
Abstract
Background
This prospective, randomized double-blind study, conducted over 19 months in a tertiary care ED, sought to determine if a fascia-iliaca regional anesthetic block provides better and safer pain relief than does parenteral analgesia.
Aims
This study also aimed to determine the effectiveness of parenteral NSAID analgesia for acute hip fractures.
Methods
Patients >65 years old presenting at an adult ED with acute hip fractures were randomized upon presentation to the ED into two groups (A and B) using numbers generated by the EPI-INFO™ (Atlanta, GA: Centers for Disease Control and Prevention) program. The randomization list was kept by one of the authors who did not interact with the patients. Two groups of patients were to receive either (A) a fascia-iliaca block with bupivacaine and parenteral saline injection, or (B) the same block with saline and an IV NSAID injection. Upon admission to the study, vital signs such as blood pressure, mean blood pressure (MAP), heart rate (HR), respiratory rate (RR) and pain-intensity measurements [using the Visual Analogue Scale (VAS)] were obtained and repeated at 15 min, 2 h and at8 h. The occurrence of complications was registered.
Results
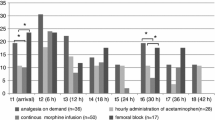
One hundred seventy-five patients were randomized, and 21 were excluded from participation. The remaining 154 patients were grouped as: group A (n = 62) or group B (n = 92). The mean pain level on admission to the ED for all patients, assessed with the VAS, was 8.21 ± 0.91 (CI 95%: 6.43–9.99); in group A the VAS was 7.6 ± 0.22 and in group B 8.5 ± 0.72 (p = 0.411). At 15-min evaluation, values were: group A 6.24 ± 0.17 and group B 2.9 ± 0.16 (p < 0.001). At the 2-h assessment, values were: group A 1.78 ± 0.11 and group B 2.3 ± 1.16 (p = 0.764). At 8 h the VAS for group A was 2.03 ± 0.12 and for group B 4.4 ± 0.91 (p = 0.083).
Conclusion
This study demonstrates that: (1) parenteral NSAIDs are very effective as analgesics after hip fractures in elderly patients, (2) fascia-iliaca regional blocks are nearly as effective for up to about 8 h after administration and (3) regional fascia-iliaca blocks effectively control post-hip fracture pain. (4) Fascia iliaca regional block has a rapid onset.
Similar content being viewed by others
Introduction
Background
In the US, hip fracture is a common event, especially in the elderly. The incidence of hip fractures is 517 fractures/100,000 person-years, with about 76% occurring in women [1]. Hip fracture rates increase exponentially with age in both men and women [2]. People ≥85 years old are from 10 to 15 times more likely to sustain hip fractures than are people aged 60 to 65 years [3]. In 1997, treatment-associated costs of hip fractures were estimated to have exceeded $20 billion [4].
Miller reported that the seriousness of hip fractures to overall patient health is reflected in these patients’ 16-day mean hospital stay, an in-hospital mortality of 5% and a 3-month mortality of 10% [5].
Inadequate pain relief contributes to delayed recovery from hip fractures [6]. Opiates often have unforeseeable neurological effects in the elderly because of the high prevalence of pre-existing cognitive deficits and vascular neurological disorders. Opiates also cause severe constipation and nausea (vomiting, when associated with neurological deficit, may lead to life-threatening aspiration pneumonia). In addition, opiates may potentially have harmful cardiovascular and respiratory effects.
To help lessen such complications, the standard of care in many parts of the world is to use parenteral non-steroidal anti-inflammatory drugs (NSAIDs) instead of narcotics as the first-line analgesic in patients with hip fracture. On the other hand, NSAIDs predispose patients to gastrointestinal bleeding, consequently increasing anemia and raising the number of transfusions; this too can cause various kinds of renal damage and refractory hypertension [7].
An alternative to avoid the above-mentioned systemic complications of both opioids and NSAIDs is to control pain using a regional block. Two such blocks, the femoral block and the fascia-iliaca (iliofascial) block, are often used to control postoperative pain. The fascia-iliaca (iliofascial) block has been shown to be easy and safe to use in the ED [9]. This block also avoids the complications of the more common femoral block (prolonged motor block, inadvertent arterial puncture, direct nerve damage) [7–9]. While it can be used to control postoperative pain, ED management is concerned with preoperative analgesia.
