Article Text

Abstract
Background To satisfy the increasing demand of mechanical thrombectomy (MT) for acute ischemic stroke treatment, new organizational concepts for patient care are required. This study evaluates time intervals of acute stroke management in two stroke care models, including one based on transportation of the interventionalist from a comprehensive stroke center (CSC) to treat patients in two primary stroke centers (PSC). We hypothesized that time intervals were not inferior for the ‘drip-and-drive’ concept compared with the traditional ‘drip-and-ship’ concept.
Methods Patients treated with MT at the PSC (‘drip-and-drive’, ‘D+D group’) were compared with patients transferred from PSC to CSC for MT (‘drip-and-ship’, ‘D+S group’) with regard to time delays. Time intervals assessed were: symptom onset to initial CT, to angiography, and to recanalization; time from initial CT to telephone call activation, to arrival, and to angiography; and time from telephone call activation to arrival and from arrival to angiography.
Results 42 patients were treated at the PSC after transfer of the interventionalist, and 32 patients were transferred to the CSC for MT. The groups did not differ with regard to median Onset–CT and CT–Phone times. Significant differences between the groups were found for the primary outcome measure CT–Arrival time (‘D+D group’: median 121 (IQR 108–134) min vs 181 (157–219) min for the ‘D+S group’; P<0.001). Time difference between the groups increased to more than 2 hours for median CT–Angio times (median 123 (IQR 93–147) min vs 252 (228–275) min; P<0.001).
Conclusion Time intervals for the ‘D+D group’ were not inferior to those of the ‘D+S group’. Moreover, under certain conditions, the ‘drip-and-drive’ concept might even be superior.
- thrombectomy
- stroke
- political
Statistics from Altmetric.com
Introduction
The publication of major positive randomized trials revealing a significant treatment effect of endovascular recanalization on patient outcome in acute ischemic stroke due to large vessel occlusion1–5 had a strong impact on stroke management and immediately resulted in new recommendations for acute stroke treatment.6 7 In Germany, as in many other countries, nationwide stroke units are established even in small and regional hospitals capable of performing acute cranial CT (CCT) and of starting intravenous tissue plasminogen activator immediately, whereas mechanical thrombectomy (MT) is mainly performed at centers with interventional neuroradiologists (INRs), ideally providing 24/7 coverage. Such service requires a certain annual caseload in MT and other intracranial procedures for maintaining skills levels and for justifying the resources, including on-call-services. Accordingly, centralization of stroke care towards comprehensive stroke centers (CSC) has been suggested. However, such re-structuring faces considerable practical, political, budgetary, and psychological challenges, in particular in federal countries such as Germany.
To ensure MT for patients in stroke centers without an INR service, the patient might be transferred to a CSC (‘drip-and-ship’) or the INR might be transferred to the patient at the primary stroke center (PSC). Whereas ‘drip-and-ship’ is already practiced by existing co-operations, such as neurovascular networks,8 no experience with the relatively new ‘drip-and-drive’ concept has been reported to date.
We present our first year experience with the latter concept. We used time intervals as practical and sensitive performance indicators, and hypothesized that the time intervals may not be significantly inferior for the ‘drip-and-drive’ concept compared with the ‘drip-and-ship’ concept.
Methods
To provide acute endovascular stroke treatment to the population of two PSCs (hospital A and B) with catchment areas of 180 000 and 200 000 citizens (treating 850–1130 acute ischemic stroke patients each per year), a formal collaboration with our university hospital based CSC was established, including joint processes and matched interventional equipment. As a precondition, technicians and radiologists of the PSCs were introduced to MT procedures and the material used at the CSC, including hands-on courses. INRs from the CSC visited the PSCs to become familiar with the local teams of neurology, radiology, and anesthesiology, as well as with the location and functioning of angiography suites and stroke units. Driving distance between the CSC and the two PSCs is 53 km (hospital A) and 63 km (hospital B). At least seven INRs work at the CSC of whom at least four provide the on-call service at the CSC and a further three INRs cover the on-call service for MT performed at the PSCs.
