Article Text

Abstract
Background Most guidelines recommend the use of capillary refill time (CRT) as part of the routine assessment of unwell children, but there is little consensus on the optimum method of measurement and cut-off time.
Methods We searched Medline (from 1948), Embase (from 1980) and CINAHL (from 1991) to June 2014 to identify studies with information on the normal range of CRT in healthy children, the validity of CRT compared with reference standard measures of haemodynamic status, reliability and factors influencing measurement of CRT, such as body site, pressing time and temperature.
Findings We included 21 studies on 1915 children. Four studies provided information on the relationship between CRT and measures of cardiovascular status, 13 provided data on the normal range of CRT, 7 provided data on reliability and 10 assessed the effect of various confounding factors. In children over 7 days of age, the upper limit of normal CRT is approximately 2 s when measured on a finger, and 4 s when measured on the chest or foot, irrespective of whether the child is feverish or not. Longer pressing times and ambient temperature outside 20°C–25°C are associated with longer CRT. Evidence suggests that the use of stopwatches reduces variability between observers.
Interpretation We recommend use of the following standardised CRT method of measurement: press on the finger for 5 s using moderate pressure at an ambient temperature of 20°C–25°C. A capillary refill time of 3 s or more should be considered abnormal.
- Evidence Based Medicine
- General Paediatrics
- Measurement
Statistics from Altmetric.com
What is already known on this topic
-
Capillary refill time (CRT) is widely used to evaluate haemodynamic status in children.
-
Measurement of CRT requires no equipment and can be performed quickly in any setting.
-
Prolonged CRT is a red flag for serious illness in children.
What this study adds
-
Normal capillary refill time (CRT) at the finger in healthy children should be 2 s or less.
-
CRT is sensitive to the method of measurement, including anatomical site of the measurement.
-
CRT should not be used as a surrogate for blood pressure, although it does correlate with other cardiovascular parameters.
Introduction
Measurement of capillary refill time (CRT) has been recognised since the 1930s1 ,2 as a potential means of assessing peripheral circulation. It came into common use after 1980, when a CRT of >2 s was incorporated into the Trauma Score, designed for assessing injury severity at the first contact with medical care.3
In children, CRT is most commonly used to evaluate haemodynamic status.4 ,5 Several systematic reviews of clinical predictors of serious illness in children have highlighted prolonged CRT as a red flag feature,6–9 and many clinical guidelines for the assessment of acutely unwell children recommend measuring CRT.10–15
Despite this, there is little consensus among clinicians, guidelines or textbooks on the optimum body sites, pressing times, pressure levels and cut-offs for CRT.16 Thresholds are typically described using terms such as ‘delayed’ or ‘prolonged’ rather than specific timed cut-offs.11 Moreover, there is currently no guidance for clinicians on the importance of factors such as ambient temperature or presence of fever, for interpreting CRT.
In this systematic review, we aimed to determine the normal range of CRT in healthy children, the validity of CRT compared with reference standard measures of haemodynamic status, reliability (interobserver and intraobserver agreement) and the factors that influence measurement and interpretation of CRT (including body site, pressing time, child's temperature and ambient temperature).
Methods
Search strategy
In collaboration with an information specialist, we developed a comprehensive search strategy (see web appendix 1). We searched three bibliographic databases (Medline from 1948, Embase from 1980 and Cumulative Index to Nursing and Allied Health Literature (CINAHL) from 1991, until 24 June 2014), to identify studies related to assessment of normal ranges of CRT in children, reliability, comparison with reference standards, and the influence of confounding factors. We identified additional studies from the reference lists of relevant papers and consultation with experts. Searches were restricted to papers published in English.
Inclusion and exclusion criteria
Selection was performed independently by two researchers. Eligible primary studies reported measurement of CRT by any manual method on a minimum of 20 children under the age of 18 years. Studies including individuals older than 18 years or neonates born prematurely (<35 weeks gestation), were included only if it was possible to extract data excluding those individuals. We excluded papers in which more than 50% of subjects had pre-existing cardiorespiratory disease (e.g. cardiac malformations).
