Article Text

Abstract
Objective To evaluate association between biomarkers and outcomes in COVID-19 hospitalised patients. COVID-19 pandemic has been a challenge. Biomarkers have always played an important role in clinical decision making in various infectious diseases. It is crucial to assess the role of biomarkers in evaluating severity of disease and appropriate allocation of resources.
Design and setting Systematic review and meta-analysis. English full text observational studies describing the laboratory findings and outcomes of COVID-19 hospitalised patients were identified searching PubMed, Web of Science, Scopus, medRxiv using Medical Subject Headings (MeSH) terms COVID-19 OR coronavirus OR SARS-CoV-2 OR 2019-nCoV from 1 December 2019 to 15 August 2020 following Meta-analyses Of Observational Studies in Epidemiology (MOOSE) guidelines.
Participants Studies having biomarkers, including lymphocyte, platelets, D-dimer, lactate dehydrogenase (LDH), C reactive protein (CRP), aspartate aminotransferase (AST), alanine aminotransferase (ALT), creatinine, procalcitonin (PCT) and creatine kinase (CK), and describing outcomes were selected with the consensus of three independent reviewers.
Main outcome measures Composite poor outcomes include intensive care unit admission, oxygen saturation <90%, invasive mechanical ventilation utilisation, severe disease, in-hospital admission and mortality. The OR and 95% CI were obtained and forest plots were created using random-effects models. Publication bias and heterogeneity were assessed by sensitivity analysis.
Results 32 studies with 10 491 confirmed COVID-19 patients were included. We found that lymphopenia (pooled-OR: 3.33 (95% CI: 2.51–4.41); p<0.00001), thrombocytopenia (2.36 (1.64–3.40); p<0.00001), elevated D-dimer (3.39 (2.66–4.33); p<0.00001), elevated CRP (4.37 (3.37–5.68); p<0.00001), elevated PCT (6.33 (4.24–9.45); p<0.00001), elevated CK (2.42 (1.35–4.32); p=0.003), elevated AST (2.75 (2.30–3.29); p<0.00001), elevated ALT (1.71 (1.32–2.20); p<0.00001), elevated creatinine (2.84 (1.80–4.46); p<0.00001) and LDH (5.48 (3.89–7.71); p<0.00001) were independently associated with higher risk of poor outcomes.
Conclusion Our study found a significant association between lymphopenia, thrombocytopenia and elevated levels of CRP, PCT, LDH, D-dimer and COVID-19 severity. The results have the potential to be used as an early biomarker to improve the management of COVID-19 patients, by identification of high-risk patients and appropriate allocation of healthcare resources in the pandemic.
- critical care
- evidence-based practice
- global health
- infectious disease medicine
- prognosis
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Data are collected from the studies published online, publicly available, and specific details related to data and/or analysis will be made available upon request.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Summary box
What is already known about this subject?
COVID-19 is rapidly spreading global pandemic with increased burden on healthcare. Few observational studies have described association between different biomarkers with severe outcomes.
Laboratory biomarkers are less expensive, faster and easier to obtain and preferred modality to monitor and predict outcomes and prognosis of disease.
What are the new findings?
In our meta-analysis of 32 studies reflective of 10 491 confirmed COVID-19 patients, we found that decreased lymphocyte count, a decreased platelet count and elevated C reactive protein, creatine kinase, procalcitonin, D-dimer, lactate dehydrogenase, alanine aminotransferase, aspartate aminotransferase and creatinine were associated with poor outcomes in COVID-19 hospitalised patients.
Meta-analysis has included studies from different geographic locations and hence results provide global findings and can be generalised.
How might it impact clinical practice in the foreseeable future?
The meta-analysis results show that there is clear evidence of association between different biomarkers and COVID-19 disease severity. This can be used as an adjunct in clinical practice to guide treatment and admission, helpful in improving prognosis and decreasing mortality rates, on evaluating accuracy of these biomarkers in future studies.
Introduction
COVID-19 was declared as a global pandemic by WHO on 11 March 2020.1 It has now spread to over 200 countries and territories worldwide. With the cumulative cases in the world approaching 22 million and cumulative deaths touching 796 281 (as of 20 August 2020), it has become a catastrophic public health crisis.2 The USA has surpassed all countries in the number of COVID-19 positive cases and now stands at over 5.5 million cases with more than 172 416 deaths as of 20 August 2020.3 Other countries with high case rates and disease burden are Brazil (3 407 354), India (2 836 925), Russia (942 106), South Africa (596 060) and Peru (549 321).4
This outbreak has been a challenge for clinicians and researchers alike. COVID-19 infection has a variable clinical presentation from asymptomatic to milder symptoms, including fever, dry cough, dyspnoea, myalgia, sore throat and headache, to more severe and emergent manifestation including confusion, chest pain, hypoxemia, pneumonia and other complications requiring intensive care unit (ICU) admission and mechanical ventilation.5–7 Diarrhoea, anosmia and ageusia have also been reported in a few studies,8–10 as well as neurologic manifestations.11–13 Researchers all over the globe have been searching for predictors of COVID-19 disease severity to identify and stratify them accordingly, in an effort to guide medical management. Insights into disease pathogenesis and methods to rapidly discern and assess COVID-19 infection are evolving. Laboratory biomarkers are less expensive, faster and easier to obtain. As such, they have been the preferred modality to monitor and predict outcomes and prognosis of disease.14 Understanding the variation and profile of specific biomarkers as a function of different COVID-19 outcomes would aid in the development of a risk stratified approach to the care of patients with this illness.
With the surge in COVID-19 cases across the globe due to its highly contagious nature, there have been numerous studies that have reported on the predictors of disease severity in COVID-19 patients. Studies have shown that severe or fatal cases of COVID-19 disease are associated with an elevated white cell count, blood urea nitrogen, creatinine, markers of liver and kidney function, C reactive protein (CRP), interleukin-6 (IL-6), lower lymphocyte (<1000/µL) and platelet counts (<100x109/L) as well as albumin levels compared with milder cases in which survival is the outcome.15–17 These studies offered an initial understanding of the impact of SARS-CoV-2 infection, but the findings cannot be generalised due to limitations of geographical locations, single centre experience and small cohorts.