Work flow at the PSC
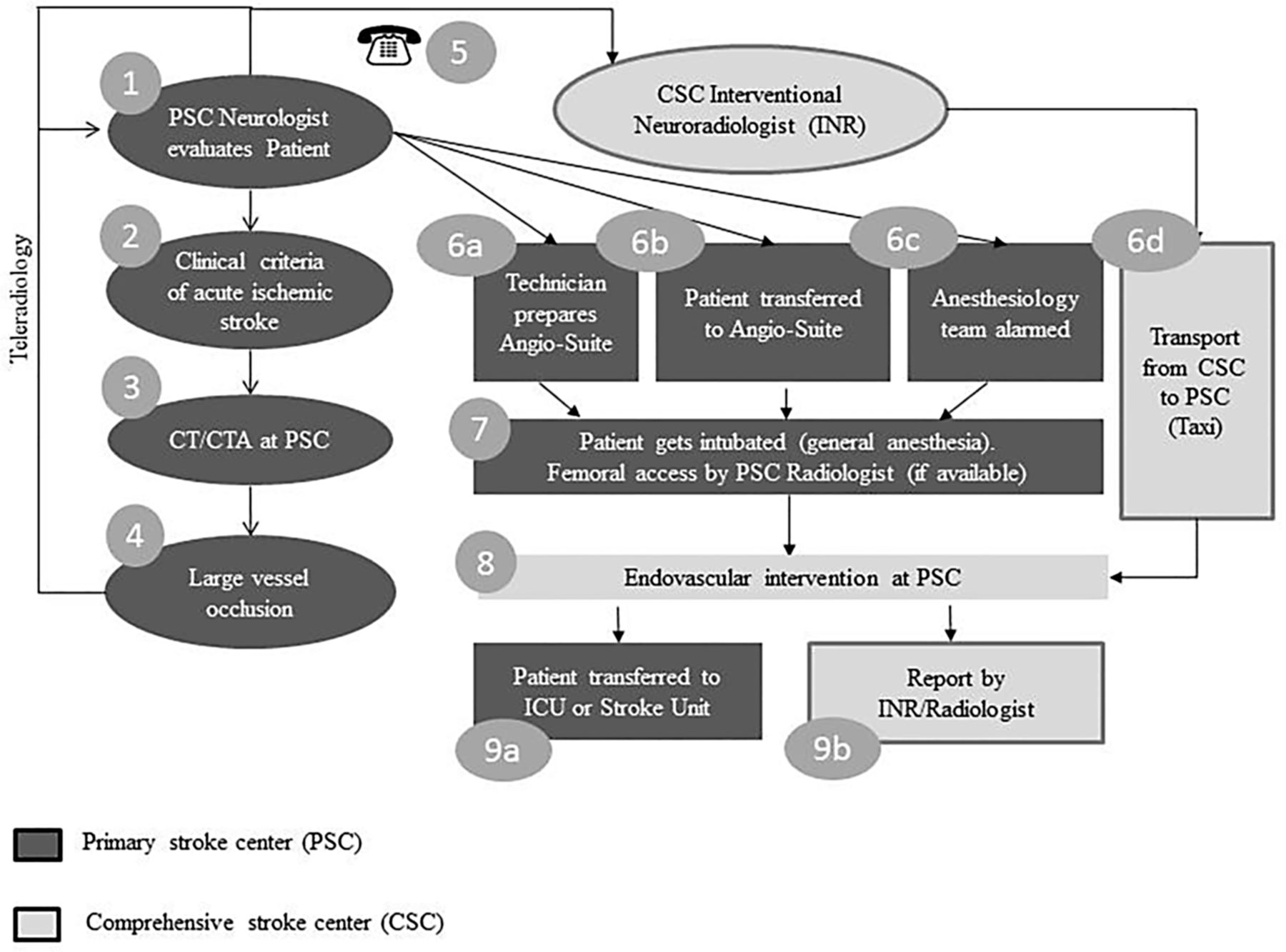
After admission to the PSC, patients were diagnosed by the neurologist on call. CCT and CT angiography (CTA) were performed to rule out hemorrhage and to evaluate vessel occlusion status. In the case of large vessel occlusion, the INR at the CSC was informed by a dedicated mobile phone and evaluated CCT and CTA images transferred by telemedicine. When endovascular treatment was indicated, the INR immediately set off to the PSC by taxi, while at the PSC, the patient was transferred to the local angiography suite and prepared for the intervention, including general anesthesia (figure 1). If available, an experienced member of the local radiology team already started the procedure by placing a catheter sheath and guiding catheter.