Goals of this investigation
This study aimed to determine if a fascia-iliaca regional anesthetic block provides better and safer pain relief than does parenteral NSAID analgesia, and whether parenteral NSAIDs are effective analgesics in these situations.
Material and methods
Setting
This prospective randomized double-blind, cross-sectional study was performed during a 19-month period (June 2006 to January 2008) in the ED of a tertiary referral center. The ED has a residency program with 120,000 consultations a year. The study was approved by the institution’s teaching and research committee.
Study design
For calculation of the sample size, a difference of 2 ± 0.8 points in the VAS scale is considered clinically significant. To detect differences in the rate of adverse effects between groups, considering a 30% incidence in group A vs. a possible 10% incidence in group B with the same error levels, 62 patients were required without continuity correction, and 72 patients were required for Fisher's exact test.
As soon as the diagnosis of hip fracture was made and before an analgesic was administered, the patient or their legal decision-maker was informed about the study. If they agreed to participate, they signed an informed consent form.
Patients were randomized into two groups (A and B) using numbers generated by the EPI-INFO™ (Atlanta, GA: Centers for Disease Control and Prevention) program. The randomization list was kept by one of the authors who did not interact with the patients. He gave instructions to the patient’s ED nurse about which treatment should be administered. The nurse prepared the medication following the physician’s instructions and assigned a letter to the protocol (from a set of 10 letters, 5 for group A and 5 for group B) that designated whether the patient was receiving active medications in the fascia-iliaca block. The physician administering the medications and obtaining the VAS scores did not know which medications the patient was receiving.
Selection of participants
Our patient pool consisted of adult patients more than 65 years old who presented to the ED because of a previously undiagnosed and untreated hip fracture.
Exclusion criteria for the study included anatomical abnormalities in the inguinal area different from fracture, known coagulation disorders, a history of allergy to any of the active ingredients used during the study and refusal to participate.
Patient measurements
The protocol included observing patients for 8 h. Upon admission to the study, vital signs such as blood pressure, mean blood pressure (MAP), heart rate (HR), respiratory rate (RR) and pain-intensity measurements [using the Visual Analogue Scale (VAS)] were obtained. Vital signs and VAS-based pain measurement evaluations were performed at 15 min, 2 h and 8 h. (Vital signs were also taken at intermediate times for clinical purposes.) The occurrence of adverse effects or complications was concomitantly evaluated in all patients.
Interventions
A peripheral IV was placed in all patients for the administration of analgesia and hydration. A single fascia-iliaca compartment block [9–11] was performed on all patients with either 0.9 normal saline (group A) or 0.3 ml/kg 0.25% bupivacaine (group B). Patients in group A received IV NSAID analgesics (Diclofenac or Ketorolac, depending on their medical history), whereas those in group B had 3 ml to 5 ml 5% dextrose administered IV.
A fascia-iliaca block is performed by identifying the inguinal ligament and the femoral artery. A 21-g, 2-inch intramuscular injection needle is inserted perpendicular to the skin at a point 1 cm below the juncture of the lateral and medial two-thirds of a line that joins the pubic tubercle to the anterior superior iliac spine. The needle is inserted until a loss of resistance is felt as the fascia lata is passed, and then further advanced until a second loss of resistance occurs when the fascia iliaca is pierced (often described as two “pops”) [9]. After aspirating to assure that the needle is not in a vessel, solution is injected.
Outcome measures
The primary measurement used was VAS to determine pain scores in the two groups. The patients’ vital signs over the course of the study period were used as secondary measurements.
Primary data analysis
The general characteristics of the entire study sample and of each subgroup were calculated for mean age, sex, co-morbidities, vital signs and VAS. Quantitative data were reported as mean ± standard error regardless of the distribution of the variables. Variables such as sex, prevalence of co-morbidities and side of fracture were dichotomized into present or absent.