We applied additional selection criteria for studies defining normal ranges of CRT. The subjects in these studies had to be afebrile and free of any illnesses likely to cause changes to CRT, including trauma, infection, respiratory, cardiac and gastrointestinal disease. Studies comparing CRT with reference standards of haemodynamic status required a suitable objective comparator considered relevant to peripheral tissue perfusion by the clinical authors.
Quality criteria
Quality assessment criteria were based on the Quality Assessment of Diagnostic Accuracy Studies-2 checklist19 and included patient selection, performance of the index test (CRT), performance of the comparator, and aspects of timing and flow (see web appendix 2). Quality assessment was completed by one author and checked by a second author.
Data extraction
Data on patient characteristics, study design, method of measuring CRT and relevant outcomes were extracted from included studies by one author using a prespecified form, and checked by a second author, with any disagreements resolved by consensus.
Analysis
Results are mainly descriptive, with attempts made to identify and explain differences between studies and heterogeneity in results. We defined 1 s as the minimum clinically important change in CRT. In both the guidelines and the clinical studies, 2 s and 3 s are common cut-offs for CRT, so a 1 s change in CRT has potential to affect clinical decision making.
For normal ranges, we extracted the mean and SD of CRT measurements. Following statistical convention, the upper limit of the normal range was defined as the mean +1.96 SDs. For a normally distributed measure, this corresponds to 97.5th centile, i.e. 2.5% of measurements would be expected to lie above this limit.
When at least two independent measurements of the upper limit of the normal range could be calculated for a given body site and age range, meta-analysis was carried out using a random-effects model, and heterogeneity (I2) values calculated. Summary measures were only reported when I2 <50%. All statistical calculations were carried out in R (V.3.0.1.).
In cases where multiple non-independent measurements were available from a single source, one measurement was used for the meta-analysis. This was chosen as the first observer described in the Methods section for multiple observers or the measurement method corresponding most closely to other studies for studies using multiple methods. Finally, given that the cardiovascular system undergoes physiological changes in the first few days of life, where possible, we analysed data from newborn infants (≤7 days) and older infants/children separately. Where a study reported data from different groups of normal children separately, these were pooled prior to meta-analysis.
Role of the funding source
The funding bodies had no input into the design of this review; collection, analysis or interpretation of data; writing of this report; or the decision to submit the paper for publication.
Results
After removal of duplicates, our search identified 527 studies, of which 309 were excluded after abstract and title review (figure 1). Of 214 full text articles screened by two reviewers, 21 were included in the current review. Of the included papers, 15 described studies carried out in high-income countries (as determined by the World Bank20), with the remaining 6 describing studies carried out in middle-income or low-income countries. Full details of individual study characteristics are given in table 1.
Characteristics of included studies

Flow chart for papers identified by search strategy. CRT, capillary refill time.