When the INR arrived, the intracranial intervention was performed. In the case of a local radiologist not being available, the whole procedure was performed by the arriving INR. Because this concept includes close collaboration of the INR with the local angiography team, it was restricted to working hours initially. Patients treated with this ‘drip-and-drive’ approach were labeled the ‘D+D group’. Patients admitted at night-time or during weekends were transferred to the CSC by helicopter or emergency ambulance if MT was considered necessary (classical ‘drip-and-ship’, ‘D+S group’). In either case, an emergency physician escorted the patient. Due to continuous expansion of the capacities (eg, availability of technicians or anesthesiology teams) at the PSCs, the ‘drip-and-drive’ concept was expanded into non-working hours. Overall, patients were treated at the PSC whenever possible (ie, available angiography suite, technicians, and anesthesiologists at the PSC). Non-working hours were defined as weekends, holidays, and 4pm to 8am on week days.

Work flow of the ‘drip-and-drive’ approach for acute ischemic stroke patients admitted to the primary stroke center (PSC). After telephone call activation by the PSC neurologist, the interventional neuroradiologist (INR) has access to CT and CT angiography (CTA) images via teleradiology, and confirms the indication for mechanical thrombectomy (step 5). During transfer of the INR from the comprehensive stroke center (CSC) to the PSC, processes at the PSC are run in parallel (step 6).
Work flow at CSC
After arrival at the CSC, the patient was briefly re-evaluated by the stroke neurologist. In the case of unchanged or worsened symptoms, a native CCT was performed to exclude hemorrhage or already demarcated large infarcts. In the case of resolving symptoms, CCT and CTA were performed, and MT initiated if large vessel occlusion persisted. Those patients still qualifying for MT were brought to the already prepared angiography suite, and interventions were performed with local anesthesia whenever possible. Otherwise, general anesthesia was initiated.
Endovascular intervention
During interventions, no heparin bolus was administered. Standard techniques includes an 8 F femoral access and 8 F guide catheter/balloon catheter for the carotid artery and 6 F guide catheter for vertebral arteries. For MT, stentrievers (Solitaire FR revascularization device; Covidien, Mansfield, Massachusetts, USA) were applied at the PSC. At the CSC, other flow restoration devices such as the Trevo ProVue Stentriever (Stryker, Kalamazoo, Michigan, USA) and ERIC retrieval device (Microvention, Tustin, California, USA) could be employed as well as the Solitaire stentriever. Intermediate catheters (ie, 5 F and 6 F Sofia; Microvention) and aspiration were employed at the discretion of the INR. After MT, patients were monitored at the ICU for at least 24 hours with follow-up CT the next day. Patients who were in a very good condition after MT were alternatively transferred directly to the stroke unit.
Time intervals and data analysis
All consecutive patients admitted to hospital A or B with acute ischemic stroke due to large vessel occlusion who were intended to be treated with MT either at a PSC or CSC were included in this analysis. The following time variables were prospectively recorded: stroke symptom onset, time of admittance to the PSC, initial CT at the PSC, telephone call from the PSC to the CSC with the decision to perform MT, arrival of the INR at the PSC angiography suite, arrival of the patient at the emergency room of the CSC, second CT at the CSC, first angiography run, and time of recanalization.
Time interval from initial CT to arrival of the INR at the angiography suite of the PSC or of the patient at the emergency room of the CSC (CT–Arrival) was defined as the primary outcome measure. Secondary outcome measures were telephone call activation of the INR to arrival either of the INR at the PSC or of the patient at the CSC (transportation time), time from symptom onset to either CT (Onset–CT), first angiography run (Onset–Angio), or recanalization. Additionally, time from initial CT to telephone call activation (CT–Phone), from initial CT to first angiography run (CT–Angio), as well as from patient arrival at the CSC to the second CT (Door–CT) and first angiography run (Door–Angio) were assessed. Patient characteristics and recanalization success according to the Thrombolysis in Cerebral Infarction (TICI) scale9 were compared between groups. TICI grades 2b and 3 were regarded as successful recanalization.
