Article Text

Abstract
The presentation, investigation, and management of four patients with spontaneous spinal epidural haematoma is presented. In each case the diagnosis was made by MRI. At the time of diagnosis spontaneous recovery had started in each patient and therefore they were all treated conservatively. In each case follow up MRI confirmed rapid reduction in the size of the haematoma and no underlying cause was demonstrated. The presentation, diagnosis, and rationale for treatment are discussed. Conservative treatment is safe in some cases of spinal epidural haematoma if early neurological recovery has started.
- haematoma
- epidural
- spine
- treatment outcome
Statistics from Altmetric.com
Spinal epidural haematoma is a rare condition, which may be due to trauma, surgery, epidural catheterisation or disorders of coagulation. In 40%-50% of cases no cause is found and a diagnosis of spontaneous spinal epidural haematoma is appropriate.1 The incidence of spontaneous spinal epidural haematoma is estimated at 0.1/100 000/year.2 Whatever the cause of haemorrhage the mainstay of treatment is urgent surgical decompression and evacuation of the haematoma via a laminectomy.3 There are only a few reports of successful conservative treatment in this condition where symptoms and signs have resolved without surgery. We report on four patients with spontaneous epidural haematomas all treated conservatively with good neurological outcome. The presentation, investigation, and management of the condition are reviewed.
Case reports
PATIENT 1
A 72 year old man developed sudden onset of pain in the cervical spine which radiated to his right arm. Weakness began in the right leg but progressed to the left leg and then to the arms. He was admitted to his local hospital and referred to the neurosurgical unit 24 hours later. Neurological examination showed a profound right sided and milder left sided limb weakness with a sensory level at T8.
Haematological tests were normal. An urgent MRI showed that the spinal cord was compressed by a right posterolateral epidural mass extending from the inferior border of C2 to the midbody of T2 (fig 1). On T1 weighted images the mass was slightly hyperintense compared with the cord. On T2 weighted sections it was almost as bright as CSF. There was no enhancement with contrast.

Fast spin echo sagittal T2 weighted MRI. The epidural lesion is isointense but slightly heterogeneous compared with CSF. The low signal intensity of the dura separating the lesion and cord is clearly seen.
A diagnosis of spontaneous epidural haematoma was made on the basis of the clinical history and MR appearances. The patient's condition was improving and he was managed conservatively with initial bed rest, a hard cervical collar, and dexamethasone. Three days later he was walking with assistance. A repeat MRI 6 days after admission demonstrated reduced cord compression. The mass now showed a high signal on T1 weighted images consistent with the presence of methaemoglobin.
Four months later the patient had normal power and only mild hyperaesthesia on the left side. A further MRI showed resolution of the epidural mass and no intrinsic cord abnormality.
PATIENT 2
This 64 year old housewife complained of sudden onset of pain radiating to the left arm while on holiday in the Channel Islands. Within 30 minutes she developed weakness in the right arm and leg and was unable to stand. Weakness then progressed to involve the left arm and leg. On examination in the local hospital she had a severe flaccid tetraparesis with a pin prick sensory level on the left below C6. The patient was transferred to the neurosurgical unit in Southampton by air and arrived 5 hours after the onset of symptoms.