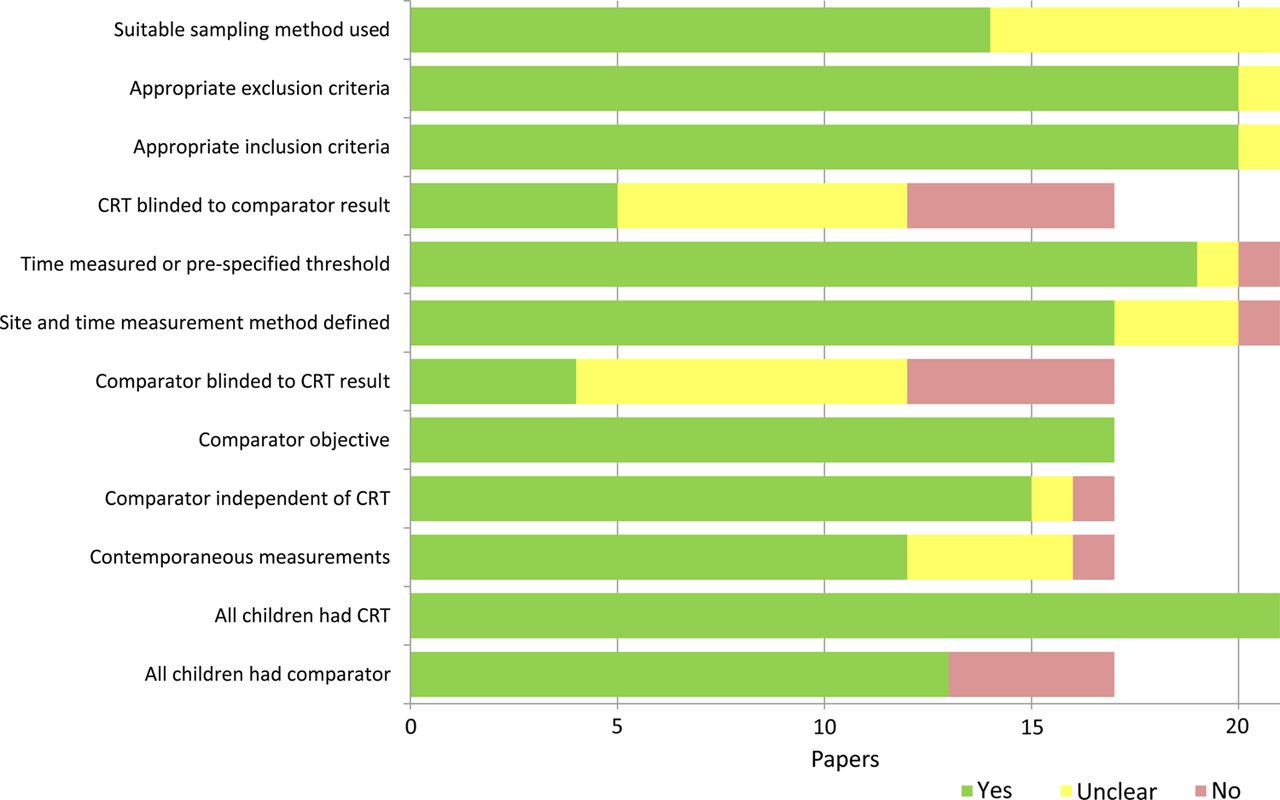
Quality assessment of included studies is summarised in figure 2, with full details in web appendix 3. Quality was generally good; all studies measured CRT on all included children and all comparators were judged to be objective. The lowest quality scores were found in the two criteria related to blinding. This was generally poorly reported, but sometimes impossible to implement, e.g. when investigating the effect of site of measurement or pressing time.

Bar chart showing quality assessment of included papers. Four papers with detail on normal ranges only are excluded from assessments of some quality criteria. CRT, capillary refill time.
Relationship between CRT and other measures of cardiovascular status
Each of the four included studies (111 children) investigated different measures, and was small (maximum 42 subjects). In healthy children, decreased arterial blood flow in the lower limb induced by inflation of a tourniquet was associated with increased CRT of just under 1 s for a 10-fold decrease in arterial blood flow.21 A study of healthy neonates found no clear correlation between CRT and blood pressure.22
Two studies investigated correlations between CRT and measurements of cardiovascular status using cardiac catheters in intensive care settings. The children mostly had acute infections, such as septic shock and pneumonia. One study found positive predictive values of 93%–96% and negative predictive values of 40%–50%, depending on the site used for CRT measurement, for CRT >2 s to predict low superior vena cava oxygenation (≤70%).23 The second found significant correlations between CRT and both core-peripheral temperature gap (r=0.66, p<0.0001) and stroke volume index (r=−0.46, p=0.001), although no significant correlation was seen with cardiac index or systemic vascular resistance index.24 The same study noted a weak correlation (r=0.34, p=0.02) between CRT and central venous pressure.