Consecutive data collection was approved by the local ethics committee. Due to the retrospective character of the analysis of anonymized data, no written informed consent of the patients was required. Statistical analysis was performed with IBM SPSS statistics V.21.0. Groups A and B were compared with regard to different time intervals, patient demographics, presenting stroke severity, and recanalization results. For time intervals, age, National Institutes of Health Stroke Scale (NIHSS), and TICI scores, non-parametric tests were applied (Mann–Whitney U). For categorical variables, Pearson’s χ2test was performed. Probability values of P<0.05 were considered significant.
Results
A total of 74 patients were included (median age 76 (IQR 67–83) years). Median NIHSS score on admission at the PSC was 15 (IQR 11–18) and 38 were men. Forty-two patients were treated at a PSC (‘D+D group’) and 32 patients were transferred to the CSC (‘D+S group’). The groups did not differ significantly regarding the occluded artery, initial NIHSS score, age, sex, or recanalization success (table 1). Treatment during non-working hours occurred in 33% of patients in the ‘D+D group’ compared with 87% of patients in the ‘D+S group’. Intravenous tissue plasminogen activator was administered to 30/42 patients in the ‘D+D group’ (71%) and to 22/32 patients in the ‘D+S group’ (69%). MT was performed in 37 patients in the ‘D+D group’ and in 23 patients in the ‘D+S group’, resulting in successful recanalization in 30/37 (81%) and in 16/22 (73%) cases, respectively.
The rate of general anesthesia was 98% in the ‘D+D group’ compared with 35% in the ‘D+S group’. Reasons not to perform MT in the ‘D+D group’ were large infarction revealed by follow-up CT before angiography in one patient, recanalization diagnosed at angiography before MT in two patients, and failed access to the intracranial vessels during angiography in two further patients. In the ‘D+S group’, follow-up CT/CTA or MRI/MR angiography at the CSC after patient transfer revealed recanalization in three patients and increased infarct size in another six patients, obviating angiography and MT. In the ‘D+S group’, 12 patients were transported by helicopter and 20 by emergency ambulance.
Demographic data and patient characteristics
The primary outcome measure, CT–Arrival time, differed significantly between the groups. Median time for INR transfer in the ‘D+D group’ was 1 hour less compared with the median time for patient transfer in ‘D+S group’ (121 (IQR 108–134) min vs 181 (157–219) min, P<0.001).
Median time intervals from symptom onset to initial CT were similar in both groups (‘D+D group’: 88 min (IQR 59–124) vs ‘D+S group’: 84 (IQR 67–100) min) as well as from CT to phone call activation (CT–Phone; 37 (24–54) min vs 40 (29–54)min, respectively).
All remaining time intervals between symptom onset, phone call activation, and initial CT on the one hand, and arrival, angiography, and recanalization on the other, were significantly shorter in the ‘D+D group’ compared with the ‘D+S group’ (table 2). Median door to angiography time at the CSC for the 23 patients receiving MT in the ‘D+S group’ was 86 min (IQR 65–104).
Comparison of time intervals between the ‘drip-and-drive’ concept and the classical ‘drip-and-ship’ concept
Discussion
The publication of five randomized trials1–5 all showing a significant treatment effect of MT on patient outcome compared with standard care, including intravenous tissue plasminogen activator administration in acute ischemic stroke patients suffering large vessel occlusion of the anterior circulation, had a large impact on stroke treatment policy.6 7 To provide widespread access to state of the art MT for the whole population, several concepts were discussed. This study assessed time delays of a new treatment concept that includes transport of the INR from the CSC to the PSC (‘drip-and-drive’) to perform MT.
The main finding of our study was that transfer time of the INR from the CSC to the PSC (‘D+D group’) was significantly shorter than transportation of the patient from the PSC to the CSC (ie, classical ‘drip-and-ship’ model (‘D+S group’). This result is all the more astonishing as transportation of the INR was by taxi service whereas patients were transported by helicopter or emergency ambulance. While transportation times between the two groups differed by 1 hour, time differences between the groups increased to more than 2 hours for CT–Angio (time from initial CT to first angiography run).