Baseline VAS scale values and vital sign data were compared to data obtained at 15 min, 2 h and 8 h in an independent manner. The Student’s t-test for paired samples was used for these continuous quantitative values. When the same values were compared between groups A and B, the Student’s t-test was used for each comparison at 15 min, 2 and 8 h, and an ANOVA curve was used for sequential comparison. Complications such as vomiting, nausea and hematoma at the injection site were dichotomized as present or absent, and were compared at 8 h using Fisher’s exact test. For statistical inference, a type I error of 0.05 and a power of 80% was assumed.
The statistical analysis was performed using the Primer of Biostatistics 4.0 software (McGraw Hill, 1996) and the Statistix 7.0 analytical software (2000).
Results
Characteristics of study subjects
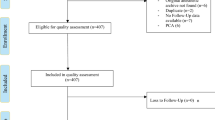
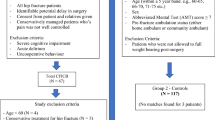
One hundred seventy-five patients were randomized upon presentation to the ED. A total of 21 were excluded from participation (1) because they or their legal decision-maker declined to participate, (2) due to systemic or laboratory abnormalities that interfered with their participation or (3) because they were subsequently found to have missing data (VAS not recorded or incomplete vital signs on scheduled measurements). The remaining 154 patients already had been randomly assigned to either group A (saline blocks with parenteral treatment for pain; n = 62) or group B (bupivacaine blocks; n = 92).
The demographic characteristics and baseline clinical status of the study patients are shown in Table 1. No statistical differences were found between the two study groups or between the initial two groups chosen before patients were eliminated from the study. Aside from the hip fracture, the most common additional clinical conditions found in the study patients were hypertension, diabetes, anemia, cancer, ischemic heart disease and chronic cognitive impairment at different stages. Of all these patients, 130 (85%) had more than one concomitant condition. The mean pain level on admission to the ED for all patients, as assessed with the VAS, was 8.21 ± 0.91 (CI 95%: 6.43–9.99); this is categorized as severe pain. There were no patients who described a maximal pain level (10 points): admission pain levels ranged from 5 to 9 in group A and 4 to 9 in group B.
Main results
Table 2 describes patient VAS and autonomic responses to the two analgesic interventions over the 8-h study period. Despite the difference in the final number of patients in the two study groups, there were no statistically significant differences between their demographic characteristics or their baseline parameters.
Patient pain assessment showed that while both the parenteral NSAID group (A) and the fascia-iliaca block (B) group demonstrated a significant analgesic effect, the parenteral block was much more effective at 15 min (p = 0.001), although both groups showed significant analgesia effects compared to baseline. At 2 h, analgesia effectiveness was statistically similar in both groups (p = 0.764).
Analgesic effects were maintained in both groups at 8 h, although at 8 h, pain intensity was somewhat higher in group B than in group A. The difference at 8 h, however, was not statistically significant (p = 0.083).
The autonomic parameters measured during the study (heart rate, respiratory rate, mean blood pressure) showed that they paralleled the VAS findings.
Complications
During the 8-h study period, some clinical derangements were seen beginning at 2 h after analgesic administration. They markedly diminished by 8 h.
The overall incidence of adverse effects during the study period was 0.177 (11/62 patients) for group A and 0.032 (3/92 patients) for group B. In group A, there were four episodes of delirium, two of nausea, and two of nausea and vomiting. It was unclear if these had any relation to the medication administration. Three local bruises occurred at the site of injection of the placebo (group A). In group B, the only complications were local bruises at the site of injection.
Including all the adverse events, the difference-in-proportions test was significant (p = 0.005) between the two groups.
Limitations
Due to a randomization before enrollment, the number of patients in the two study groups was dissimilar. Nevertheless, there were no statistical differences between either their demographics or their baseline clinical parameters.
Since the treating nurse was aware of the randomization group, it is possible that s/he could have biased the patient or the treating provider, consciously or otherwise. The sample size was calculated on the basis of complications only. Distracting injuries were not recorded.
Discussion
Good emergency care requires early and effective management of hip fracture pain. In this study, we found that fascia-iliaca blocks seem to provide at least equivalent relief to patients without causing unwanted and potentially deleterious side effects.
