
Abstract
Introduction
Hypoglycemia is a common side effect of insulin therapy and has negative implications for quality of life and healthcare resources. The authors investigated the self-reported frequency of non-severe and severe hypoglycemic events (NSHEs and SHEs), hypoglycemia awareness, patient–physician communication, health-related effects and economic impact on people with insulin-treated diabetes (Type-1 and Type-2) in Spain.
Methods
People with Type-1 (T1DM) or insulin-treated Type-2 (T2DM) diabetes older than 15 years of age completed up to 4 questionnaires at weekly intervals. NSHE was an event which respondents could manage without assistance. SHE needed help from a third party to manage.
Results
In total, 630 respondents completed questionnaires covering 2,235 weeks. Mean self-reported NSHEs per respondent-week were 1.7 (T1DM) and 0.4–0.8 (T2DM). Impaired hypoglycemia awareness or unawareness was reported by 55% of T1DM and 39% of T2DM respondents. Overall, 31% of T1DM and 20% of T2DM respondents rarely/never informed their physician about NSHEs. Respondents reported feeling tired/fatigued after 67% of NSHE and less alert after 45% of NSHE. Over the week following an NSHE, blood glucose measurement test-strip use increased by 5.3 (mean). In employed respondents (43%), 18% of NSHEs were reported to lead to lost work time (mean 1.5 h per event). After an SHE, 49% of respondents required emergency visits and/or hospital admission.
Conclusion
NSHE are a common occurrence with T1DM and insulin-treated T2DM in Spain and are associated with a cost burden and negative impact on well-being. Patient–physician communication is higher in Spain than Europe overall; however, many patients expressed reluctance to discuss their hypoglycemia.
Similar content being viewed by others
Introduction
The prevalence of diabetes is increasing and according to the International Diabetes Federation (IDF), more than 3.8 million adult citizens currently live with diabetes in Spain, corresponding to a prevalence of 10.8% (2013 estimate) [1]. Other studies have estimated a slightly higher prevalence of diabetes (≤15%) [2], the most recent reporting a prevalence of 13.8% in a representative sample of the Spanish population [3].
Maintenance of normoglycemia, often through the use of insulin, is the cornerstone of optimal diabetes management. However, intensification of insulin therapy can lead to an increased incidence of hypoglycemia: the most common adverse event associated with insulin treatment [4]. Hypoglycemic episodes are defined as either severe or non-severe depending on whether assistance is required by another individual, or whether the person can manage the event alone, respectively [5, 6]. Non-severe hypoglycemic events (NSHEs) account for 88–98% of all events [7–9] and have been shown to impact the health-related quality of life of people with diabetes [7, 10]. Furthermore, the rise in the prevalence of diabetes may also create problems for healthcare systems as hypoglycemia can have a direct and indirect economic impact [11].
Hypoglycemia also represents a barrier to optimal diabetes management, as fear of hypoglycemic events can cause sub-optimal insulin therapy and poor glycemic control [12, 13]. Although international diabetes bodies (the European Association for the Study of Diabetes and the American Diabetes Association) highlight that education on the recognition and treatment of hypoglycemia is an important part of diabetes management, the real-world level of patient–physician communication regarding hypoglycemia is not known [14].
There are limited data on the frequency of hypoglycemia outside of clinical trial settings and, furthermore, there are few studies reporting data for NSHEs in people with Type 1 Diabetes Mellitus (T1DM) and Type 2 Diabetes Mellitus (T2DM) in Spain. Previous European studies have reported real-world estimates [8–10, 15]; however, results vary according to the definition of events used, methods of data collection, and country coverage. Moreover, limited data exist on the health-related impact and the use of healthcare resources due to NSHEs in Spain.
This paper reports the frequency of self-reported NSHEs and severe hypoglycemic events (SHEs) in people with T1DM and insulin-treated T2DM in Spain. Additionally, levels of impaired hypoglycemia awareness, patient–physician communication of hypoglycemic events and the health-related effects and economic impact of NSHEs are reported.