How can the time discrepancies between the two groups in our study be explained? Transfer times in the ‘D+D group’ by taxi were consistently between 60 and 90 min, depending on traffic. After phone call activation, the INR immediately called a taxi with the start of transportation 5–10 min later. This transportation time might be further reduced if the INR could be transported by emergency ambulance, another vehicle with special license, or by helicopter.
Time delays with the ‘drip-and-ship’ concept due to patient transportation, interfacility communication, and re-evaluation are well known.10 11 According to our experience, organization of patient transport is often time consuming as different services have to be coordinated and helicopter service availability depends on weather conditions. In rural areas, the emergency ambulance is sometimes not allowed to leave the county district (ie, due to lack of resources or because of other emergencies). Therefore a ‘mobile’ emergency ambulance has to be ordered that often arrives from the city of Hamburg or even from other towns of Lower Saxony. The handover of the patient at the PSC to the transport service often takes approximately 20 min.
After arrival at the emergency rooms of the CSC, the patient will be evaluated again clinically and by CT, and then transported to the angiography suite. The time interval from arrival at the emergency room of the CSC to the first angiographic run exceeded 1 hour in our patients, which is comparable with times reported for busy neurovascular centers.12 13 This relatively long work flow at the CSC might be related to the treatment of the ‘drip-and-ship’ patients during non-working hours. Whereas the steps ‘transportation’, ‘re-evaluation’, and ‘angiography preparation’ are performed sequentially in ‘D+S group’ patients, they are paralleled in the ‘D+D group’, resulting in comparable CT–Arrival and CT–Angio times for the ‘D+D group’ patients.
During INR transfer from the CSC to the PSC, patient work up at the PSC progresses. The patient is transported to the angiography suite, and is intubated and prepared for the intervention. In a best case scenario, local members of the radiology department start the intervention by placing the catheter sheath or even the guide catheter in the cervical arteries. As a result, intracranial recanalization is started immediately after arrival of the INR at the PSC, saving another hour that is lost due to work flow at the CSC (figure 2). Consequently most of ‘D+D group’ patients had already been recanalized at the PSC before MT at the CSC was started for the ‘D+S group’ patients.

{kind=link}
{kind=link}
Comparison of patients treated by ‘drip-and-drive’ (‘D+D group’, white boxes) with those treated by ‘drip-and-ship’ (‘D+S group’, gray boxes). No significant difference was found for the time from symptom onset to initial CT. The remaining time intervals were significantly different (CT–Arrival and CT–Angio, P<0.001; Onset–Recanalization, P=0.001). Note the increase in time difference between the groups after arrival. Onset–CT, symptom onset to CT at the primary stroke center (PSC). CT–Arrival, CT at the PSC to arrival of the interventional neuroradiologist at the PSC (‘D+D group’) or of the patient at the comprehensive stroke center (‘D+S group’). Onset–CT, symptom onset to CT at the PSC. CT–Angio, CT to first angiographic run. Onset–Recanalization, symptom onset to recanalization.
Time intervals and delays in acute ischemic stroke treatment have been subject to several studies in the past. Onset–CT times of both groups were in the reported range of 79–90 min.14 15 For ‘drip-and-ship’ patients, Onset–Angio times of 233–300 min were reported.12 14 16 Onset–Angio times of ‘D+S group’ patients in our study were even longer. The shortest reported time of 233 min was achieved in a well established stroke network in a densely populated area of Germany,14 whereas the PSCs of our study are located in less densely populated areas, explaining the longer transportation times to some extent. For example, an additional time loss of approximately 45 min was found for patients transferred from regional hospitals (distance to CSC >42 km) compared with patients transferred from local hospitals (distance to CSC <42 km).10 Driving distance from the CSC to both PSCs in our study was >42 km.
Transportation time of the ‘D+D group’ was shorter, and that of the ‘D+S group’ was longer than the 104 min reported in the study of Prabhakaran,11 whereas CT–Phone times in both groups were shorter than that reported by Sun et al 15 (47 min). However, Onset–Angio and CT–Angio times in the ‘D+D group’ (201 min and 123 min, respectively) were shorter than the fastest reported times (233 min and 139 min, respectively).14 This demonstrates the feasibility of the ‘drip-and-drive’ concept with regard to time delays.
