Article Text

Abstract
Background: NICE guidelines for the management of head injury were published in June 2003. Their recommendations differ markedly from previous guidelines published by the Royal College of Surgeons (RCS). In place of skull radiography and admission, computed tomography (CT) is advocated. The impact of these guidelines on service provision in the UK is unknown.
Methods: Data on all clinical correlates of children presenting with any severity of head injury was collected in three hospitals in the northwest of England. The current skull radiograph (SXR), CT scan, and admission rates were determined. The rates of SXR, CT scan, and admission that should have occurred when following either the RCS or NICE guidelines were then determined.
Results: Data from 10 965 patients who attended three hospitals between February 2000 and August 2002 was studied. Twenty five per cent of patients received a SXR, 0.9% a CT scan, and 3.7% were admitted. Strict adherence to the RCS guidelines would have resulted in a 50% SXR rate, a 1.6% CT scan rate, and a 7.1% admission rate. Adherence to NICE guidelines would result in a 0.3% SXR rate, an 8.7% CT scan rate, and a 1.4% admission rate, although the CT rate would drop to 6.3% if vomiting three or more times in the under 12s was used instead of more than one vomit.
Conclusions: The new NICE guidelines do not increase the workload caused by patients attending with head injury but they move their management from the observation ward to the radiology department.
- CT, computed tomography
- GCS, Glasgow Coma Score
- NICE, National Institute of Clinical Excellence
- RCS, Royal College of Surgeons
- SXR, skull radiograph
- craniocerebral trauma
- brain injuries
- tomography
- x-ray computed
- guidelines
Statistics from Altmetric.com
- CT, computed tomography
- GCS, Glasgow Coma Score
- NICE, National Institute of Clinical Excellence
- RCS, Royal College of Surgeons
- SXR, skull radiograph
One million patients with head injuries attend emergency departments each year in the UK, of which up to 50% are children.1–,3 In contrast to the high incidence of head injury, the mortality rate is comparatively low (6–10 per 100 000), and as few as 0.2% of all people attending the emergency department suffer a fatal outcome.4,5
Thus although emergency clinicians see a large number of patients with minor head injury, they rarely see patients who then suffer life threatening intracranial complications. Therefore they must rely on clinical guidelines to govern the management of these patients.
Over the past decade a number of decision rules have been developed in order to identify high risk patients in the minor head injury category who require a CT scan.6–,11 UK practice has consistently been centred on guidelines based on high rates of skull radiography and admission, and low rates of computed tomography (CT). The most recent, widely adopted version of these guidelines was published in June 1999 by the Royal College of Surgeons of England.12
The National Institute of Clinical Excellence (NICE) has recently published a markedly different protocol for the management of head injuries in adults and children for widespread use in the UK.13 Based on the Canadian Head CT rule,6 these guidelines advocate a management strategy based on early computed tomography for high risk patients and a marked reduction in skull radiography and admission.
The implication of these guidelines on UK hospital resources in terms of increased CT requests and possibly lower admission rates are currently unknown. A comprehensive database of 11 000 consecutive children presenting with a head injury was therefore analysed to investigate the impact of these new guidelines.
METHODS
Study type
This was a subanalysis of a larger multicentre prospective cohort study currently underway in the northwest of England.
Patient selection
A prospective cohort study of all children presenting to 10 hospitals in the northwest of England with any severity of head injury, was conducted between February 2000 and August 2002. This study analysed all patients in this database who attended Alder Hey Hospital, Stepping Hill Hospital, or Manchester Royal Infirmary, during this time period.
Inclusion criteria
All patients under 16 years of age were included. Any patient presenting to the emergency department with a head injury of any severity was included in the study. Of note, there was no necessity for loss of consciousness or amnesia for inclusion into our study. There were no exclusion criteria other than refusal to enter the study by the patient or guardian.
Data collection
A specifically designed proforma was created for data collection. This proforma collected data on over 40 clinical correlates pertaining to the head injury, including correlates on the mechanism of injury, symptoms, signs, and management of the patient. Every physician who participated in the study was given a one hour training session on the study and the use of this proforma for data collection. Response rates and quality of completion was monitored in all centres on a monthly basis in order to ensure high compliance. Importantly, all physicians were asked to follow the 1999 Royal College of Surgeons guidelines for the management of head injuries; the guidelines were printed clearly on the front of every proforma.
Outcome measures
Three outcome measurements were analysed, skull radiograph (SXR), head CT, and need for admission. The actual management of the patient was taken from proforma documentation. Any proforma documenting a SXR, admission or CT scan, or with data missing from any of these categories, had this data verified by consulting hospital records. Some management decisions depend on the presence of a skull fracture. All SXRs were checked by radiologists and diagnosis of a fracture was determined only by the radiologist’s report.
