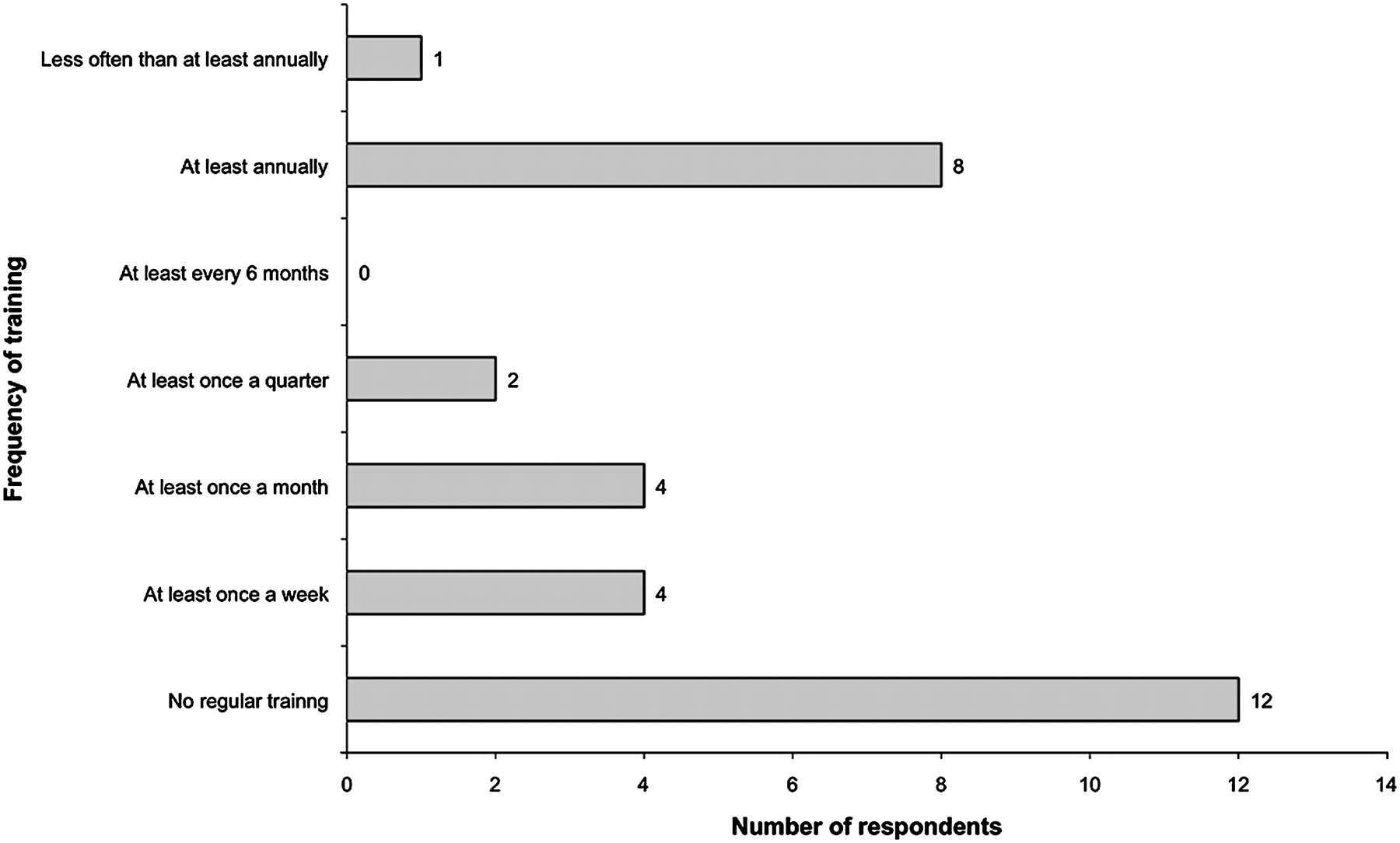
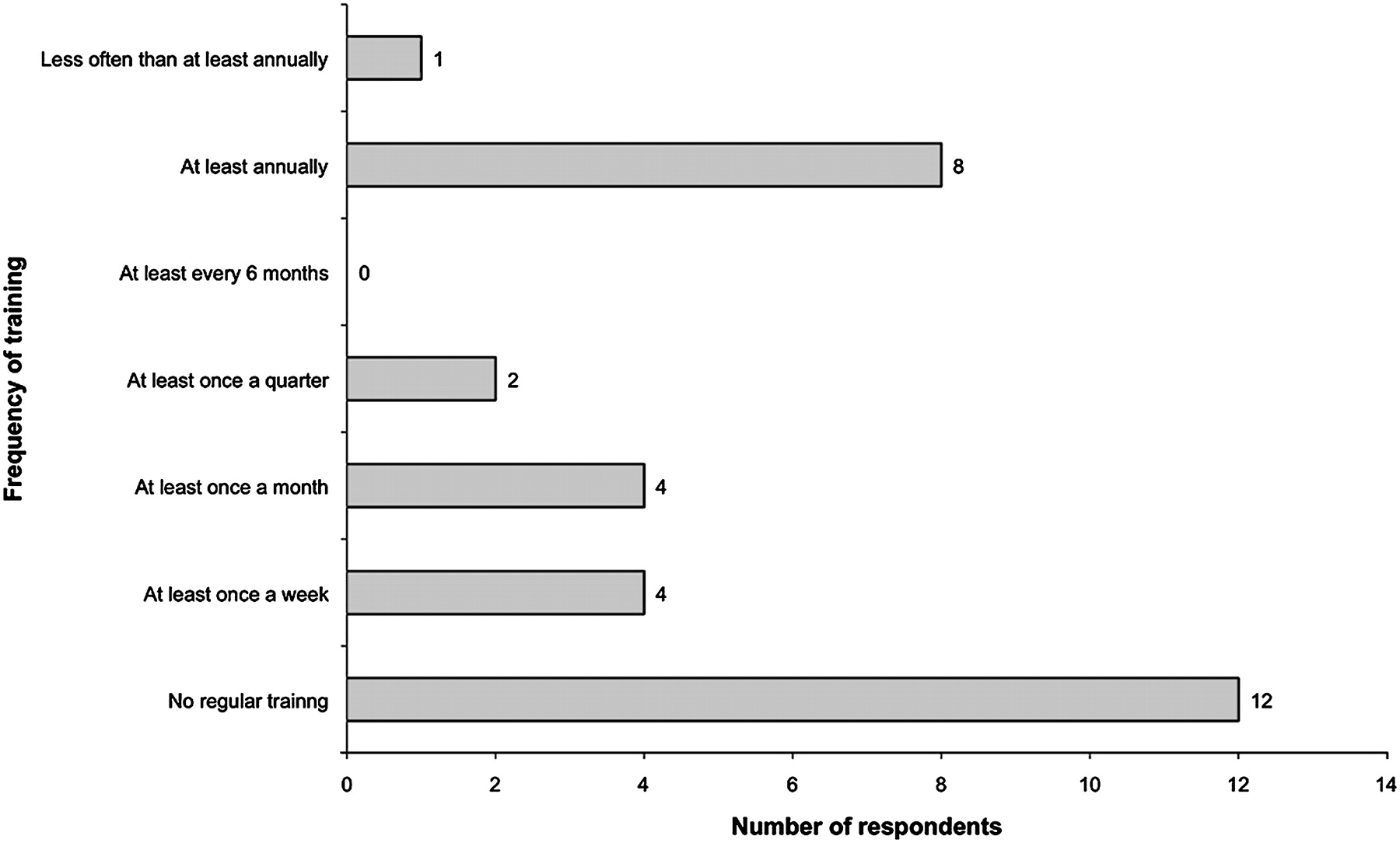
Twenty-six services (83.9%) responded stating that they require a minimum level of anaesthetic experience prior to undertaking prehospital anaesthesia and 19 services (61.3%) have mandatory continual training requirements. Figure 3 illustrates the frequency of training for the services and that 12 (38.7%) services have no regular training requirements. Thirteen services (41.9%) use a simulator and 20 services (64.5%) incorporate crew resource management or human factors training as part of the training process.
{kind=link}
{kind=link}
{kind=link}
Frequency of training for services undertaking prehospital anaesthesia.
Discussion
Our survey represents the most comprehensive review to date of current activity relating to prehospital anaesthesia in the UK. There are a total of 31 services in the UK that have the ability to perform prehospital anaesthesia, at least some of the time during which the service is active. Our survey demonstrated that prehospital anaesthesia in the UK is only provided by physicians, usually from a background of anaesthesia or emergency medicine.
Overall though, the UK is still lagging behind many other countries with regard to physician delivered prehospital care with 30% of air ambulances never carrying a doctor and a further 30% only utilising a doctor part of the time. By comparison, in other European, particularly Scandinavian countries, almost all regions provide 24 h physician delivered prehospital care.18–20 The development of the new curriculum and medical subspecialty training in prehospital emergency medicine in the UK may begin to redress this inequity.
