Article Text

Abstract
Objectives: Acute epiglottitis in adult is a potentially life-threatening condition that may be underdiagnosed. The present study reports the clinical features, management and patient outcomes in an acute hospital in Hong Kong over a seven-year period.
Method: All adult patients aged 18 years or above admitted to Tuen Mun Hospital between July 1999 and June 2006 with the diagnosis of acute epiglottitis were included in this retrospective study. The diagnosis of acute epiglottitis was established by direct visualisation of inflamed epiglottis during laryngoscopic examination.
Results: 106 patients were identified. A total of 21 patients (20%) had co-morbidities, with diabetes mellitus (11%) being the most common. Five patients had a history of nasopharyngeal carcinoma and three patients had a previous history of acute epiglottitis. The majority (94%) of patients presented with sore throat as their major complaint. Blood cultures were collected from 15 patients and all were negative. A combination of cefotaxime and metronidazole was the most common empirical antibiotic regimen prescribed. Seven patients required active airway intervention (six with endotracheal intubation and one failed intubation with emergency tracheostomy performed). No mortality was reported.
Conclusion: Acute epiglottitis in adults is not a rare entity and vigilance for this condition is needed. In general, the prognosis is good with antimicrobial therapy, close monitoring and selective airway intervention.
Statistics from Altmetric.com
Acute epiglottitis, which is a form of acute inflammation of the epiglottis and adjacent structures, is a potentially life-threatening condition in which a previously healthy patient may develop lethal upper airway obstruction within hours. In the past, acute epiglottitis was described as a disease of childhood. The incidence in childhood has, however, declined, whereas there is an increased recognition of adults with this condition after massive immunisation against Haemophilus influenzae B.1 2 Mayo-Smith et al2 postulated that adult acute epiglottitis might be a distinct form of disease for which the aetiological agents could not be identified from blood cultures and specimens collected from the inflamed epiglottis and supraglottic areas. The authors also suggested that the term “supraglottitis” might be more appropriate as the surrounding supraglottic structures were also involved in most cases. The objective of this study was to review the cases of adult acute epiglottitis admitted to a regional hospital in Hong Kong during a seven-year period.
STUDY METHOD
We used the International Classification of Diseases version 9 code to identify adult patients aged 18 years or older admitted to Tuen Mun Hospital, the only acute hospital with 1600 beds serving a population of approximately one million in the north-western part of Hong Kong, between July 1999 and June 2006. Information regarding demographic data, presenting features, investigation results, antimicrobial therapy, airway interventions and treatment outcomes was collected from a retrospective medical record review. The diagnosis of acute epiglottitis was established by direct visualisation of inflamed epiglottis by either flexible nasopharyngolaryngoscopy, indirect or direct laryngoscopy.
RESULTS
A total of 107 adult patients were diagnosed with acute epiglottitis during the study period. As we considered direct visualisation of the inflamed epiglottis the gold standard of diagnosis, one patient without laryngoscopy performed was excluded from further analysis. Diffuse oedema and swelling of the epiglottis was seen in all 106 patients during larynogoscopic examination. Coexisting epiglottic cysts were observed in 12 patients (11%).