Normal ranges of CRT
Seven of the 13 studies (n=1252) reporting normal ranges were conducted in 953 newborn infants up to 7 days of age. We present data on normal ranges in newborn infants and older children separately, organised by body site, as three studies in children of both age groups found clinically relevant differences in CRT measured at different sites.17 ,25 ,26
Figure 3 shows a forest plot of the upper limit of the normal range for newborn infants up to 7 days of age, measured at six sites: the head, chest, abdomen, hand, finger and foot. Significant statistical heterogeneity was not explained by clinical factors and was present at all sites, so summary results are not reported. Upper limits of the normal range of CRT in newborns ranged from 2.5 s to over 7 s. The largest range of values was seen at the foot, but upper limits of over 5 s were also found at the finger, hand and chest.

Forest plot of upper limits of capillary refill time (CRT) in normal infants (≤7 days of age). Data from the 3–4 s pressing time in the LeFlore and Engle22 study were included in the meta-analysis, as this corresponded more closely to the pressing times reported by other included studies, which were typically 3 or 5 s. *Excluded from meta-analysis as multiple measurements were made on the same participants.
Data on the upper limit of the normal range of CRT for older children (1 week–18 years) (figure 4) was available from three sites: the chest, finger and foot. In most of the included studies, the anatomic site was pressed for 5 s. The summary upper limit for CRT measured at the foot was 4.05 s (95% CI 3.61 to 4.49 s). Unexplained significant heterogeneity (I2>75%) was present in data from both the chest and finger, precluding summary estimates. However, all the 95% CI for the upper limit at the chest were below 4 s. At the finger, the maximum upper limit for CRT was 2.08 s; all the 95% CI for the upper limits were below 2.5 s.

Forest plot of capillary refill time (CRT) in normal infants and children 7 days to 18 years of age. ^Excluded from meta-analysis as paper reported median and 95th percentile (shown), rather than mean and SD. *Excluded from meta-analysis as multiple measurements were made on the same participants.
Three studies, all on normal newborn infants, reported the distribution of CRT values measured at different sites. Two27 ,28 reported that measurements made at the head and chest approximated a normal distribution, those at the hand appeared less normal and those at the foot were more widely scattered. However, the third study reported a normal distribution for measurements made at the hand and foot.18
Four studies assessing the difference in normal range with age were identified, of which three investigated only infants in the first week of life.18 ,22 ,29 The fourth was limited by small sample size (n=8 in each age group) and did not report consistent results at different body sites.17
Effect of confounding factors on CRT values
Effect of body site
Eight studies (n=691) investigated the relation between measurement site and CRT (table 2). Most assessed healthy children or infants, and were comparable in terms of pressing time and measurement method (e.g. stopwatch), although the amount of pressure used and the number of observers varied.
Comparison of capillary refill time (CRT) measured at different body sites
Included studies assessed CRT at eight body sites: forehead, sternum/chest, hand, finger, lower abdomen, thigh, heel and sole/foot (figure 5). All but one study30 found statistically significant differences, with clinically significant differences (>1 s) between mean CRT at different sites in three studies.17 ,25 ,30 Measurements on the lower extremities were typically longer than those on the upper extremities, head or chest.

Visualisation of comparisons between capillary refill time at different sites. Thin lines indicate a single comparison between two sites. Multiple comparisons are indicated with thicker lines labelled with the number of comparisons.
Effect of pressing time
Pressing time was examined in two studies of 322 healthy term infants (figure 6).22 ,27 One study22 compared pressing times of 1–2 s and 3–4 s at the finger, chest and heel on 42 infants, and found CRT significantly increased by 1.2–1.4 s with longer pressing times. The second study27 also found significantly longer CRT for most of the longer pressing times at the head and chest, but differences were small (0.17–0.42 s) and inconsistent (see web appendix 4). Pressing times did not influence CRT at the heel.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of differences in capillary refill time (CRT) with various pressing times in healthy infants (≤7 days of age). ^Strozik et al27 compared seven pressing times (1, 2, 3, 4, 5, 6 and 7 s), at each of three sites (head, chest and heel), as well as composite data for pressing times of 3–7 s for the head and chest. Comparisons were not pairwise, as each pressing time was tested on 40 independent infants, therefore, we selected the following clinically relevant pairs for comparison: 7 vs 1 s, 3 vs 1 s, 4 vs 2 s, 5 vs 2 s, 5 vs 3 s, and, where possible, 3–7 vs 1 s.