Methods
Subjects
A full description of the methodology for this study has been previously reported by Östenson et al. [16]. Respondents in Spain were recruited using existing large consumer panels that provided a representative sample of the general diabetes population. People over the age of 15 with a T1DM or T2DM diagnosis, receiving insulin, were included in the survey. Respondents with T2DM were divided into three subgroups based on regimen: long acting insulin only (basal only therapy; T2BOT), short and long acting insulin (basal bolus; T2BB) or other insulin regimens (e.g., premix; T2O).
A small incentive (5€) was offered for completion of the questionnaire, in line with current market research guidelines and to ensure that there was no undue incentive to participate. Questionnaires were completed anonymously in accordance with the regulations and practice of market research governing bodies European Society for Opinion and Marketing Research (ESOMAR) [17] and European Pharmaceutical Market Research Association (EphMRA) [18].
Materials: Online Questionnaires
Four waves of questionnaires were sent out over 4 weeks. The first questionnaire collected information on respondent demographics and patient awareness of hypoglycemia. It also collected the self-reported number of NSHEs in the preceding seven days and the number of SHEs in the past year. The subsequent three questionnaires recorded the frequency of NSHEs in the preceding seven days only. Data on the impact of hypoglycemia (particularly NSHE; based on a respondent’s last NSHE within the 7-day recall period) on respondent well-being, work productivity and healthcare resource use were also collected. The questionnaire was based on one used in a previous study, [19] which was created using insights collected during focus groups on the self-reported impacts of hypoglycemia [20]. Adaptations made to the questionnaire for this study included questions on frequency.
Definitions and Calculations
An NSHE was defined as symptoms of hypoglycemia (e.g., sweating, shaking, and headache) with or without a blood glucose measurement, or a low blood glucose measurement (≤3.1 mmol/L) without symptoms, that the individual managed without assistance. An SHE was defined as an event of low blood glucose level (≤3.1 mmol/L) needing help from a third party to manage (e.g., help from a family member or a health care professional, including emergency room visits and hospitalization).
Weekly NSHE frequencies were calculated using data from all respondents completing at least one questionnaire (wave) with annual frequency calculated using the mean weekly event frequency multiplied by 52. Standard descriptive methods (means/percentage and standard deviations) were used to report results for respondents.
The classification system for awareness of hypoglycemia was based on a prospectively validated study by Pedersen-Bjergaard et al. [21]. Any respondent who answered ‘sometimes’ or ‘never’ to the question “can you feel when your blood sugar is low?” was assigned as being unaware of hypoglycemia, those who answered ‘usually’ as having impaired awareness and those who answered ‘always’ deemed to be aware. Comparisons of NSHE frequencies according to respondent awareness were performed using t tests with an employed significance level of p < 0.05.
This was a non-interventional market research study. Questionnaires were completed anonymously in accordance with the regulations and practice of market research governing bodies: European Society for Opinion and Marketing Research (ESOMAR) and European Pharmaceutical Market Research Association (EphMRA). The EphMRA Code of Conduct states that Market Research does not require Clinical Research Ethics Committee or Independent Review Board approval.
This article does not contain any new studies with human or animal subjects performed by any of the authors.
Informed consent was obtained from all patients for being included in the study.
Results
Subjects
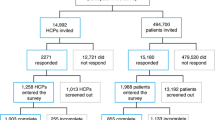
The 630 patients entering the study completed in total 2,235 patient-week records with 90, 85 and 80% completing wave two (570 patients), wave three (534 patients) and wave four (506 patients), respectively. The frequency of NSHEs is based on 2,235 respondent-week records.
Demographics for respondents are shown in Table 1. In total, 47% of respondents had T1DM and 53% of respondents had T2DM.