The lack of maximum pain scores in the study population may have been because of the high prevalence of co-morbidities observed in the study group. It could be that the patients had previously experienced more intense pain than that from the hip fracture or that their pain was attenuated by the peripheral or even central neurological disorders (convergence phenomenon) of the co-morbidities and by age. These underlying medical conditions may have also caused the falls that resulted in the patients’ fractures, an association clearly established in the literature [1].
When administering parenteral analgesics to patients with hip fractures, we follow the practice standard used throughout Argentina: that is, first to administer parenteral NSAIDs, and, if the pain does not lessen substantially, opioids are given. While none of our study patients rated their pain intensity as a VAS score of 10 (maximum tolerable pain), values above 8 generally indicate that opioids should be administered. In our study, we did not need to use opioids because of the reduction of pain levels obtained with the fascia iliaca block.
Fascia-iliaca blocks, a routine practice in our ED, are easily learned, much safer than the commonly used femoral blocks and well-tolerated [9]. They can be done with commonly available equipment and should be part of all emergency physicians’ skill sets.
An analgesic effect from both interventions was evident at 15 min, although it was much more significant in group B (regional block). By 2 h after administration, both groups had achieved similar pain relief, but at 8 h, the block’s effects were wearing off. The change in patients’ autonomic responses to pain generally followed their reported pain levels. No clinical complications attributed to either of the analgesic agents were observed during this period.
Further study is needed to evaluate the possible synergic activity of NSAIDs and fascia iliaca block in pain management for patients with hip fracture.
Conclusions
This study demonstrates that: (1) parenteral NSAIDs are very effective as analgesics after hip fractures in elderly patients, (2) fascia-iliaca regional blocks are nearly as effective for up to about 8 h after administration, and (3) regional fascia-iliaca blocks effectively control post-hip fracture pain—without narcotics’ deleterious side effects. (4) In the ED, by significantly reducing pain, fascia-iliaca regional blocks can permit more rapid assessment and diagnostic procedures in the ED.
References
National Center for Health Statistics, Trends in Health and Aging. http://www.cdc.gov/nchs/agingact.htm. Accessed on April 22, 2008.
Samelson EJ, Zhang Y, Kiel DP, Hannan MT, Felson DT (2002) Effect of birth cohort on risk of hip fracture: age-specific incidence rates in the Framingham Study. Am J Public Health 92(5):858–862
Scott JC (1990) Osteoporosis and hip fractures. Rheum Dis Clin North Am 16(3):717–740
Braithwaite RS, Col NF, Wong JB (2003) Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc 51(3):364–370
Ray NF, Chan JK, Thamer M, Melton LJ III (1997) Medical expenditures for the treatment of osteoporotic fractures in the United States in 1995: report from the National Osteoporosis foundation. J Bone Miner Res 12:24–35
Bonica JJ (1987) Importance of effective pain control. Acta Anaesthesiol Scand 31 (suppl 85):1–16
Lopez S, Gros T, Bernard N, Plasse C, Capdevila X (2003) Fascia iliaca compartment block for femoral bone fractures in prehospital care. Regional Anesthesia and Pain Management 28(3):203–207
Khoo ST, Brown TCK (1983) Femoral nerve block: the anatomical basis for a single injection technique. Anesth Intensive Care 11:40–42
Monzon DG, Iserson KV, Vazquez JA (2007) Single fascia ilíaca compartment block for post- hip fracture pain relief. J Emerg Med 32(3):257–262, Epub 2007 Feb 8
Haddad FS, Williams RL (1995) Femoral nerve block in extracapsular femoral neck fractures. J Bone Joint Surg 77:922–923
Finlayson BJ, Underhill TJ (1988) Femoral nerve block for analgesia in fractures of the femoral neck. Arch Emerg Med 5:173–176
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
The views expressed in this paper are those of the author(s) and not those of the editors, editorial board or publisher.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Monzón, D.G., Vazquez, J., Jauregui, J.R. et al. Pain treatment in post-traumatic hip fracture in the elderly: regional block vs. systemic non-steroidal analgesics. Int J Emerg Med 3, 321–325 (2010). https://doi.org/10.1007/s12245-010-0234-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12245-010-0234-4