At initial assessment in the neurosurgical unit there had been considerable motor and sensory improvement. Blood tests including coagulation were normal.
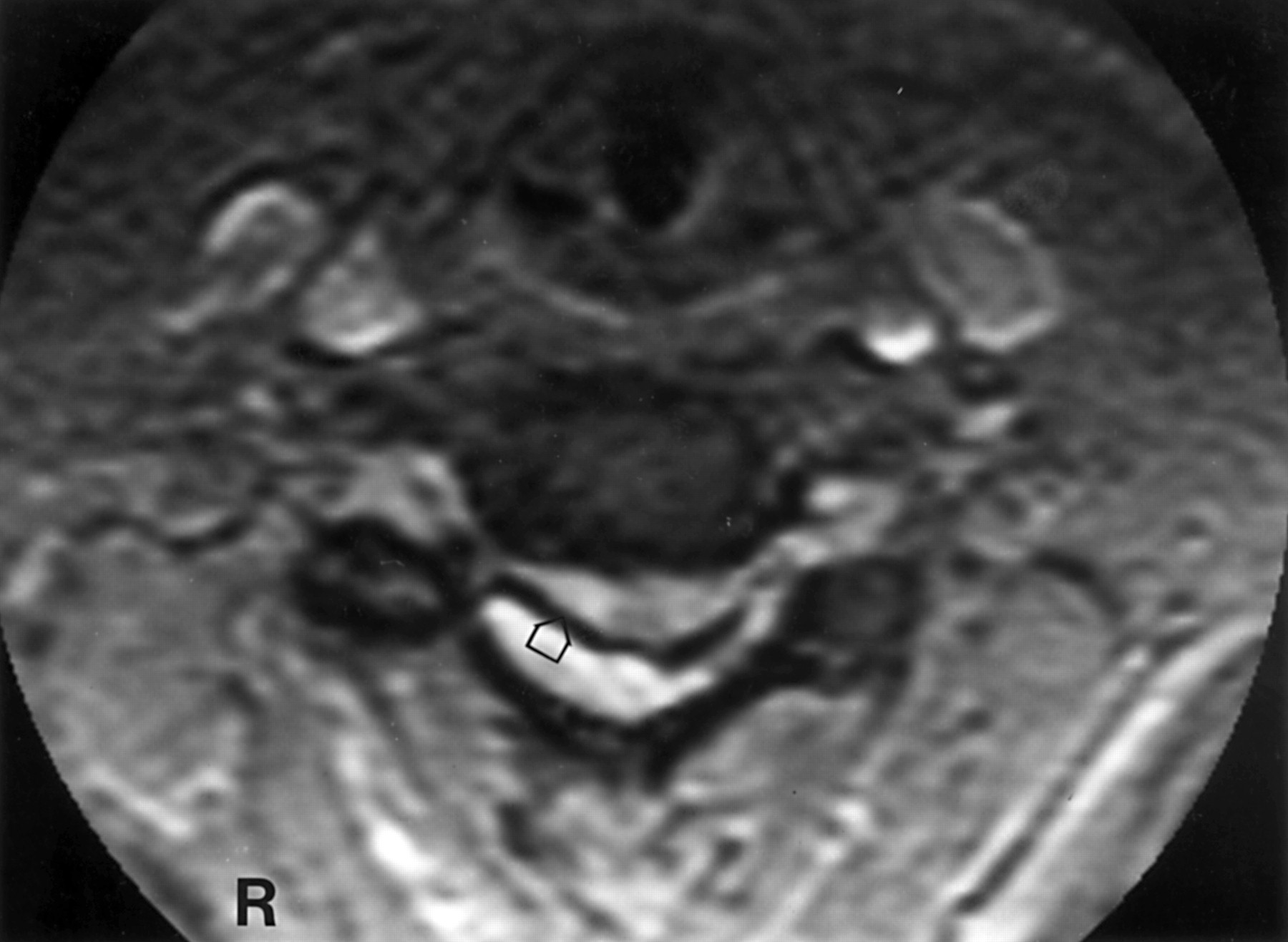
An urgent MR scan was performed and demonstrated a posteriorly situated epidural mass extending from C2 to T1 causing spinal cord compression between C3 and C6, maximal at C4/5. The mass was hyperintense to the cord and slightly hypointense to CSF on T2 weighted images and slightly hyperintense to the cord on the T1 weighted sequence. There was a small area of high signal within the cord on T2 weighted images at C4/5 (fig2).
{kind=link}
{kind=link}
Gradient echo (GE) axial T2 weighted MRI at the level of C5 showing the hyperintense lesion posterolaterally on the right displacing and compressing the cord. Note prominent signal void in the anterior aspect of the lesion consistent with susceptibility artefact from the presence of deoxyhaemoglobin (arrow). There is high signal within the cord.
The patient's condition was rapidly improving and she was therefore treated conservatively. Six days later a further MR scan showed reduction in size of the epidural mass. At discharge 26 days later she was able to walk with a stick and climb stairs. An MR scan 6 weeks later showed complete resolution of the haematoma.
PATIENT 3
This 68 year old woman developed severe thoracic back pain while opening her bowels. She developed paraesthesiae in the lower limbs and then weakness. On admission to the local hospital she was hypertensive and in atrial fibrillation. There was a flaccid paralysis of the legs with pinprick reduced below T6 on the left and T10 on the right. An initial diagnosis of aortic dissection with an ischaemic paraplegia was made.
An MR scan performed after 48 hours demonstrated a posteriorly placed epidural mass extending from the upper to lower thoracic spine with cord compression from T4 to T11. On gradient echo images signal void was seen in the anterior margin of the mass consistent with the presence of deoxyhaemoglobin. After the MR scan the patient was referred to the neurosurgical unit.
On admission rapid neurological improvement was occurring. This continued and 10 days later she was mobilising well and was discharged to her local hospital. She remained well initially but then had a haemorrhage of the large bowel and required exploratory laparotomy and colostomy for a rectal ulcer, sigmoid abscess, and rectovaginal fistula. Despite transfer to the intensive care unit she died 1 month later. At postmortem there was evidence of old epidural haemorrhage; no other spinal abnormality was found.
PATIENT 4
This 28 year man noticed interscapular pain while walking. This was followed by paraesthesiae in the right leg, then numbness; the symptoms progressed to involve the left side and over 24 hours he developed severe weakness and urinary retention.
The patient was referred to the neurosurgical unit 48 hours after the initial onset of symptoms. On examination power was grade 1–3/5 in the right leg. There was reduced sensation below the T5 level.An urgent MR scan identified a posterior epidural mass extending from C7/T1 to T5/6. This was isointense to the cord on T1 weighted images and appeared heterogeneous and approximately isointense to CSF on T2 weighted sequences. On axial, gradient echo T2 weighted images, heterogeneous signal with prominent low signal was seen highly suggestive of the presence of blood with deoxyhaemoglobin formation.