Frequency of NSHEs
The mean self-reported NSHEs per week were 1.7 for T1DM, 0.4 for T2BOT, 0.8 for T2BB and 0.6 for T2O respondents. Annual calculated NSHE frequencies were 88.0, 18.3, 42.1 and 29.8 for T1DM, T2BOT, T2BB and T2O, respectively. The proportion of NSHE occurring at night was 26% in T1DM and 30–32% in T2DM respondents (depending on insulin treatment).
Self-reported mean annual SHE frequencies were 0.9 for T1DM, 0.3 for T2BOT, 0.3 for T2BB and 0.4 for T2O respondents.
Self-Reported Hypoglycemia Awareness and Corresponding NSHE/SHE Frequency
In T1DM respondents who had previously experienced an NSHE (i.e., at any point in the past, and not just in the study recall period), 42% reported an impaired awareness of hypoglycemia. Impaired awareness was reported by 25% of T2DM respondents (Table 2). A further 13% of T1DM and 14% of T2DM respondents were classified as unaware.
Respondents with T2DM who had impaired awareness of hypoglycemia had a significantly (p < 0.05) higher NSHE frequency than those who were aware, driven by a significant difference in T2BOT respondents. A similar trend (although not significant) was seen in T2BB and T1DM respondents.
T2DM respondents with impaired awareness reported a significantly (p < 0.05) higher SHE frequency compared with respondents who were aware, driven by the trend in T2BB respondents.
Patient–Physician Communication Regarding Hypoglycemia
Overall, 31% of T1DM and 20% of T2DM respondents rarely or never informed their general practitioner (GP)/specialist about NSHEs (Table 3). The frequency of NSHE was significantly lower in T2BOT and T2BB respondents who rarely/never inform their GP/specialist about NSHEs. An opposing trend was seen in T1DM and T2O respondents, where the frequency of NSHEs was higher in respondents who rarely/never inform their GP/specialist, although this trend was not statistically significant (Table 3).
When respondents were asked about topics discussed during GP/specialist consultations, 10% of T1DM and 13% of T2DMrespondents reported that their GP/specialist did not ask about hypoglycemia during routine appointments (Table 3).
Economic Impact of NSHEs
NSHE resulted in increased use of healthcare resources (Table 4). Over the seven days following an NSHE, blood glucose measurement (BGM) test-strip use increased by a mean of 5.0 in T1DM and 5.9 in T2DM respondents. This equates to an estimated additional resource use of €1.3/event (cost/test-strip €0.25) [22, 23]. In respondents with T1DM, 8% of daytime and 12% of nocturnal NSHE during the study period led respondents to contact a healthcare professional (HCP) (Table 4). A fifth of NSHE (20%) in respondents with T2DM resulted in contact with a HCP, regardless of the time of day that the event occurred.
Among respondents who had experienced an SHE, 30% required emergency hospital visits following their last SHE and 19% were admitted to hospital. In employed T1DM respondents (n = 185), 18% of NSHE led to lost work time with approximately 1.5 h work time lost per event. In employed T2DM respondents (n = 89), 15% of NSHE led to lost work time, with approximately 1 h’ work time lost per event (Table 4).
Patient Impact of NSHEs
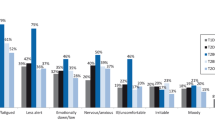
Respondents reported negative health-related impacts following their last NSHE, including feeling tired/fatigued (following 70% and 63% of NSHE in T1DM and T2DM, respectively), less alert (48% and 42% of NSHE in T1DM and T2DM) and ill/uncomfortable (39% and 47% of NSHE in T1DM and T2DM). Respondents’ emotional well-being was also affected, with NSHE resulting in feeling emotionally low (following 37% and 35% of NSHE in T1DM and T2DM, respectively), anxious/nervous (31% and 38% in T1DM and T2DM) and moody (30% and 26% in T1DM and T2DM).
Figure 1 shows the reported impact of NSHEs on daily routine for all respondents combined (i.e., T1DM and T2DM), according to if they were day or nighttime events. The specific impact of NSHEs relating to daily routine was similar, regardless of the time of day they occurred.