Demographic characteristics and clinical features
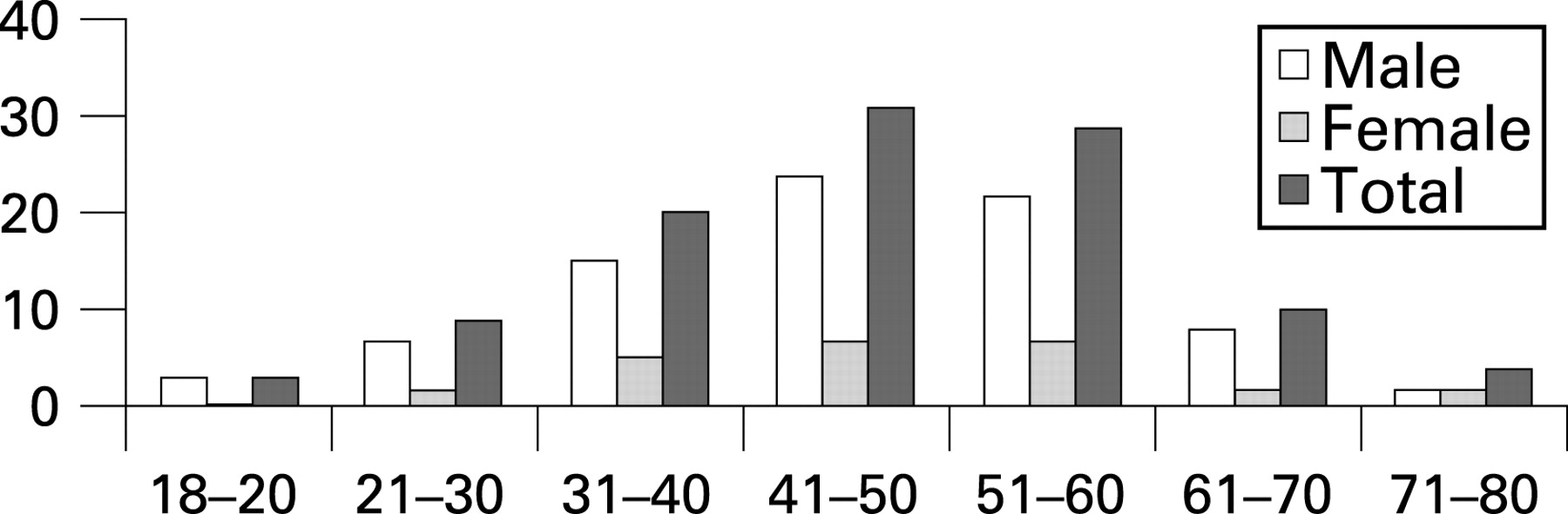
Demographic data are presented in fig 1 and table 1. There was no obvious seasonal variation in the incidence of disease. The majority (94%) of patients presented with sore throat as their major complaint (n = 100). Other common symptoms included fever (n = 43), odynophagia (n = 39), dysphagia (n = 31), dyspnoea (n = 24) and hoarseness of voice (n = 21). Five patients (4.7%) developed stridor. Five patients were able to recall a recent history of upper respiratory tract infection, whereas five could recall a history of foreign body ingestion. Sixty-nine patients (65%) presented within two days of symptom onset but 10 patients (9%) presented with a delay of more than one week (range 1–28 days).

{kind=link}
Radiological investigations
Seventy-one patients had a lateral neck radiograph performed. In these patients, the “thumb sign” was documented in the medical records of 55 patients (77%) but the “vallecula sign” was mentioned in only one patient. One patient had a foreign body shown on the radiograph.
Microbiological investigations
Blood cultures were collected from 15 patients. All were sterile after incubation for five days. Respiratory specimens (sputum or endotracheal aspirate) and throat swabs were collected from nine and five patients, respectively. No pathogens were identified in seven respiratory specimens and five throat swabs. Non-typeable H influenzae was identified in the endotracheal aspirate from one intubated patient and Mycobacterium tuberculosis was identified in the sputum specimen of one patient.
Antimicrobial therapy
All patients received intravenous antibiotics initially. The most common empirical antimicrobial therapy was a combination of third generation cephalosporin (cefotaxime) and metronidazole, which was given to 92 patients (87%) as the initial antimicrobial therapy. Thirty-six patients received oral cefuroxime and metronidazole, whereas 37 patients received amoxicillin–clavulanate as their oral maintenance therapy. The mean duration of antibiotic treatment was 11.61 days (range 3–28 days).
Airway intervention
Ninety-nine patients did not require any airway support during their illness, whereas seven patients (6.6%) required an artificial airway. Six patients required endotracheal intubation within 24 h after admission (range 3–24 h). All patients were extubated within seven days. One patient had an emergency tracheostomy for failed intubation within one hour after admission.
Clinical progress and outcome
Fifty-five patients (52%) were admitted to the intensive care unit (ICU) for close monitoring. For this group of patients, the mean length of ICU stay was four days (range 1–10 days). One patient developed an epiglottic abscess and three patients developed infected epiglottic cysts that required surgical drainage. There was no mortality in this case series. The mean hospital stay was 6.76 days.