Since laboratory medicine has always supported clinical decision making in various infectious diseases, it is important to assess the ability of laboratory-derived biomarkers to facilitate risk stratification of COVID-19 disease. Therefore, in the present systematic review and meta-analysis, we assessed the association between different laboratory biomarkers and outcomes in COVID-19 hospitalised patients.
Methods
Endpoint
The aim of the study is to evaluate the role of the laboratory biomarkers in predicting outcomes in COVID-19 hospitalised patients. COVID-19 confirmation was evaluated by combined findings of reverse transcription PCR, serology, symptoms and MRI chest in all the studies. The biomarkers included in the study were lymphocyte, platelets, D-dimer, lactate dehydrogenase (LDH), CRP, aspartate aminotransferase (AST), alanine aminotransferase (ALT), creatinine, procalcitonin (PCT) and creatine kinase (CK). Poor outcomes were defined by ICU admission, oxygen saturation (SpO2) <90%, invasive mechanical ventilation (IMV) utilisation, severe disease and in-hospital mortality. Study-specific poor outcomes and biomarkers are mentioned in table 1.
Study characteristics, outcomes and laboratory biomarkers
Search strategy and selection criteria
A systematic search was conducted on published studies using Meta-analyses Of Observational Studies in Epidemiology (MOOSE) guidelines18 from 1 December 2019 to 15 August 2020. We searched PubMed, Web of Science, Scopus and medRxiv for observational studies that described laboratory findings of COVID-19 patients following keyword/Medical Subject Headings (MeSH) terms: ((COVID-19 [Title/Abstract]) OR coronavirus [Title/Abstract]) OR SARS-CoV-2 [Title/Abstract] OR 2019-nCoV [Title/Abstract]. Studies were included in this meta-analysis if they had laboratory findings and outcomes of COVID-19 hospitalised patients. Literature other than observational studies, non-English literature, non-full text and animal studies were excluded. Flow diagram of the literature search and study selection process is described in figure 1.

Flow diagram of literature search and study selection process of COVID-19 outcomes and biomarkers.
Study selection
Abstracts were reviewed, and articles were retrieved and reviewed for availability of data on laboratory findings and outcomes of COVID-19 patients. Studies which gave details on outcomes were selected for quantitative analysis. PM and DM independently screened all identified studies and assessed full texts to decide eligibility. Any disagreement was resolved through discussion with another reviewer (UP).
Data extraction and quality assessment
From the included studies, we extracted the following variables relating to laboratory biomarkers and outcomes: lymphocytes count (cells/µL), platelet count (cells/µL), D-dimer (mg/L), LDH (U/L), CRP (mg/L), AST (U/L), ALT (U/L), creatinine (mg/dL), PCT (ng/mL) and CK (U/L). Details on binary outcomes like ICU versus non-ICU admission, severe versus non-severe disease (definitions in table 1), IMV versus no-IMV use, SpO2 <90% versus >90%, in-hospital mortality versus discharged alive and survivors were collected using prespecified data collection forms by two authors (PM and DM) with a common consensus of another author (UP) on disagreement. We have presented the study characteristics including the first author’s last name, publication month and year, country of origin, sample size, study period, mean or median age, sex, outcomes and biomarkers assessed in that individual study (table 1). Cut-off ranges for biomarkers used in the individual studies included in meta-analysis are mentioned in online supplemental file 1.
Supplemental material
Statistical analysis
Data analysis was performed using Review Manager V.5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). If the study has more than one outcome comparison, then we have used data from the most severe outcome in the analysis to minimise the overall selection bias of our study. The Mantel-Haenszel formula was used to calculate dichotomous variables to obtain ORs along with its 95% CIs to describe the relationship of laboratory biomarkers and outcomes of COVID-19 patients in each study. Random-effect models were used regardless of heterogeneity to estimate the combined effect and its precision, to give a more conservative estimate of the ORs and 95% CI. The I² statistic were used to assess statistical heterogeneity. The I² statistic of >50% was considered significant heterogeneity. P value <0.05 was considered significant. Publication bias was assessed visually using funnel plots (online supplemental file 1), the Newcastle-Ottawa Scale (NOS) and Quality in Prognostic Studies tool (online supplemental file 2). NOS was used to assess the quality and bias in the included studies, which rates selection, comparability and outcome.19 Risk of bias of included studies is described in online supplemental file 1. All studies were assessed to be of moderate quality. Sensitivity analysis was performed to assess the effect of publication bias and heterogeneity by excluding outlying studies on the funnel plot. The pooled-OR and 95% CI are represented in the form of forest plots. Each square on the chart area represents individual study, and the area of each square is equivalent to the weight of the study, which is the inverse of the study variance. The diamond represents the summary measures and the width corresponds to the 95% CI.
Supplemental material
Results
Literature screening and characteristics of included studies
Review of the databases identified 125 163 articles, out of which 200 full text articles assessed for eligibility after removing duplicated articles, non-human studies, non-observational studies and articles with non-English language. During the second round, 140 articles with insufficient clinical information on COVID-19 outcomes and biomarkers were excluded, and 60 articles on epidemiological characteristics, comorbidities, complications, biomarkers and outcomes were extracted for final evaluation. Twenty-eight articles with missing data on binary outcomes (poor vs non-poor) and elevated biomarkers were excluded. After detailed assessment and considering strict inclusion and exclusion criteria, as of 15 August 2020, we included 32 observational studies with 10 491 confirmed cases of COVID-19 patients detailing laboratory findings and outcomes. Most of the included studies were from China, four were from the USA, one each from Italy, Iran, Korea, Oman and South Korea. Meta-analysis random-effects models quantified the study level impact of different laboratory biomarkers on outcomes in COVID-19 patients.