The patient-reported impact of daytime and nighttime non-severe hypoglycemic events in Type 1 Diabetes Mellitus and Type 2 Diabetes Mellitus patients combined. Base: All last events from respondents with at least one last event being a daytime (n = 342)/nighttime (n = 91) event in one of the waves. N/A not applicable, NSHE non-severe hypoglycemic event
These overall findings were reflected in the specific results for respondents with T1DM or T2DM. T1DM respondents reported having less energy than usual following 57% of daytime NSHE and 50% of nighttime NSHE, having a headache following 32% (daytime) and 30% (nighttime) of NSHE, and requiring daytime sleeping following 35% (daytime) and 32% (nighttime) of NSHE. T2DM respondents reported similar trends with 54% of daytime and 43% of nighttime NSHE resulting in reduced energy levels, 27% (daytime) and 24% (nighttime) of NSHE resulting in headaches, and 36% (daytime) and 30% (nighttime) of NSHE leading to daytime sleeping. Respondents also changed their behavior relating to insulin administration, reducing their normal insulin dose following 25% (T1DM) and 20% of NSHE (T2DM).
Discussion
This study identifies the real-world frequency of NSHEs and SHEs both in people with T1DM and people with insulin-treated T2DM in Spain. Furthermore, it provides an insight into the negative impact of NSHEs on patient well-being and healthcare resource use specific to Spain.
Frequency of Hypoglycemic Events
The self-reported frequencies of NSHEs and SHEs in Spain are similar to those seen in the overall European study using the same methodology, across all respondent subgroups [16]. In comparison to other previously conducted European studies, the frequency of NSHEs was similar for T1DM (1.7 in this study versus 1.8–2.2 in previous studies [9, 24, 25]), but differed for T2DM (0.4–0.8 in this study versus 0.3 in a previous study in Scotland [8]). This variation may be due to differences in the geographical region, T2DM treatment regimen, and study sample size, or how hypoglycemic events had been defined [8]. For example, the study in Scotland was substantially smaller (less than half the size of the Spanish study), with at least 70% of respondents with T2DM receiving premixed insulin (compared to fewer than 10% in this study). In addition, the definition of NSHE in the study in Scotland is narrower—all symptomatic NSHEs were recorded with a BGM, whereas this study included the detection of hypoglycemic symptoms with or without confirmation through a BGM [8].
The frequency of NSHE in T1DM respondents in this study is double the frequency of NSHE in T2DM respondents. It has been suggested that the risk of hypoglycemia in people with insulin-treated T2DM increases with longer diabetes duration, [8] and Henderson et al. [26] reported that NSHE frequency among people with T2DM only reached the same level as in people with T1DM after 10 years of insulin use in T2DM [26]. In the present study, only 32% of respondents with T2DM had received insulin for over 10 years, which may partly explain the lower frequency of NSHEs. In T2DM, the frequency of NSHE also varies according to treatment regimen, although this is expected due to the different types of insulin coverage [14].
Self-Reported Hypoglycemia Awareness and Implications for SHEs
In the present study, the authors investigated levels of hypoglycemia awareness in Spain. Reports of unawareness were similar between T1DM (13%) and T2DM (14%) respondents, although impaired awareness was higher in T1DM respondents (42% versus 25%). This is consistent with the overall European findings [16]. Consideration should be given to respondent demographics when comparing awareness levels across respondent groups. For example, the prevalence of impaired awareness is reported to increase with diabetes duration in T1DM, [9] which may confound the results of this study. Further investigation with larger sample sizes is required to fully understand the complex relationship between diabetes duration, hypoglycemia awareness and NSHE frequency.
Impaired awareness has previously been reported as the most important risk factor for severe hypoglycemia [27]. The results of this study support this finding; T2DM respondents with impaired awareness reported significantly higher SHE frequencies (p < 0.05) than respondents who were aware of their hypoglycemia. This trend, although not significant, was also seen for T1DM respondents. The statistical analysis of T2DM subgroups (T2BOT, T2BB, and T2O) may be inconclusive due to the small number of respondents with impaired awareness in each group. Further investigation with larger sample sizes is required to fully understand the trends for people receiving different insulin regimens.