Management of these patients according to the Royal College of Surgeons guidelines and the NICE guidelines were determined for each individual patient in the study and this was compared to actual management.
Statistical analysis
Descriptive analysis was conducted using SPSS version 11.5. In order to provide clinicians with an estimate of the variability in the frequency that investigations might be required on a weekly basis, confidence intervals for a theoretical group of 100 patients attending the emergency department with head injury were constructed using a Monte-Carlo simulation.14 One hundred patients were randomly selected from our dataset and the number of investigations required was calculated. Their data were replaced and the process was repeated 1000 times. The 95% confidence intervals of this dataset are presented. The simulation was performed using STATA version 7.
Ethics
Multicentre ethical approval was obtained for this study and consent to participate in this study obtained from all patients or guardians prior to entry to the study.
RESULTS
A total of 10 965 patients entered this study from Alder Hey, Stepping Hill, and Manchester Royal Infirmary. Table 1⇓ shows their demographics.
Patient demographics
Of the 10 965 patients, attending physicians requested 2746 skull radiographs (25%). Only 94 CT scans were requested (0.9%) and 409 patients were admitted (3.7%). Another 511 patients were observed in the emergency department for over three hours (4.7%), although 477 of these patients went home within six hours.
When the Royal College of Surgeons guidelines were strictly applied to the database it was found that these guidelines dictate that 5519 (50.3%) of patients should have had a SXR. Figure 1⇓ shows the reasons for a SXR request by these guidelines. It can be seen that the majority of SXRs were required by RCS guidelines due to the presence of any bruising or swelling. It is clear that physicians are not using the presence of any bruise or swelling to request a SXR as the actual number of SXRs requested is far fewer than that predicted. The figure for SXRs required by the RCS guidelines was recalculated for an increasing size of bruise or swelling. If a bruise or swelling over 4 cm was used instead of any bruise or swelling, 3122 (28%) of patients would have required a SXR. So it seems that physicians may be regarding bruise or swellings only over 4 cm as significant.

SXR required by RCS guidelines 1999.
Applying RCS guidelines to the dataset, 171 CT scans would have been required (1.6%), most of these being due to a skull fracture being found on SXR. Full application of the RCS guidelines would have required 775 admissions (7.1%).
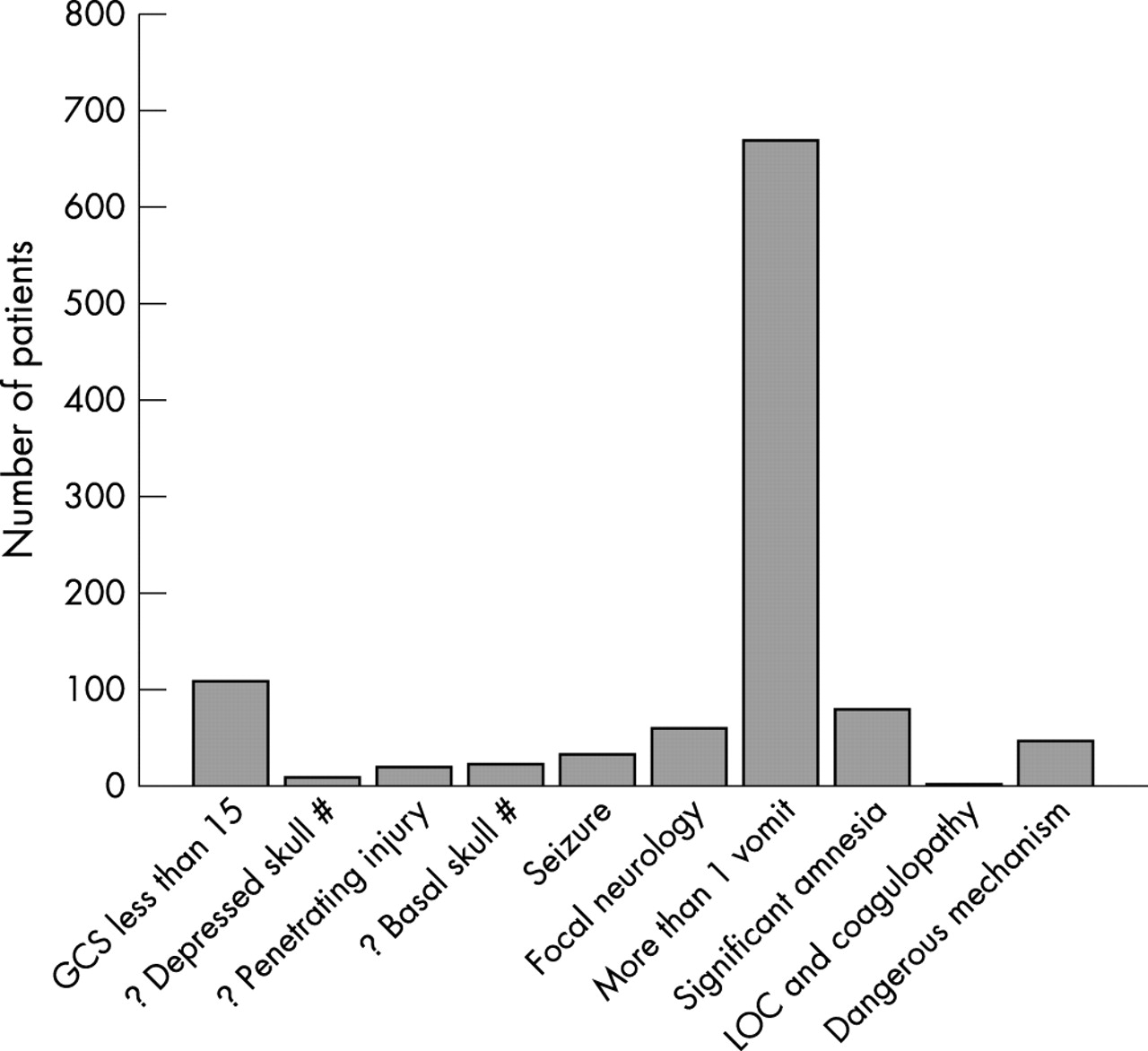
The NICE guidelines were applied to the dataset (full results are given in table 2⇓ and NICE guidelines for a CT are given in table 3⇓). There are very few reasons for requesting a SXR under the NICE guidelines and we found that only 30 SXRs should have been performed due to suspicion of non-accidental injury. Following exactly the recommendations for a CT scan by NICE it was found that 957 (8.7%) CT scans would have to have been required in our dataset. Figure 2⇓ gives the reasons for requiring a CT scan. It was found that by far the most common reason for requesting a CT scan was the presence of more than one vomit. There is a caveat in the NICE guidelines for vomiting in the under 12s, allowing clinicians to use their clinical judgement as to whether more than one vomit is a sufficient reason to request a CT scan. We therefore recalculated these figures for our database using three or more vomits as the number of vomits required to request a CT scan in the under 12s. The number of CT scans now required by NICE dropped to 687 (6.3%).