In view of the recovery that was already taking place the patient was treated with steroids. One week later only mild sensory disturbance remained. Repeat MR showed almost complete resolution of the haematoma with no underlying abnormalities.
Discussion
In 40%-50% of cases of spinal epidural haematoma no cause can be identified.1 In the remainder trauma, whether accidental or surgical, often precedes the haematoma and epidural catheterisation may also be responsible.3 Other causes include coagulation disorders and anticoagulation therapy, arteriovenous malformation, cavernous angioma, and Paget's disease.3-6Spontaneous epidural haematoma has also been described after thrombolytic therapy.
The clinical presentation of epidural haematoma is usually of sudden severe spinal pain that may radiate to the limbs. Radicular pain may precede spinal pain.5 7 Neurological symptoms then develop rapidly, with varying degrees of motor and sensory loss and bladder involvement.8
The condition is a neurological emergency and requires urgent investigation and treatment. The investigation of choice is MR scanning.2 5 9 In the first 24 hours an epidural haematoma is uniformly isointense with the cord on T1 weighted images. On T2 weighted images it is usually hyperintense although it may be heterogeneous.2 10-12 An important feature is the early detection of deoxyhaemoglobin. It gives rise to low signal intensity due to a local magnetic susceptibility effect and this is most obvious on T2 weighted gradient echo sequences. By 48 hours the haematoma gives an increased signal on T1 weighted images and remains hyperintense on T2 weighted sequences.2 10-12 A negative scan once the blood has resolved probably removes the need for spinal angiography although small, low flow vascular malformations could escape detection on MRI.
In almost all cases of spinal epidural haematoma surgical evacuation via a laminectomy is necessary. The extent of neurological recovery has been shown to be related to the interval between the onset of symptoms and surgery and also the degree of neurological deficit.1 3 5 7 13-15 Conservative treatment usually results in a poor outcome, particularly when the haematoma compresses the cervical cord.8 12 There is, however, an increasing number of reports of individual cases managed conservatively.16-21 In epidural haematoma due to coagulopathy, treatment with replacement clotting factors has resulted in resolution of the haematoma without surgical intervention.6 Boukobza et al, in their paper describing the MR appearances of spinal epidural haematomas, included five patients who did not have surgery. An MR scan was performed 24 to 48 hours after the onset of symptoms.11 Holtas et al, while describing the MR appearances and clinical correlations of spontaneous spinal epidural haematoma, report 11 of 13 patients treated conservatively with good outcomes.2 Jamjoom noted the increase in both the number of cases of spontaneous spinal epidural haematomas being reported and the increase in the number not requiring surgery since the advent of MRI.23
All the patients in this series had improving neurological signs at the time of arrival in the neurosurgical unit, which was 5 to 48 hours after the ictus. The longer intervals before referral were due to delay in recognition of the need for neurosurgical referral in the referring hospitals (patients 1 and 4), the logistical difficulty of transfer (patient 2), and an initial incorrect diagnosis with delayed scanning (patient 3).
The diagnosis of epidural haemorrhage was confirmed on MR scanning in all cases although in two patients alternative diagnoses were suggested after the initial scan. In patient 4 the presence of some enhancement raised the possibility of extradural abscess but there was insufficient clinical evidence to support this. Extradural tumour, possibly lymphoma, was considered in patient 2 but was discounted after repeat imaging. All our patients were treated with a course of steroids followed by mobilisation when recovery allowed and a repeat MR scan at 1 week. The decision not to operate was based on the recovery occurring in each patient at the time of presentation. All were closely watched in the regional neurological centre with on site facilities available for emergency MR scanning and neurosurgery. Laminectomy and evacuation of the haematoma would have been performed if any patient had not improved. Good neurological outcome occurred in all of these cases and all were able to walk within 1 week of initial presentation. On the basis of these and other reports it seems safe to treat cases of spinal epidural haematoma in whom recovery has started with observation and steroids, provided this is done only in neurosurgical centres. Cases have been reported where recovery was followed by deterioration requiring surgery.23 24Observation in a hospital without neurosurgical services is therefore inappropriate.
Conclusion
Accurate diagnosis of epidural haematoma is pivotal if conservative management is to be adopted and urgent MR scanning is mandatory. Suspicion of the diagnosis therefore requires careful analysis of the signal characteristics of an epidural mass with regard to time since ictus. T2*weighted gradient echo sequences are particularly useful in the early stages due to their sensitivity for the detection of deoxyhaemoglobin.
The treatment in most cases remains urgent laminectomy and evacuation of the haematoma, but in a few patients in whom early recovery of function has started, a conservative policy seems justified. This should involve close observation in a neurosurgical unit with early repeat MR scanning. Surgical intervention may still be necessary if symptomatic recovery with haematoma resolution does not continue.