Patient–Physician Communication Regarding Hypoglycemia and Corresponding NSHE Frequency
An interesting finding of this study is the higher patient–physician communication levels observed in Spain, compared to the overall European study [16]. The proportion of Spanish respondents who always/mostly inform their GP/specialist of a hypoglycemic event was nearly double that observed in the wider European study [16] (approximately 70–80% in Spain versus 35–50% in Europe). Furthermore, only a small proportion of respondents stated that their GP/specialist did not ask about hypoglycemia (10–16% in Spain, compared to 17–28% in Europe).
This study also analyzed trends in NSHE frequency according to patient communication of hypoglycemia. T2DM respondents who always/usually inform their GP/specialist about their hypoglycemia reported significantly (p < 0.05) higher NSHE frequencies than those who rarely/never inform their GP/specialist. Although causality cannot be established, these results suggest that patients who experience hypoglycemia more often are more likely to discuss their events with their physician (potentially in an attempt to improve their recognition and treatment of hypoglycemia; although this was not investigated as part of this study). Despite this, almost a third of patients surveyed in Spain expressed reluctance to discuss their hypoglycemia, which may be due to wider factors such as concerns regarding driving privileges, [12] implications for employment, or fear that they may be perceived by their general practitioner/specialist to have poor control of their diabetes. Further research is needed to understand the reasoning behind why people may not actively be reporting their hypoglycemic events.
Patient-burden and Economic Impact of NSHEs
Unsurprisingly, NSHEs were shown to have a negative effect on respondent’s physical and emotional well-being. The impact following a nighttime or a daytime NSHE was relatively similar across diabetes type. NSHE also altered a patient’s daily routine, as a quarter of T1DM and a fifth of T2DM reduced their normal insulin dose following an NSHE. This is consistent with an average of 24.9% reported in a study by Brod et al. [19] in a study of 4 countries (USA, UK, Germany and France). Respondents may have altered their correct insulin dose following an NSHE in fear of a future hypoglycemic event, an avoidance behavior shown to be a substantial obstacle to appropriate diabetes management [28–30].
Another adaptive behavior demonstrated by diabetes patients, in this study and previous studies, is an increase in self-monitoring of glucose levels. Whilst this change in diabetes self-management behavior is an appropriate adaptive response which may help prevent new events in the short-term [12], it presents a direct cost burden through increased healthcare resource use (i.e., increase in BGM test-strip consumption). This burden could be alleviated if NSHE frequency was reduced through improved awareness and recognition of events. The increase in BGM test-strip use in the week following an NSHE in this study (5.0–5.9) is comparable to that reported by Brod et al. in a study of 4 countries (5.6) [19]. The increase in BGMs following nighttime NSHEs in this study (6.5 in T1DM and 7.0 in T2DM) was similar to that reported by Spanish respondents in a study focusing on nighttime NSHE (6.8) [31]. An additional contributor to the direct cost burden of NSHEs in Spain is the resulting contact with HCPs.
Although direct costs associated with SHE are not reported in this study, the cost of an SHE to the Spanish healthcare system has previously been reported as €3,500 per event [11]. On average, 30% of respondents reported an emergency hospital visit following an SHE in this study, and 19% were admitted to hospital (16% T1, 25% T2). Considering the higher frequency of SHE reported in Spain compared to the European study, this could present a substantial burden on the Spanish healthcare system.
NSHE and SHE also present an indirect cost burden in Spain through lost work time. The percentage of NSHE reported to lead to lost work time in this study (18%) is the same as that reported by Brod et al. [19]. However, the amount of work time lost due to an NSHE was considerably lower in this study (1.5 h) compared to Brod et al. (9.9 h). This could be explained by this study encompassing NSHE which occurred outside work time, whereas Brod et al. [19] included only NSHE which occurred during working hours.