Complete blood count biomarkers
Lymphocyte count (cells/µL)
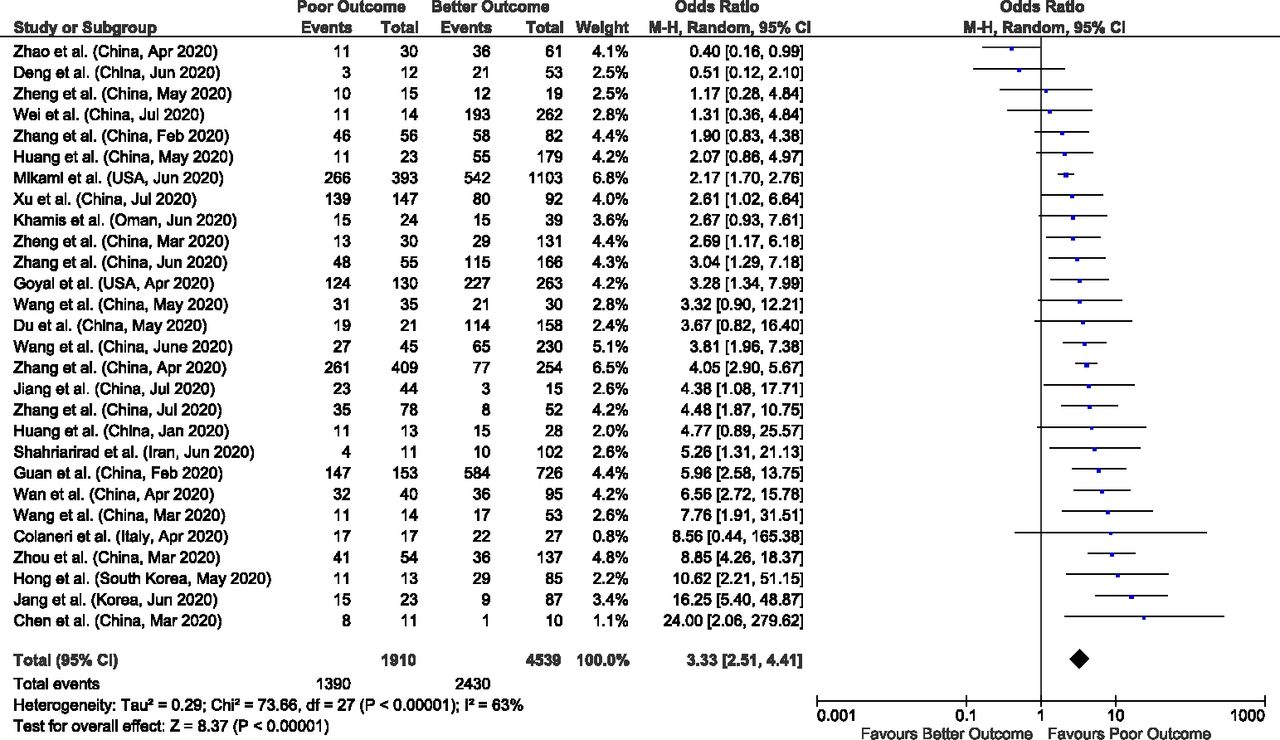
Total of 28 studies reported data on low lymphocyte counts (<1500 lymphocytes/µL) with outcomes giving a total sample size of 6449 COVID-19 patients for evaluation. Meta-analysis of all 28 studies showed that lymphopenia had nearly threefold higher risk of poor outcomes compared with better outcomes (pooled-OR: 3.33; 95% CI: 2.51–4.41; p<0.00001). Significant between study heterogeneity was identified (p=<0.00001; I²=63%). Sensitivity analysis was conducted by eliminating the four outlying studies (Zhao et al, Deng et al, Hong et al and Jang et al) on funnel plot in order to account for heterogeneity. Results after sensitivity analysis also showed significant pooled-OR of 3.47 (95% CI: 2.77–4.36; p<0.00001) with 38% heterogeneity between studies (p=0.03) (figure 2).

Forest plot of lymphopenia for predicting the outcome in COVID-19 hospitalised patients.
Platelet count (cells/µL)
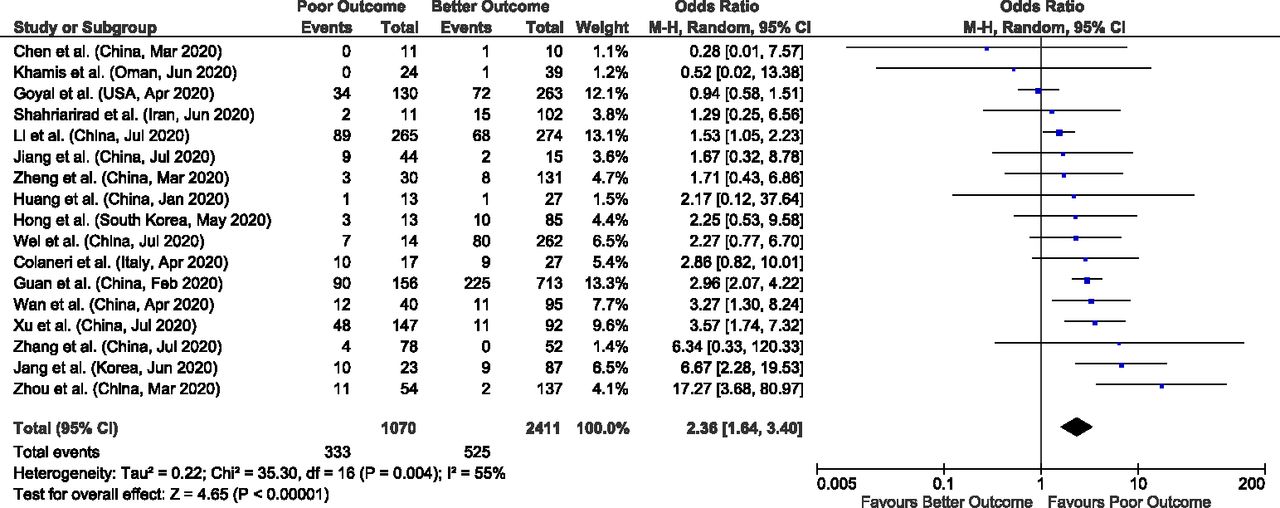
We found 17 studies that provided data concerning low platelet count (<150 000) and its association with poor outcomes. These studies collectively provide a total sample size of 3481 patients for evaluation. Meta-analysis of all 17 studies showed that thrombocytopenia had significant higher odds of poor outcomes compared with better outcomes with a pooled-OR of 2.36 (95% CI: 1.64–3.40; p<0.00001), with a significant between study heterogeneity (p=0.004; I²=55%). We performed a sensitivity analysis by eliminating the two outlying studies (Goyal et al and Zhou et al) on funnel plot in order to account for heterogeneity between the studies. Results after sensitivity analysis also showed significant pooled-OR of 2.42 (95% CI: 1.87–3.13; p<0.00001) with minimal heterogeneity (p=0.32; I²=12%) (figure 3).