Management of 10 965 patients with head injury.
NICE guidelines for CT scanning of high risk patients

{kind=link}
{kind=link}
Reasons for a CT under NICE guidelines. #, fracture; ?, query.
The number of admissions required under NICE guidelines was calculated to be 151 (1.4%), of which 107 were due to an admission GCS score of less than 15. These patients would be eligible for discharge on returning to GCS 15 under NICE guidelines, after a CT scan.
Our database contains only information on children and adolescents. In order to gain an insight as to the possible impact that the NICE guidelines would have on an adult population, we analysed only those patients between 12 and 16 years of age. Table 4⇓ presents the full results; it was found that the rates of investigation and management are similar to the full database, although the CT scan rate as determined by NICE was a little higher at 10.7%. It can be seen by the current management rates of admission and SXR that the adolescents perhaps contain fewer trivial injuries, which may account for the higher predicted CT scan rate.
Management of patients 12–16 years of age (n = 1561)
There has been some concern that the new NICE head injury guidelines identify a higher proportion of patients at high risk compared to the Royal College of Surgeons guidelines. We therefore looked at the number of patients that each guideline assigned as high risk. A high risk patient was defined as any patient that qualified for either a CT scan or an admission. The Royal College of Surgeons guidelines allocated 787 patients as high risk (7.2%), whereas the NICE guidelines allocated 983 patients (8.9%). However, if the higher threshold of vomiting was used for the NICE guidelines in patients under 12, only 714 patients would have been allocated as high risk (6.5%). Therefore NICE guidelines do not allocate a higher proportion of patients as high risk compared to RCS guidelines.
In order to provide clinicians with an estimate of the upper limits of investigation that might be required in their department, we modelled a theoretical cohort of 100 patients and calculated the 95% confidence intervals for each management option. Table 5⇓ presents the full results. It was found that the upper limit of the number of CT scans that might be required for a group of 100 patients attending the emergency department using the NICE guidelines was 11.1%.
95% CI for rates of imaging or management that might be expected for 100 patients attending the emergency department with a head injury (modelled by Monte-Carlo simulation)
DISCUSSION
NICE guidelines aim to unify clinical practice in the UK for the management of head injuries around a single, best evidence guideline. However, in order to implement these practice parameters, clinicians must not only have confidence in the methodology and research background of the guidelines, but also an understanding as to the likely impact on service provision. NICE guidelines have been produced to the highest methodological standards, but were unable to provide an accurate indication of the likely impact that these guidelines would have in terms of rates of imaging and admission. We have shown that admission rates are currently 3.7% of all head injury attendances and that this rate is likely to drop to 1.4% with full application of the guidelines. In its place the CT scan rate will rise to between 6% and 8% depending on how clinicians apply the vomiting recommendation.