Comparison to Methodologies used in Other Publications
Methodological differences between this study and the UK Hypoglycemia Study Group study [15] relate to the recall period, patient subgroups, and the classification of hypoglycemia awareness. Patients in the UK Hypoglycemia Study recorded each hypoglycemic event as it occurred for 9–12 months [15], whereas this study used a 7-day recall period over 4 weeks. The recall period chosen for this study was supported by a previous study demonstrating that a respondent’s ability to remember NSHE during the previous week was not significantly different from the prospective recording of events over 1 week [9]. Another study has shown that people with T1DM and people with T2DM are able to accurately recall severe hypoglycemic events within a 1-year period (corresponding with the recall period in the current study) [21]. In addition to collecting self-reported data, the UK Hypoglycemia Study recorded biochemical hypoglycemia through continuous glucose monitoring with a continuous glucose monitoring system (CGMS) [15]. Patient subgroups also varied—the UK study compared the frequency of hypoglycemic events on the basis of recent or prolonged duration of insulin therapy, plus use of sulfonylureas without insulin in T2DM respondents [15]. Finally, in the UK Hypoglycemia Study, patients rated their awareness of hypoglycemia symptoms on a scale from 1 to 7 (1 = full awareness, 7 = total unawareness) [15]. This study used three categories (unaware, impaired awareness, always aware), thereby enabling identification of the gradual loss of awareness, in contrast to the Clarke [32] and Gold [33] methods which use only two categories (aware/unaware). Whilst there is no consensus on how to classify awareness, the method used in this study is the only one proven to perform similarly across language barriers [34].
Study Limitations
The limitations of the study have been reported previously, by Östenson et al. [16]. A total of 10% of respondents with T1DM in Spain reported receiving long acting insulin only. Since long acting insulin as monotherapy should only be used in T2DM, this may indicate that some respondents with T2DM had incorrectly reported their condition as T1DM. If this is the case, the proposed study may underestimate the frequency of events in T1DM, since the respondents reported as having T2DM had fewer hypoglycemic events.
There is also the potential that the study duration may over- or underestimate the annual frequency of hypoglycemia, as seasonal variation is not considered (study conducted December to May). Self-reporting and anonymity also make validation of patient data impossible, and as the response rates for waves of the study diminished (90%, 84% and 80% of respondents completed wave two, three and four, respectively), the authors cannot rule out the possibility that later waves were completed by respondents who had more experience of hypoglycemic events.
Conclusion
This study shows that NSHEs are a common occurrence across people with T1DM and T2DM in Spain. Although communication levels between respondents and GP/specialists are higher than reported across Europe as a whole, respondents experience a similar frequency of NSHEs, demonstrating a need for patient education surrounding hypoglycemia management. The importance of improving glycemic control is evidenced by the negative impact on patient well-being and healthcare resource use in Spain that result from even non-severe events.
References
International Diabetes Federation. IDF Diabetes Atlas, 6th edn. Brussels: International Diabetes Federation. 2013. http://www.idf.org/diabetesatlas. Accessed 29 Jan 2014.
Valdes S, Rojo-Martinez G, Soriguer F. Evolution of prevalence of type 2 diabetes in adult Spanish population [In Spanish]. Med Clin (Barc). 2007;129:352–5.
Soriguer F, Goday A, Bosch-Comas A, et al. Prevalence of diabetes mellitus and impaired glucose regulation in Spain: the Di@bet.es Study. Diabetologia. 2012;55:88–93.
Anarte Ortiz MT, Caballero FF, Ruiz de Adana MS, et al. Development of a new fear of hypoglycemia scale: FH-15. Psychol Assess. 2011;23:398–405.
European Medicines Agency Committee for Medical Products for Human Use (CHMP). Guidelines on clinical investigation of medical products in the treatment or prevention of diabetes mellitus. 2012. European Medicines Agency. http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2012/06/WC500129256.pdf.