DISCUSSION
This is the first large case series of acute epiglottitis of adults in Hong Kong. We encountered a significant number of patients within our study period, which implies that adult acute epiglottitis is not an uncommon disease entity. The increased awareness of doctors and greater availability of flexible nasolaryngoscopy may also contribute to the apparent increase in the incidence of acute epiglottitis in adults. A significant proportion presented with symptoms such as sore throat and fever, without respiratory distress or features suggestive of upper airway obstruction such as drooling of saliva and stridor. These cases would be misdiagnosed as common upper respiratory tract infection if laryngoscopic examinations were not performed. We suggest that doctors should remain vigilant for acute epiglottitis and seek early advice from otolarynologists in patients with sore throat that cannot be accounted for by findings during the bedside oropharyngeal examination.
A well-performed lateral neck radiograph may be used as a diagnostic tool for acute epiglottitis and several qualitative radiological features are helpful in making the diagnosis.3 The “thumb sign” is one of the classic radiological findings in acute epiglottitis. It is actually a rounded mass shadow of the normal leaf-like epiglottis resulting from the thickening and oedema of the inflamed epiglottic tissue. Another radiological feature of acute epiglottitis is the “vallecula sign”, which is the result of partial or complete obliteration of a well-defined air pocket bounding the base of the tongue and the epiglottis. The “vallecula sign” may be useful in improving diagnostic sensitivity and specificity.4 In our case series, the “thumb sign” was present in 77% of patients who had a lateral neck radiograph performed. The “vallecula sign” was, however, observed in only one patient, which suggests that this specific radiological feature of acute epiglottitis is still not very well recognised by our local colleagues.
In the present study, more than half of the patients had been admitted to the ICU for close monitoring and had an average stay of four days. The ICU is the ideal place for the close monitoring of patients with acute epiglottitis as experienced nursing staff and personnel skilled in airway management are available.
Airway management is one of the most important and controversial aspects in managing acute epiglottitis. On one hand, some experts advocate airway protection as an initial management.5 The rationale for early airway intervention before signs of airway obstruction occur is the lack of reliable criteria for discriminating patients who may develop a sudden airway obstruction from those who will follow a benign course. On the other hand, there is a recent trend towards adopting a more conservative approach, with medical therapy and close patient monitoring, whereas active airway intervention was performed only for selected patients.6–8 Park et al9 suggested that routine prophylactic intubation appeared unnecessary for adult patients with acute epiglottitis without severe respiratory distress at presentation. Various studies have also been performed to identify predictive factors for the need for airway intervention. A combination of features such as stridor, drooling, acute onset or rapid progression, hoarseness, respiratory distress, dyspnoea, chest wall retractions and upright position have been associated with the need for airway intervention.2 8 A classification system (table 2) has been developed to help clinicians to decide the need for an artificial airway10 and some authors recommended creating an artificial airway in Friedman stages II to IV.6 Katori et al11 found that symptoms of stridor and muffled voice, a rapid clinical course and diabetes mellitus were the factors associated with airway intervention. They also found that extreme severe epiglottic swelling, in which only less than half of the posterior vocal folds can be visualised (scope classification III) and extension of the swelling to the arytenoids (scope classification B) were factors strongly associated with airway intervention. In our study, active airway intervention was performed for seven patients only. Six patients underwent endotracheal intubation. Emergency tracheostomy was performed for one of these patients as endotracheal intubation failed. Ninety-four per cent of our patients received medical therapy but we did not encounter any mortality. As active airway intervention is not without risk, we recommend a conservative approach with endotracheal intubation in selected cases. The equipment and expertise for emergency tracheostomy, however, need to be readily available as a last resort for securing a patent airway.
CONCLUSION
Acute epiglottitis in adults is not a rare entity and we need to remain vigilant for this condition. In general, the outcome is good and a conservative approach with antibiotic therapy should be adequate for most patients. Close monitoring is essential to detect those patients requiring active airway intervention. Selective intubation of patients should be considered in patients presenting with rapid clinical progression, features suggestive of upper airway obstruction, respiratory distress and laryngoscopic findings of severe epiglottic swelling and arytenoid involvement.
REFERENCES
Footnotes
Competing interests: None declared.
Linked Articles
- Primary survey