Effect of ambient, skin and core temperatures
Four studies on 558 children investigated the effects of ambient, skin and core temperatures. Two provided data on the effect of ambient temperature on CRT in 292 neonates and another on 32 older children (see web appendix 5). Studies varied in the room temperatures compared, body sites and population characteristics, precluding meta-analysis. Two17 ,18 reported significant inverse correlations between ambient temperatures and CRT, with a 5°C decrease in ambient temperature resulting in >1 s increase in CRT in one study.17 Conversely, a third study found a significant positive correlation, at ambient temperatures of 26°C–30°C.29
Two studies17 ,18 assessing the relationship between CRT and skin temperature at the measurement site also found inverse correlations. A further two studies compared the effect of core temperature on CRT. One18 found a statistically significant relationship, although a decrease of 2°C–3°C in core temperature would be required for a 1 s increase in CRT. The second study31 found no significant difference in CRT between febrile (core temperature >38.3°C) and afebrile children.
Reliability of CRT measurement
We found limited evidence regarding reliability of CRT measurements. Seven studies examined interobserver reliability on 485 children (web appendix 6), but results were highly variable, with reliability ranging from poor (κ<0.15)32 ,33 to good (κ=0.54 and 0.65).17 ,34 Using stopwatches to measure CRT appeared to be associated with better interobserver reliability.
There was even less data on intraobserver reliability. One small study in 32 children found strong agreement (ICC=0.96) between three repeated measures17 and a second study in 20 children showed that CRT decreased with successive measurements at the same site (p<0.0001).18
Discussion
This review reveals that in healthy children, CRT measured on a finger should be 2 s or less (although some healthy children may have a CRT at this site of up to 2.5 s), with an upper limit of 4 s for measurements made on the chest or foot. In neonates aged 7 days or less, the upper limit of normal CRT may extend up to 5 s –7 s at some body sites.
Multiple studies suggest that anatomical site affects CRT. Measurements made on the lower extremities tend to result in longer times than those made on the upper extremities, head or chest. Lower skin temperatures increase CRT, with potential for clinically significant changes, and there may be a similar effect with lower ambient temperature. However, there is no clear evidence that fever results in clinically significant changes. CRT is highly variable between different observers, possibly related to the method of measurement; standardisation of CRT measurements is warranted to decrease variability. In neonates, there is evidence that longer pressing times are associated with longer CRT. Finally, although CRT appears to correlate well with various markers of cardiovascular status, there is little evidence to demonstrate a clear association between CRT and blood pressure; this may be largely related to variation in normal blood pressure in healthy children.
We used a comprehensive literature search with broad search terms and citation searching to identify all potentially relevant studies. We included data from 10 countries from high-income (5 countries), middle-income (4 countries) and low-income (1 country) settings, making the results likely to be applicable worldwide. As with any systematic review, the conclusions are limited by the number, quality and variability of identified studies. We found few studies that quantified the association between CRT and reference standards for haemodynamic status. Studies inconsistently reported the exact methods used to measure CRT and other possible confounding factors. This limited our ability to conduct a formal meta-analysis of the results, or in some cases draw firm conclusions. Where meta-analysis was possible, we identified high levels of heterogeneity, which, in the absence of apparent clinical differences between studies, may be explained by interobserver variability and unreported differences in measurement technique. The small number of included studies precluded subgroup analysis of only high-quality studies, or based on setting or country.
By contrast with heart rate, which varies markedly with body temperature, CRT does not appear to show clinically significant changes with fever.35 Additionally, while the relationship between age and normal range is complex for heart rate and breathing rate, our findings suggest a much simpler relationship with CRT. In part, this may reflect inaccuracies in its measurement and variability due to multiple observers, but imply a far simpler clinical application than other vital signs.