One of the core skills for any practitioner of prehospital care is that of advanced airway management and the ability to facilitate intubation with the use of anaesthetic drugs. This procedure has been the focus of the most controversy within the literature and the evidence is conflicting. Earlier studies looked at the actual procedure of prehospital anaesthesia and compared subsequent patient outcomes or adverse events.10 11 21 There is now growing evidence that it is not the actual procedure of prehospital anaesthesia per se but the process and specifically the training and experience of the practitioner performing the procedure that affects patient outcome.12 13 22
Prehospital anaesthesia involves much more than simply placement of a tracheal tube. In addition to the unique environmental challenges posed in this arena, there are important factors such as the decision making process, communication and other non-technical skills to consider. With regard to the actual skill of intubation itself, there is good evidence that full competency is only achieved after approximately 50–60 intubations in a controlled environment.23 24 Given that this is well short of the number that most paramedics perform during their initial training and that most will subsequently do very few intubations each year, the Joint Royal College Ambulance Liaison Committee (JRCALC) has recommended that paramedics in the UK should no longer learn or perform intubation.25 26 The issues are even starker when paramedic prehospital anaesthesia is considered, with studies consistently demonstrating unacceptable levels of intubation failure, oesophageal intubation and high levels of adverse events.13 21
It is therefore no surprise that our survey demonstrated that in the UK, prehospital anaesthesia is performed only by physicians. While studies of physician performed prehospital anaesthesia have consistently demonstrated higher success rates and lower levels of complications than found in paramedic delivered systems, the key issues for any practitioner remain skill acquisition and skill retention.22 27–29 This is particularly pertinent as our study elicited the fact that many prehospital services perform a low number of prehospital anaesthetics per annum. The recent publication of the AAGBI safety guideline now provides a national set of standards for the UK practice of prehospital anaesthesia.17 The document highlights the importance of performing prehospital anaesthesia to the same standard as an emergency anaesthetic in the hospital environment, and that individual practitioners should have the necessary training to perform the skill to a level equivalent to those doing unsupervised emergency anaesthesia in hospital.
The vast majority of services in our survey (83%) require a minimum level of anaesthetic experience prior to undertaking prehospital anaesthesia and almost two-thirds provide regular ongoing training. Regular training is essential for skill maintenance, most importantly for those not performing regular emergency anaesthesia in the hospital setting. There is no clear evidence for an annual number of procedures to maintain the skill of prehospital anaesthesia but 10 has been suggested and the AAGBI guideline recommends about one per month.17 20 With recent literature supporting the view that simulator training reduces the number of safety critical events during prehospital anaesthesia, it is encouraging that 40% of services currently have access to a simulator for training.30 Similarly, with the growing evidence that effective team working can decrease the incidence of errors, it is reassuring that 20 of the 31 services (64%) have included human factors training.31 32
Many of the key recommendations in the AAGBI guideline were around the clinical governance structure supporting the process of prehospital anaesthesia. It is therefore very encouraging that the majority of services in the UK (74%) now have a designated lead clinician for prehospital anaesthesia, and most services utilise written guidelines and checklists. One in five services however still do not have a written difficult airway plan.
A specific recommendation in the AAGBI guideline is that a trained assistant should be utilised during prehospital anaesthesia. It is therefore concerning that this does not occur in almost a third of the surveyed UK services performing prehospital anaesthesia, and that only just over half of the services always use a trained assistant in the process. For those services utilising an assistant, in over two-thirds the assistant was a paramedic. Currently there is no standard training course for paramedics assisting with prehospital anaesthesia, although several courses have recently been developed along with a proposal to develop a national curriculum for critical care paramedics.
The AAGBI safety guideline makes a number of recommendations with regard to equipment and monitoring. As recommended, all services carried both a gum elastic bougie, at least one type of supraglottic device and the capability to perform a surgical airway. There were also high rates of compliance with the recommendation for minimal monitoring, with the vast majority of services utilising end-tidal CO2 monitoring.
In summary, we have demonstrated that the majority of services undertaking prehospital anaesthesia in the UK are currently operating to a high standard and are already fulfilling most of the recommendations made in the AAGBI safety guideline. It is very concerning however that there are still a large number of services who continue to practice prehospital anaesthesia without the use of a trained assistant, and over a third of services do not currently provide ongoing regular training for prehospital anaesthesia. Additionally, a small number of services could improve on the governance structure by designating a clinical lead for prehospital anaesthesia and implementation of guidelines and written difficult airway plans.
Acknowledgments
The authors would like to thank all of the clinicians who kindly took the time to complete the survey.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Primary survey