American Diabetes Association Workgroup on Hypoglycemia. Defining and reporting hypoglycemia in diabetes. Diabetes Care. 2005;28:1245–9.
Davis RE, Morrissey M, Peters JR, et al. Impact of hypoglycaemia on quality of life and productivity in type 1 and type 2 diabetes. Curr Med Res Opin. 2005;21:1477–83.
Donnelly LA, Morris AD, Frier BM, et al. Frequency and predictors of hypoglycaemia in Type 1 and insulin-treated Type 2 diabetes: a population-based study. Diabet Med. 2005;22:749–55.
Pramming S, Thorsteinsson B, Bendtson I, et al. Symptomatic hypoglycaemia in 411 type 1 diabetic patients. Diabet Med. 1991;8:217–22.
Lundkvist J, Berne C, Bolinder B, et al. The economic and quality of life impact of hypoglycemia. Eur J Health Econ. 2005;6:197–202.
Brito-Sanfiel M, Diago-Cabezudo J, Calderon A. Economic impact of hypoglycemia on healthcare in Spain. Expert Rev Pharmacoecon Outcomes Res. 2010;10:649–60.
Wild D, von Maltzahn R, Brohan E, et al. A critical review of the literature on fear of hypoglycemia in diabetes: implications for diabetes management and patient education. Patient Educ Couns. 2007;68:10–5.
Leiter LA, Yale JF, Chiasson JL, et al. Assessment of the impact of fear of hypoglycemic episodes on glycemic and hypoglycemia management. Can J Diabetes. 2005;29:1–7.
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes: a patient-centred approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2012;55:1577–96.
UK Hypoglycaemia Study Group. Risk of hypoglycaemia in types 1 and 2 diabetes: effects of treatment modalities and their duration. Diabetologia. 2007;50:1140–7.
Östenson CG, Geelhoed-Duijvestijn P, Lahtela J, et al. Self-reported non-severe hypoglycaemic events in Europe. Diabet Med. 2014;31:92–101.
World ESOMAR Research. ICC/ESOMAR International Code on Market and Social Research. 2007. International Chamber of Commerce (ICC). http://www.esomar.org/uploads/public/knowledge-and-standards/codes-and-guidelines/ESOMAR_ICC-ESOMAR_Code_English.pdf. Accessed 29 Jan 2014.
European Pharmaceutical Market Research Association. Code of Conduct 2012. http://www.ephmra.org/Code-of-Conduct. Accessed 29 Jan 2014.
Brod M, Christensen T, Thomsen TL, et al. The impact of non-severe hypoglycemic events on work productivity and diabetes management. Value Health. 2011;14:665–71.
Brod M, Pohlman B, Wolden M, et al. Non-severe nocturnal hypoglycemic events: experience and impacts on patient functioning and well-being. Qual Life Res. 2013;22(5):997–1004.
Pedersen-Bjergaard U, Pramming S, Thorsteinsson B. Recall of severe hypoglycaemia and self-estimated state of awareness in type 1 diabetes. Diabetes Metab Res Rev. 2003;19:232–40.
Decision as for the competitive bidding to provide needles for prefilled pens of insulin in the Health District of Santa Cruz de Tenerife-Canary Islands-Regional Health System of Canary Islands, decision number 298. 13th of February, 2012. http://legislacion.derecho.com/anuncios-particulares-12-marzo-2012-comunidad-autonoma-de-canarias-4143938.
Decision of General Director of the Teaching Hospital of Canary Islands for the provision of test strips and lancets for the Teaching Hospital of Canary Islands. HUC-CA-022/10. 2011. http://www.gobiernodecanarias.org/boc/2011/167/008.html.
Pedersen-Bjergaard U, Pramming S, Heller SR, et al. Severe hypoglycemia in 1076 adult patients with type 1 diabetes: influence of risk markers and selection. Diabetes Metab Res Rev. 2004;20:479–86.