Existing guidelines for feverish or acutely ill children often recommend measuring CRT, yet provide little detail on how exactly it should be measured, merely stating threshold values, with little or no recommendations for clinicians on where and how to measure CRT.12 ,13 Clear evidence-based recommendations are needed to ensure consistent clinical use of CRT in children. Standardising measurements could improve the use and reliability of CRT.
Our findings have several implications for practice. First, individual clinicians should reassess how they measure and interpret CRT based on this evidence. Second, clinical settings should implement standardised methods, to ensure that CRT measured in one area (e.g. the emergency department) can be compared with assessments made in a different clinical area (e.g. the inpatient ward). Finally, guideline developers and triage scoring systems should recommend a single measurement method, incorporating a clear pressing time, body site and the use of a timer or stopwatch.
Taking into account our findings based on current evidence, we propose the standardised measurement method for CRT given in the box 1. We urge researchers and writers of clinical guidelines to document the technique used or recommended for recording CRT measurement including the body site, pressure time and method of counting. We recommend that clinicians measuring CRT should use the standardised protocol in the box 1, documenting the precise time (e.g. 4 s rather than ‘prolonged’) and any deviations from the recommendations.
Standardised measurement method for capillary refill time (CRT)
-
Use the finger as the preferred measurement site.
-
Press for 5 s using moderate pressure.
-
Ideally, maintain an ambient temperature of 20°C–25°C irrespective of child's body temperature. Allow time for skin temperature to acclimatise if the child has recently been moved from a warmer or colder environment.
-
Use a stopwatch or timer to measure CRT.
-
Apply a cut-off of 3 s or more to define abnormal CRT in infants and children over 7 days of age. Normal CRT in this age group is considered to be 2 s or less. A CRT measurement of between 2 and 3 s may be considered to be ‘borderline abnormal’, but it should be noted that some healthy children may have CRT as long as 2.5 s.
For clarity, cut-offs should be defined using terminology such as ‘2 seconds or less’ or ‘3 seconds or more’, rather than using mathematical inequality symbols. Use of mathematical inequalities (e.g. >2 s) to define cut-offs for CRT can lead to confusion, particularly as CRT is typically measured by counting, and so measurements of non-integer seconds are uncommon. Therefore, a cut-off of >2 s may be functionally equivalent to one of ≥3 s, but visually is more similar to one of ≥2 s. We, therefore, recommend that mathematical inequalities are not used to define CRT cut-offs, but rather that inclusive wording such as ‘2 seconds or less’ or ‘3 seconds or more’ is used, which reduces ambiguity.
The lack of published data on key aspects of the measurement and interpretation of CRT is surprising, given the prominent place it has in clinical assessment and emergency triage scores for children worldwide and the relative ease of measurement. Priority areas to be addressed include the relationship between CRT and reference standards of cardiovascular status (to determine whether CRT is a true proxy for underlying status), and more robust examination of normal ranges of CRT, optimal duration of pressure, and intraobserver and interobserver reliability, particularly in clinical settings, where reliability is likely to be worse than in research settings. Finally, while we only included studies of manual measurement, we are aware of one automated method for measuring CRT36 and encourage further studies of similar devices.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online appendix
Footnotes
-
Contributors SF, PG, JAT, AVdB and MT developed the protocol and identified papers for inclusion. SF, PG and CJ carried out the analysis. All authors contributed to the final manuscript. SF had full access to all the data in the review and had final responsibility for the decision to submit for publication.
-
Funding This paper presents independent research funded by the European Union Seventh Framework Programme (FP7/2007–2013) under grant agreement no 305292 for the programme ‘Supporting Life’.
-
Competing interests SF was funded by a fellowship award from the National Institute for Health Research School for Primary Care Research (NIHR SPCR). PG received funding from the Rhodes Trust, Alberta Innovates—Health Solutions, and the Canadian Institute of Health Research. JAT was funded by the University of Washington Pediatric Endowed Professorship for Research Sabbaticals. CH also received funding from the NIHR SPCR. The views expressed in this paper are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement As this is a systematic review, most unpublished data should be in the public domain. However, additional unpublished data will be made available to researchers on application to the authors.