Forest plot of thrombocytopenia for predicting the outcome in COVID-19 hospitalised patients.
Inflammatory biomarkers: CRP, PCT and CK
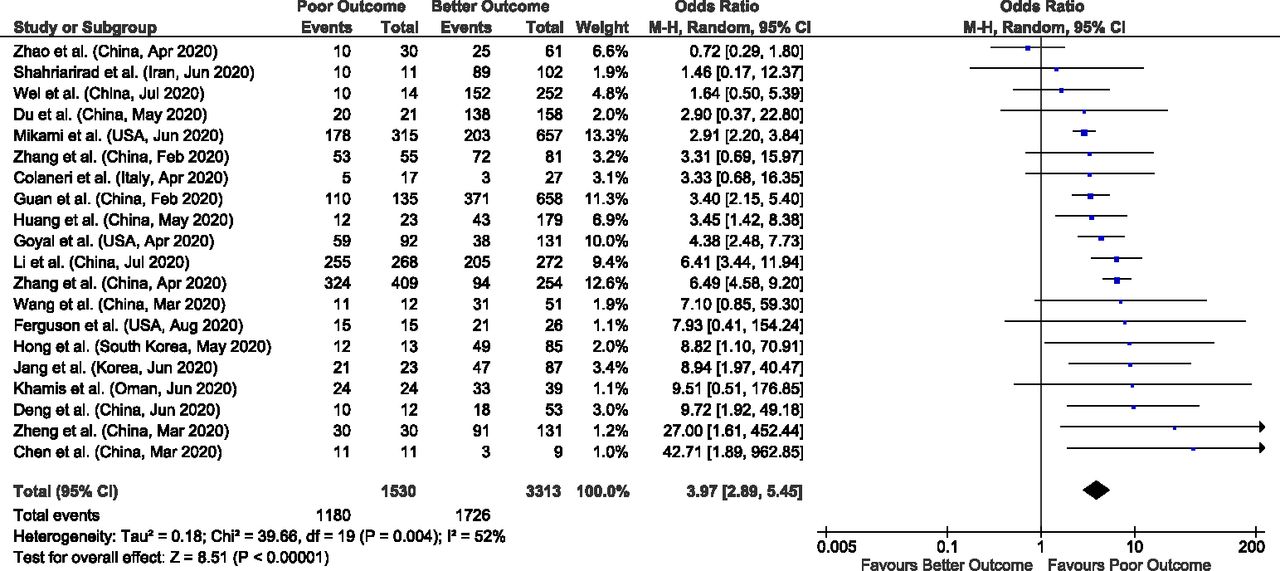
Meta-analysis of 20 studies including 4843 COVID-19 patients, reporting impact of elevated CRP (>10 mg/L) on outcomes showed that there is nearly fourfold higher risk of poor outcomes in COVID-19 patients with elevated CRP (pooled-OR: 3.97; 95% CI: 2.89–5.45; p<0.00001). Significant heterogeneity was found (p=0.004; I²=52%) between studies. After removing one outlying study (Zhao et al) on funnel plot by sensitivity analysis, there was still significant association between elevated CRP and poor outcomes with a pooled-OR of 4.37 (95% CI: 3.37–5.68; p<0.00001) and 31% heterogeneity in the data (p=0.09) (figure 4).
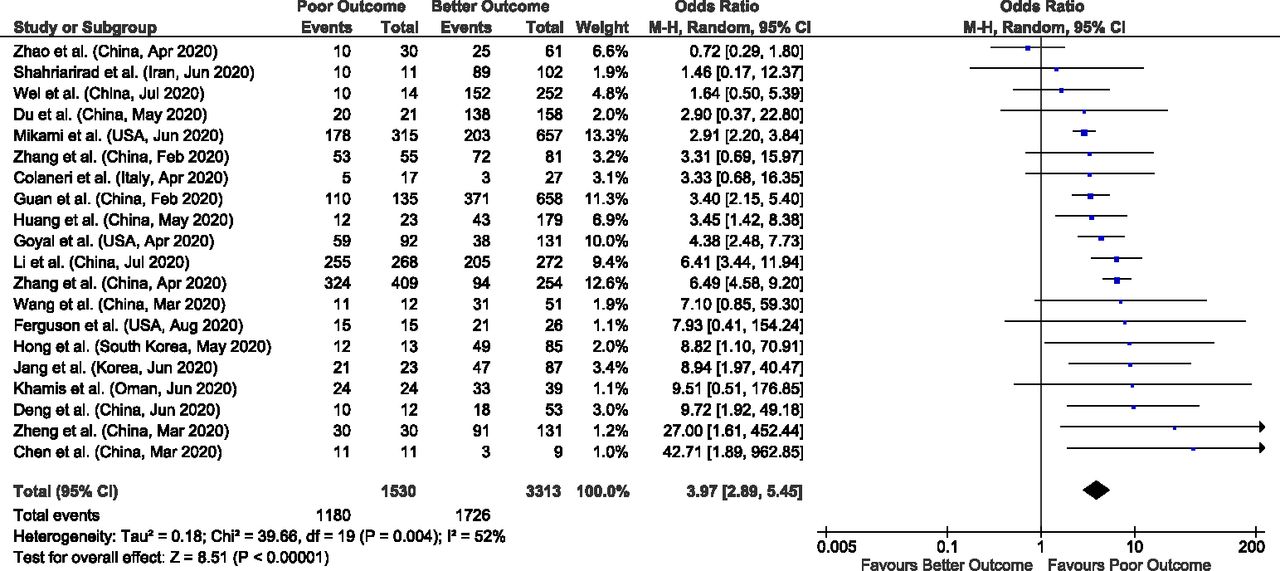
Forest plot of elevated C reactive protein (CRP) for predicting the outcome in COVID-19 hospitalised patients.