Clinicians managing service provision not only require an insight into the mean number of investigations required by the NICE guidelines but also the likely upper limits. A theoretical cohort of 100 patients was modelled in order to obtain clinically relevant confidence intervals. This number was chosen as it represents about one month of head injury attendances in a medium sized emergency department. It was found that using an interpretation of the vomiting criterion of three or more, while the mean CT rate was 6.3% the upper limit of CT scan requests can be expected to be around 11% of all emergency department attendances.
We have shown that a large number of the requested CT scans will be performed due to the presence of vomiting. Furthermore, we have shown that the way in which this criterion is interpreted by clinicians will be of paramount importance in the number of scans performed.
Our cohort of patients is in the childhood population only. Although the NICE guidelines are the same for adults and children, children are more likely to vomit than adults. Therefore in order to try and provide some indication as to the likely CT scan rates in adults, we performed a subanalysis with only the patients from 12–16 years of age in our database. We found a 10.7% CT scan rate, which is similar to the scan rate for all children. Although adolescents have a lower incidence of vomiting and therefore may be expected to have a lower CT rate, there is a higher rate of very minor head injuries in the very young. This may account for our finding that the CT rate was similar for adolescents and younger patients. We propose that it is likely that our findings in adolescents may be extrapolated to young and middle aged adults, although the major confounding factor is likely to be alcohol consumption. The intoxication rate in our adolescent age group was less than 1%, whereas in young adult populations this rate may be as high as 50%. However, the NICE guidelines make no specific recommendations regarding presence of intoxication, and patients will qualify for a CT scan only when the level of intoxication is enough to reduce their GCS.
A weakness of our paper is that the figures for management dictated by the NICE guidelines were assessed retrospectively for our database rather than prospectively looking at how physicians apply the guidelines. We can therefore not comment on how physicians will apply the NICE guidelines. We predict however that while the CT guidelines are likely to be closely followed, physicians may request a CT scan in vomiting patients less often than recommended, and may either observe or admit these patients, as physicians may be uncomfortable discharging a vomiting patient even with a normal CT scan.
To our knowledge, there have been no other studies modelling the impact of the NICE guidelines in paediatric head injuries. Our findings of current practice are similar to those of other cohort studies looking at all severities of head injuries in children in the UK. Lloyd and colleagues15 reported a cohort of 9269 childhood head injuries from 1993 to 1995 in the UK. They found a SXR rate of 64% and an admission rate of 9.1%. Their CT scan rate was 1.7%, with skull fracture being the most common reason for a CT scan.
Nee and colleagues16 reported a cohort of 5416 children and adults with head injury and found an incidence of 12% for vomiting in children, of which 3.6% were multiple vomits. A study of 12 395 patients that had sustained a head injury in Chester (published 1978) found that 7% of all patients had vomited.17 Boulis and colleagues18 reported a cohort of 1000 children with head injury having a SXR at the Royal Free Hospital and found an incidence of 17% for vomiting, 7% loss of consciousness, and 9% headache. They reported that the most common reason for requesting a SXR was soft tissue injury to the scalp.
We have also found a marked difference between actual management and the guidelines that the clinicians had been asked to follow. Strict adherence to the RCS guidelines would have resulted in a 50% SXR rate, a 1.6% CT scan rate, and a 7.1% admission rate. In clinical practice we found that the rate was half this for each category, at 25%, 0.9% and 3.7% respectively. Our findings that clinicians were not closely following the RCS guidelines are in agreement with a previous study that found a 47% non-adherence to guidelines for SXRs when the use of the Harrogate criteria was assessed in 1990.19
Finally, our finding that the NICE guidelines do not actually increase the number of patients that are being labelled as “high risk” is interesting. Taking the liberal interpretation of vomiting, the RCS guidelines allocated 7.2% of all patients as high risk, whereas the NICE guidelines allocate 6.5% as high risk. Therefore the effect of the NICE guidelines is not to increase the workload of clinicians caring for head injured patients but to move this workload from the observation ward to the radiology department.
Conclusion
The NICE guidelines will result in a CT scan rate of 6–9% for all children attending the emergency department with head injury, with an upper limit to this figure not exceeding 14%. The interpretation of the severity of vomiting will have a great impact on this figure, but overall the NICE guidelines do not increase the number of patients allocated as high risk; they merely move their treatment from the ward to the radiology department.
REFERENCES
Footnotes
Grant support: The Emergency Medicine Research Group is grateful for the support given by the Enid Linder Research Fellowship from the Royal College of Surgeons of England, and a grant from the Children’s Brain Injury Trust
The research was performed at the Emergency Medicine Research group, Department of Accident and Emergency Medicine, Manchester Royal Infirmary, Oxford Road, Manchester M13 9WL, UK
Linked Articles
- Atoms