Kristensen PL, Hansen LS, Jespersen MJ, et al. Insulin analogues and severe hypoglycaemia in type 1 diabetes. Diabetes Res Clin Pract. 2012;96:17–23.
Henderson JN, Allen KV, Deary IJ. Hypoglycaemia in insulin-treated Type 2 diabetes: frequency, symptoms and impaired awareness. Diabet Med. 2003;20:1016–21.
Akram K, Pedersen-Bjergaard U, Carstensen B, et al. Frequency and risk factors of severe hypoglycaemia in insulin-treated Type 2 diabetes: a cross-sectional survey. Diabet Med. 2006;23:750–6.
Vexiau P, Mavros P, Krishnarajah G, et al. Hypoglycaemia in patients with type 2 diabetes treated with a combination of metformin and sulphonylurea therapy in France. Diabetes Obes Metab. 2008;10(Suppl 1):16–24.
Frier BM. How hypoglycaemia can affect the life of a person with diabetes. Diabetes Metab Res Rev. 2008;24:87–92.
Cryer PE. The limiting factor in the glycaemic management of type I and type II diabetes. Diabetologia. 2002;45:937–48.
Brod M, Wolden M, Christensen T, et al. A nine country study of the burden of non-severe nocturnal hypoglycaemic events on diabetes management and daily function. Diabetes Obes Metab. 2013;15:546–57.
Clarke WL, Cox DJ, Gonder-Frederick LA, et al. Reduced awareness of hypoglycemia in adults with IDDM. A prospective study of hypoglycemic frequency and associated symptoms. Diabetes Care. 1995;18:517–22.
Gold AE, MacLeod KM, Frier BM. Frequency of severe hypoglycemia in patients with type I diabetes with impaired awareness of hypoglycemia. Diabetes Care. 1994;17:697–703.
Hoi-Hansen T, Pedersen-Bjergaard U, Thorsteinsson B. Classification of hypoglycemia awareness in people with type 1 diabetes in clinical practice. J Diabetes Complicat. 2010;24:392–7.
Acknowledgments
Editorial support was provided by Ben Rousseau, Sophie Laurenson and Elizabeth Canty of Adelphi Values and funded by Novo Nordisk, Madrid, Spain. Sponsorship for this study and article processing charges were funded by Novo Nordisk, Madrid, Spain. All named authors had full access to all of the data in this study, meet the ICMJE criteria for authorship for this manuscript, take complete responsibility for the integrity of the data and accuracy of the data analysis and have given final approval for the version to be published.
Conflict of interest
D. Orozco-Beltrán has received honoraria for consulting Novo Nordisk, Lilly, Astra-Zeneca, Esteve, Chiesi, MSD and Sanofi. P. Mezquita-Raya received honoraria for clinically advising, Lilly, Roche, Sanofi, Novo Nordisk, Amgen, MSD, Pfizer, Boerinhger, Tolerx. Consultor/Ponente: Lilly, Almirall, Novartis, Novo Nordisk, Astra-Zeneca, BMS, Esteve, MSD, Sanofi and Fes. M. Galán and A. Ramírez de Arellano are currently employed by Novo Nordisk.
Compliance with ethics
This was a non-interventional market research study. Questionnaires were completed anonymously in accordance with the regulations and practice of market research governing bodies: European Society for Opinion and Marketing Research (ESOMAR) and European Pharmaceutical Market Research Association (EphMRA). The EphMRA Code of Conduct states that Market Research does not require Clinical Research Ethics Committee or Independent Review Board approval.
This article does not contain any new studies with human or animal subjects performed by any of the authors.
Informed consent was obtained from all patients for being included in the study.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Orozco-Beltrán, D., Mezquita-Raya, P., Ramírez de Arellano, A. et al. Self-Reported Frequency and Impact of Hypoglycemic Events in Spain. Diabetes Ther 5, 155–168 (2014). https://doi.org/10.1007/s13300-014-0057-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-014-0057-z