In our meta-analysis of 21 studies with reported data on elevated PCT (>0.5 ng/mL) and outcomes including 6031 COVID-19 patients, we found that there is nearly sixfold risk of poor outcomes in COVID-19 patients with elevated PCT (pooled-OR: 6.33; 95% CI: 4.24–9.45; p<0.00001). There was significant heterogeneity (p=0.002; I²=54%) between studies. After removing one outlying study (Goyal et al) on funnel plot by sensitivity analysis, there was still significant association between elevated PCT and poor outcomes with a pooled-OR of 6.99 (95% CI: 4.76–10.27; p<0.00001) and 41% heterogeneity (p=0.03) (figure 5).

Forest plot of elevated procalcitonin for predicting the outcome in COVID-19 hospitalised patients.
We found 12 studies with data on elevated CK and outcomes with a total sample size of 1910 patients for evaluation. Meta-analysis of the all 12 studies showed significant association of elevated CK with outcomes with a pooled-OR of 2.42 (95% CI: 1.35–4.32; p=0.003). Significant between study heterogeneity was identified (p=0.003; I²=61%). We performed a sensitivity analysis by eliminating the one outlying study (Zhou et al) on funnel plot in order to account for heterogeneity among the studies. However, results after sensitivity analysis showed nearly threefold risk of poor outcomes in COVID-19 patient with elevated CK (pooled-OR: 2.87; 95% CI: 1.80–4.57; p<0.00001) with 30% heterogeneity (p=0.16) (figure 6).
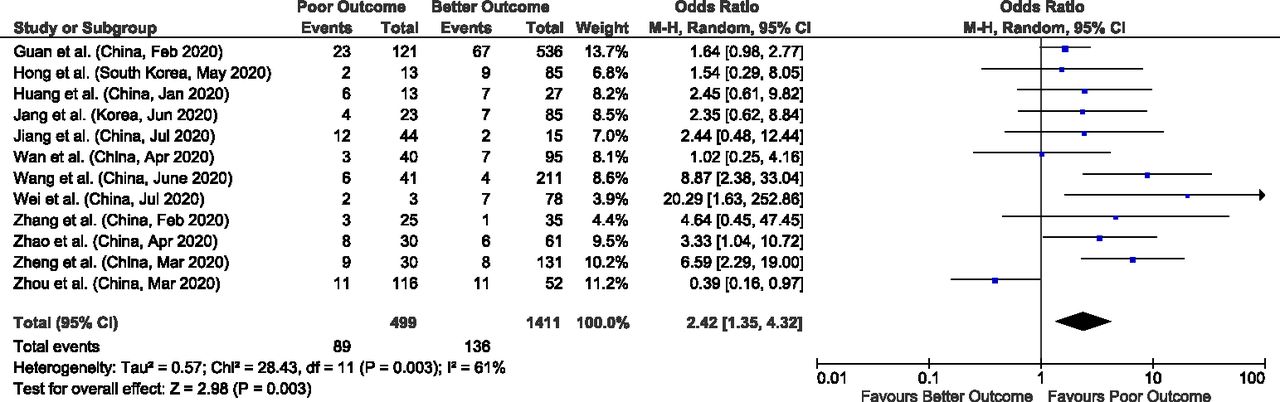
Forest plot of elevated creatine kinase (CK) for predicting the outcome in COVID-19 hospitalised patients.
Comprehensive metabolic panel biomarkers
AST
Out of 32 studies, meta-analysis of 18 studies who have reported data on elevated AST (>40 IU/L) and outcomes giving a total sample size of 6383 patients for evaluation, showed that elevated AST values are associated with nearly threefold more risk of poor outcomes in COVID-19 patients (pooled-OR: 2.75; 95% CI: 2.30–3.29; p<0.00001), with 23% heterogeneity between studies (p=0.18) (figure 7).

Forest plot of elevated aspartate aminotransferase (AST) for predicting the outcome in COVID-19 hospitalised patients.
ALT
Similarly, in 13 studies meta-analysis with reported elevated ALT (>40 IU/L) and outcomes including 6019 patients for evaluation, we found an approximately twofold increased likelihood of poor outcomes (pooled-OR: 1.71; 95% CI: 1.32–2.20; p<0.00001), with 55% heterogeneity between studies (p=0.009). We performed a sensitivity analysis by eliminating the two outlying studies (Deng et al and Jang et al) on funnel plot in order to account for heterogeneity among the studies. However, results after sensitivity analysis showed nearly 1.5-fold risk of poor outcomes in COVID-19 patient with elevated ALT (pooled-OR: 1.49; 95% CI: 1.21–1.82; p<0.0001) with 34% heterogeneity (p=0.12) (figure 8).

Forest plot of elevated alanine aminotransferase (ALT) for predicting the outcome in COVID-19 hospitalised patients.