We are not able to provide standard clinical outcome measures, such as modified Rankin Scale scores after 90 days, in a sufficient number of our patients. However, several studies have shown the strong effect of a shorter time to treatment on both the rates of good outcome and the therapy effect in acute ischemic stroke patients for intravenous tissue plasminogen activator as well as for MT.17–19 For example, in the SWIFT Prime study, the probability of a good outcome (modified Rankin Scale score 0–2) was 91% if recanalization by MT was achieved in the first 2.5 hours after symptom onset and decreased to 30% at 6 hours.20 Given these numbers, a time delay of 2 hours means an absolute reduction of 20–40% for a good outcome.
A study assessing Alberta Stroke Program Early CT scores (ASPECTS) before and after patient transfer revealed a significant decline from a median score of 8 to 7 in 106 patients, whereas median time elapsed between both imaging procedures was 2.7 hours.16 The decline in ASPECTS resembles potential infarct growth that might result in exclusion of the patient from further endovascular treatment. In our study, six patients in the ‘D+S group’ (19%) in whom time elapsed between CT at the PSC and at the CSC was approximately >3 hours were excluded from MT because of infarct growth. However, as salvageable tissue can persist far beyond 6 hours from symptom onset,21 22 repeated stroke imaging, even beyond 6 hours of stroke onset, should be performed with careful evaluation not to miss those candidates for MT.
There may be many instances to improve patient management and transportation to shorten time delays, especially for the ‘drip-and-ship’ model. However, reasons for the unsatisfactory situation reflected by the findings of our study are manifold, and might be found in the federally organized health system of Germany, the high economic cost pressure on hospitals, and difficulties in recruiting enough qualified personnel in rural areas.
Concerns may exist regarding the quality of endovascular treatment at a PSC (eg, decreased quality due to low caseload, less experienced personnel, and limited stocks of endovascular material). We tried to overcome these constraints with special training for all of the personnel and standardized materials. Moreover, the caseload of the PSCs in our study conformed to medium volume centers, performing 8–35 MTs per year. For such medium volume centers no difference in mortality rates compared with high volume centers performing >35 MTs per year was found.23
The results of our study are not applicable to every county hospital that serves as a PSC, because local stroke organization, traffic conditions, and transportation systems may be significantly different. However, our study confirms the feasibility of the ‘drip-and-drive’ concept. In particular, the short transfer time that results in shorter times from symptom onset to recanalization is a strong predictor of better patient outcome. Notably, the number of our patients was not powered to compare clinical outcomes between the groups.
Limitations
Anesthesia conditions differed between the groups. However, this may have influenced patient outcome, which is beyond the scope of this study. If ‘D+S group’ patients were treated under general anesthesia instead of under local anesthesia, time to treatment would have been prolonged and the study results would not have changed. Groups were biased with regard to treatment hours (table 1). ‘D+D group’ patients were more likely treated during working hours whereas ‘D+S group’ patients were more likely treated during night-time hours or at weekends. Acute management times at the PSC did not differ between the groups (Onset–CT and CT–Phone). Transportation time of the INR by taxi (‘D+D group’) should be shorter at night and at weekends due to better traffic conditions. On the other hand, transportation time of ‘D+S group’ patients might have been shorter due to better transport capacities during working hours.
Conclusion
Transfer of the INR to perform MT in collaboration with local teams at the PSC is feasible (‘drip-and-drive’) and may result in significant reduction of process time compared with the established ‘drip-and-ship’ approach. Prospective comparison of clinical outcomes with the different approaches is required to definitely evaluate the ‘drip and drive’ approach.
References
Footnotes
Contributors CB, HS, HH, and JF made substantial contributions to the conception and design of the work. Data acquisition was performed by CB, EG, CK, JT, and FF. CB and FF performed the data analysis. Interpretation of the data was done by CB, EG, HS, HH, GT, and JF. CB and JF drafted the manuscript and all of the other authors revised it critically for important intellectual content. All authors approved the final version to be published. They agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the manuscript are appropriately investigated and resolved.
Competing interests None declared.
Ethics approval The study was approved by the ethics committee of the Medical Association of the City of Hamburg.
Provenance and peer review Not commissioned; externally peer reviewed.