Creatinine
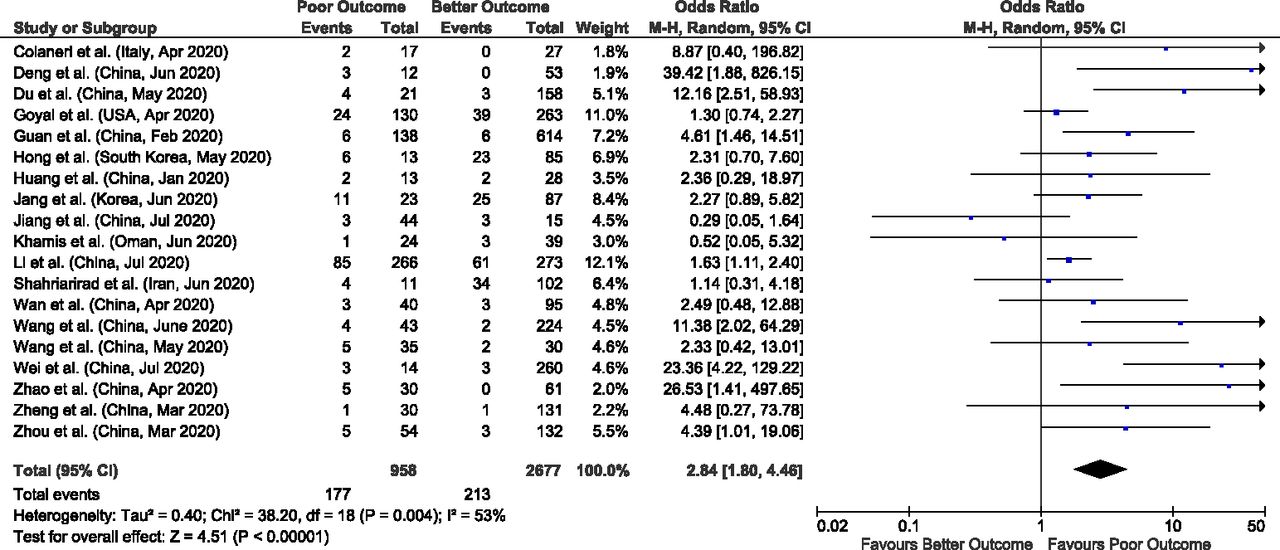
In our meta-analysis of 19 studies including 3635 COVID-19 patients for evaluation, we found that elevated creatinine levels (>1.18–1.5) significantly increase the chance of poor outcomes by nearly threefold compared with better outcomes (pooled-OR: 2.84; 95% CI: 1.80–4.46; p<0.0001), with 53% heterogeneity between studies (p=0.004). We performed a sensitivity analysis by eliminating the two outlying studies (Wei et al and Jiang et al) on funnel plot in order to account for heterogeneity among the studies. However, results after sensitivity analysis showed nearly 2.6-fold risk of poor outcomes in COVID-19 patient with elevated creatinine (pooled-OR: 2.64; 95% CI: 1.76–3.94; p<0.00001) with 37% heterogeneity (p=0.06) (figure 9).

Forest plot of elevated creatinine for predicting the outcome in COVID-19 hospitalised patients.
Other biomarkers
D-dimer
Out of 32 studies, 16 reported data on elevated D-dimer (≥0.5 mg/L), giving a total sample size of 4862 patients for evaluation. In meta-analysis of all 16 studies, we found that elevated D-dimer values are associated with nearly threefold higher risk of poor outcomes in COVID-19 patients (pooled-OR: 3.39; 95% CI: 2.66–4.33; p<0.00001). Significant between study heterogeneity was identified (p=0.04; I²=42%). In order to account for heterogeneity, sensitivity analysis was performed by eliminating the one outlying study (Jang et al) on funnel plot but still found a significant pooled-OR of 3.17 (95% CI: 2.57 –3.91; p<0.00001) with 26% heterogeneity in the data (p=0.17) (figure 10).

Forest plot of elevated D-dimer for predicting the outcome in COVID-19 hospitalised patients.
LDH
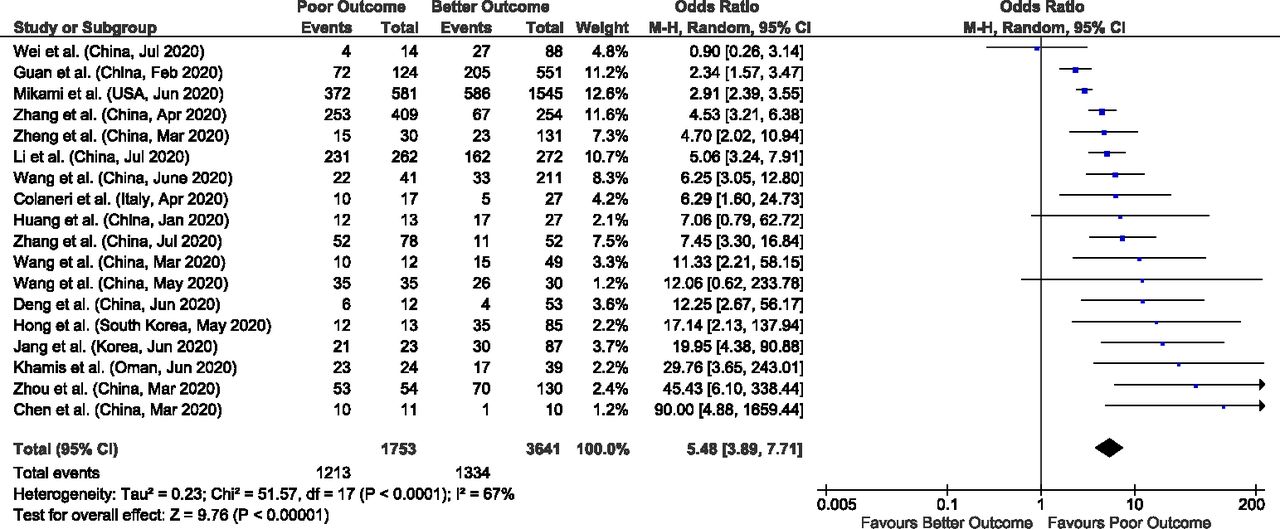
Out of 32 studies, meta-analysis of 18 studies with a total sample size of 5394 patients for evaluation, showed that in COVID-19 patients, elevated LDH values are associated with approximately fivefold more risk of poor outcomes (pooled-OR: 5.48; 95% CI: 3.89–7.71; p<0.00001), with significant heterogeneity between studies (p<0.0001; I²=67%). A sensitivity analysis was performed by eliminating the four outlying studies (Guan et al, Mikami et al, Zhou et al and Chen et al) on funnel plot in order to account for heterogeneity between studies. The results after sensitivity analysis also showed nearly sixfold risk of poor outcomes in COVID-19 patient with elevated LDH (pooled-OR: 5.84; 95% CI: 4.25–8.04; p<0.00001) with 31% heterogeneity (p=0.13) (figure 11).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of elevated lactate dehydrogenase (LDH) for predicting the outcome in COVID-19 hospitalised patients
Discussion
In our meta-analysis of 32 studies reflective of 10 491 confirmed COVID-19 patients, we found that specific biomarkers were associated with poor outcomes in COVID-19 hospitalised patients. These specific biomarkers included a decreased lymphocyte count, a decreased platelet count and elevated CRP, CK, PCT, D-dimer, LDH, ALT, AST and creatinine.
The COVID-19 pandemic is rapidly spreading and increasing the healthcare burden worldwide. The variable course of illness ranging from asymptomatic to severely ill with complications of acute respiratory failure makes it crucial to collect strong evidence to determine the patient’s condition in a timely manner and predict complications. Biomarkers are quantitative measurements that reflect the pathophysiology of disease and thus help clinicians in recognising the severity of medical illness. They also aid in the development of clinical care management algorithms that have the potential to improve patient outcomes. These laboratory indices will be helpful in differentiating severely ill patients and allow for the appropriate allocation of healthcare resources. The use of these biomarkers in understanding COVID-19 may also help to prevent virus-induced acute inflammatory response complications such as acute hypoxemic respiratory failure and multiorgan dysfunction including acute cardiac, hepatic and renal injury in affected patients. The main pathologic changes reported so far in COVID-19 are immune system damage and lung infection. In our meta-analysis, 28/32 studies reported the data on lymphopenia, and it appears to be the most frequently described prognostic biomarker in COVID-19 followed by PCT (21/32 studies) and CRP (20/32 studies).
Lymphocytes play a key role in maintaining immune homeostasis and inflammatory response to protect the body against viral infections.20 The majority of the studies included in this meta-analysis have suggested that one of the typical characteristics of SARS-CoV-2 infection is a decreased number of lymphocytes, which in turn was significantly associated with poor outcomes.21 These findings are consistent with other studies.22–24 One hypothesis is that lymphocytes express SARS-CoV-2 receptor ACE2 and hence are directly attacked and consumed by the virus.25 Another theory is the elevated level of proinflammatory cytokines such as tumour necrosis factor (TNF)-α and IL-6 in COVID-19 patients results in lymphocyte-induced apoptosis.26 Therefore, lymphopenia inhibits the body’s innate immune system leading to exacerbations of COVID-19 patients and poor outcomes.
Another crucial biomarker is PCT which may play a useful role in predicting the evolution towards the more severe form of the COVID-19 disease. PCT is often used as a biomarker of systemic bacterial infection and its levels do not usually change in viral infections.27 A meta-analysis of four studies by Lippi et al 28 showed that elevated PCT is associated with fivefold more risk of severe SARS-CoV-2 infection, these findings are consistent with our meta-analysis of 21 studies. In a non-complicated COVID-19 infection, the PCT may remain in normal limits but a continuous increase in PCT levels may indicate a bacterial coinfection and progression towards more severe complications such as COVID-19 pneumonia and acute respiratory distress syndrome (ARDS). A possible explanation for this finding is that the synthesis of PCT is decreased by an increased production of interferon-γ during viral infection; however, there is a surge in PCT production and release during bacterial infections which is enhanced by IL-1β, TNF-α and IL-6.29 Additionally, it is suggested that both PCT and CRP correlate with disease severity in ARDS patients.29 However, this does not hold true for either biomarker independently. Additionally, PCT levels are significantly higher in ARDS patients with sepsis making it useful in early identification of such patients and aid in treatment.29
CRP is a non-specific acute phase reactant induced by IL-6 in the liver. Clinically, it is used as a biomarker for different inflammatory and infectious conditions. Elevated CRP levels are directly correlated with level of inflammation and disease severity. Hence, it is an important biomarker in diagnosis and assessing the severity of infectious diseases.29 Our meta-analysis findings are consistent with other small cohort studies that positively associate elevated CRP levels with disease severity30–32 and formation of lung lesions in the early stages of COVID-19. Hence, suggesting that CRP can be the most effective and sensitive biomarker in predicting the COVID-19 disease progression.
Our study found that elevated D-dimer levels are associated with an increase in the risk of poor outcomes by threefold in COVID-19 patients. The increased inflammatory response in COVID-19 and hypoxia due to severe pneumonia, eventually leads to the activation of coagulation and fibrinolysis, followed by a hypercoagulable state causing DIC, and multi organ dysfunction.33 34 Additionally, prior studies show that D-dimer levels greater than 2.0 µg/mL on admission could effectively predict in-hospital mortality rates of patients with COVID-19.35 Patients with higher D-dimer levels requiring intubation were also associated with a greater probability of developing a pulmonary embolism after admission. A study by Yu et al found significantly elevated levels of D-dimer in COVID-19 patients than patients with community acquired pneumonia.36 The study also found that elevated D-dimer was related with markers of inflammation, especially with CRP. In this study, treatment with anticoagulants led to a decrease in D-dimer and CRP levels in patients with good clinical prognosis.36 In our meta-analysis, we found that elevated D-dimer values are associated with a higher risk of poor outcomes and that COVID-19 patients manifest higher CRP levels. This suggests that use of anticoagulants and anti-inflammatories could lead to a decrease in poor outcomes in COVID-19 patients.36
AST and ALT are released in the setting of hepatocyte damage which leads to increased serum levels (abnormal liver function). Studies have shown that COVID-19 only transiently increases levels of AST and ALT and have elaborated that the mechanism through which liver dysfunction occurs is most likely through secondary liver damage rather than a direct insult. This secondary damage is caused by several factors, most importantly the systemic inflammatory response, observed in this disease, and the use of hepatotoxic drugs in the management of COVID-19 patients. The occurrence of multiple organ failure is believed to be mediated by the sudden initiation of an ‘inflammatory storm’ that activates both natural and cellular immunity in critically ill COVID-19 patients.37 Additionally, hypoxia seen in COVID-19 patients could lead to hepatocellular necrosis through the marked increase in reactive oxygen species which act to activate redox-specific transcription factors that amplify the release of hepatotoxic proinflammatory factors.38 39 The progression of liver injury was also found to be exacerbated by the use of certain antiviral medications such as lopinavir and ritonavir during hospitalisation.40 According to initial studies, more than one-third of patients had elevated AST and ALT which was associated with longer hospital stay.41–43 In a study done by Cai et al,40 of the 417 patients with COVID-19, 76.3% had abnormal liver tests while 21.5% developed liver injury during hospitalisation, which was defined by ALT, AST, total bilirubin and gamma-glutamyl transferase levels elevated to more than three times the upper limit of normal. The study found that patients with abnormal liver tests had significantly higher odds of developing severe pneumonia.40 This is consistent with our study that shows a significant increase in AST and ALT among COVID-19 patients and the potential for these biomarkers to signify poor outcomes among these patients.
LDH is present in tissues throughout the body and is involved in the interconversion between pyruvate and lactate through an nicotinamide adenine dinucleotide (NADH)-dependent reaction. Abnormal LDH levels can result from decreased oxygenation, leading to an upregulation of the glycolytic pathway and from multiple organ injury. The mechanism through which lactate leads to injury is via the action of metalloproteinases and enhanced macrophage-mediated angiogenesis.44 In a study conducted on COVID-19 patients, it was found that levels of LDH early on in the course of the disease can be a good predictor of lung injury and severe COVID-19 cases.45 High LDH has also been associated with worse outcomes in several studies.46–48 In a pooled analysis, elevated LDH values were associated with a >16-fold increase in odds of mortality and a sixfold increased odds of severe disease.44 Our overall results also demonstrate the odds of having higher LDH in patients with poor outcomes compared with better outcomes.
CK is an enzyme found in many tissues throughout the body such as the heart, brain and skeletal muscle. Elevated CK in the blood serves as a marker for muscle damage. A case report on two COVID-19 patients has shown that an elevated CK level can be the sole initial presentation of patients with COVID-19.49 This acute increase in CK can also be seen in the context of rhabdomyolysis. The mechanism through which this viral-induced myositis occurs is not well understood, however, cases have reported that viral mediated muscle invasion may damage myocytes and that the process can also be mediated by the immune system.50 Immune-mediated damage can be explained through the deposition of virus–antibody complexes in muscles, circulating viral toxins in the blood, immunologic cross-reactivity and virus-induced expression of antigens on the cell membrane.50 Our study found a nearly fourfold increase in poor outcomes in patients with elevated CK. This suggests that CK level monitoring is a vital factor in monitoring the clinical progression of COVID-19.
Creatinine is a marker for kidney function. In a prospective cohort study done in 701 COVID-19 patients, it was found that during hospitalisation, the incidence of acute kidney injury and death was significantly higher in patients with elevated baseline serum creatinine levels than in patients with normal baseline values.51 The mechanism by which this takes place is speculated to be through hematogenous spread and accumulation of the virus in the kidney, causing renal cell necrosis.51 Our study found that elevated creatinine levels increase the chance of poor outcomes by nearly twofold.
Strengths, limitations and future directions
The main limitation of this meta-analysis is the heterogeneity of the included studies. All the studies are retrospective studies due to the lack of data from prospective studies and randomised trials. Furthermore, the different definitions of the severity of the COVID-19 disease and discrepancy in the cut-off values for the biomarkers might be explanations for the heterogeneity. Another limitation is that we did not have data on the changing levels of the biomarkers during the disease course, which is significant to predict the clinical course of the COVID-19. Due to the expeditious increase in COVID-19 cases globally, waiting for prospective study results will delay our understanding and clinical management of patients infected with SARS-CoV-2. Despite these limitations, our meta-analysis of 10 491 confirmed COVID-19 patients suggests that alterations in laboratory biomarkers including lymphopenia, thrombocytopenia and elevated CRP, D-dimer, PCT, LDH, CK, AST, ALT and creatinine play a significant role in the progression of COVID-19. These markers may help in early triage of high-risk patients and prevent the complications associated with poor outcomes. However, unavailability of sensitivity, specificity and accuracy of these biomarkers in predicting outcomes are other limitations.52 Most of our study findings are consistent with meta-analysis published by Henry et al, which included articles until 17 March 202053 and review articles by Ponti et al and Kermali et al, which described the role of haematological, inflammatory and other special biomarkers role in the progression of the disease.54 55 Hence, our study findings have added to the existing knowledge of biomarkers usefulness for risk stratification model that may serve as predictors of severe COVID-19. Future studies should focus on the timeline of the changes in levels of biomarkers and then severity of the COVID-19 disease and its associated complications.
Conclusion
Our meta-analysis suggests that laboratory biomarkers including lymphopenia, thrombocytopenia and elevated CRP, PCT, D-dimer, CK, LDH, AST, ALT and creatinine are significantly associated with poor outcomes in COVID-19 patients. Our study results may be used as helpful biomarker in the early management of the high-risk COVID-19 patients and potentially improve prognosis and mortality rates. Furthermore, these biomarkers may be helpful in developing prevention policies and responses to combat critical adverse COVID-19 outcomes.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Data are collected from the studies published online, publicly available, and specific details related to data and/or analysis will be made available upon request.
Ethics statements
Ethics approval
Though this article does not contain any studies with direct involvement of human participants or animals performed by any of the authors, all procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
References
Footnotes
Contributors PM and UP contributed to conceptualisation and methodology. PM and DM contributed to acquisition of data, PM contributed to formal analysis and investigation. PM, UP, DM, NP, RK and MA contributed to writing-original draft preparation. JLG and HS contributed to writing-review, critical feedback and editing. HS contributed to supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.