Article Text

Abstract
Background: Although repetitive exposure to stressful situations is thought to habituate the physical stress responses, work stress is experienced by medical personnel in emergency and intensive care units; performance should, however, remain stable over time.
Aims: To investigate the neuroendocrine reactions (reactivity during and recovery after work) in experienced emergency caregivers during emergency situations.
Methods: A within subjects pre-post design was studied in the natural work environment of 20 municipal Dutch emergency caregivers. A stress protocol was developed in which the biomarker cortisol was measured in saliva at baseline, during the emergency period, and during recovery. Four scenarios were tested between subjects in which the severity of the emergency situation and the time of day were taken into account.
Results: Greater endocrine reactions were shown during and after the handling of patients in direct life threatening situations during morning hours compared to the handling of patients who were not in direct life threatening situations.
- work stress
- emergency unit
- paramedic personnel
- cortisol
- recovery
Statistics from Altmetric.com
Work and work related changes in health and wellbeing of both doctors and nurses have become the subject of growing concern in recent years. The long term effects of work stress and the higher incidences of burnout of medical staff in emergency and intensive care units compared to other units have been subject of research (for example, Ferrari et al1). Part of the problem could be the denial of the effect of stress and fatigue (time of day) on own performance by medical staff, as shown by Sexton and colleagues.2 In addition, repetitive exposure to episodes of emotional stressors (such as the struggle between life and death in the emergency room) is thought to participate in tissue damage through overproduction of stress hormones or the lack of shutting off these responses.3–5
Main messages
-
A lack of recovery in cortisol values is found after handling patients in direct life threatening situations.
-
Experience in stressful work does not result in optimal neuroendocrine coping.
-
The acute stress protocol that is used as method for stress research in laboratory settings is also a useful tool for research in natural work situations.
Policy implications
-
Health care workers who encounter patients in acute life threatening situations should be allowed a break after every encounter to encourage full neuroendocrine recovery.
Most studies have focused on subjective experiences, although some publications have assessed the magnitude of the stress response in the natural work environment.6 Although the magnitude of the endocrine reaction has been defined, information about the severity of the stressful context, time of day, and duration of physiological reactivity is lacking.
The aims of this study, therefore, are: (1) to assess cortisol reactivity during and after handling patients in emergency situations; and (2) to differentiate outcomes by severity of patients and time of day.
METHODS
Over a period of three months, 20 Dutch, male ambulance paramedics (average 42 years of age (SD 5) and 16 years of experience in the job (SD 7)) were observed and monitored during their work in Amsterdam after written informed consent was obtained. Salivary cortisol measurements during and after emergency calls were monitored for each subject on at least one working day. The acute stress protocol that is used as method in most stress research in laboratory settings was applied: sampling of the baseline values of salivary cortisol concentrations took place at the moment of the incoming emergency call (baseline), followed by repeated sampling immediately after delivery of the patient to the hospital (post 0), and two recovery samples at 15 and 30 minutes after delivery (post 15 and post 30, respectively). Protocols were taken into account only when no other tasks were asked for during recovery or, more precisely, during the period between the post 0 and post 30 samples. Post hoc, protocols were labelled “severe” if resuscitation took place or if the patient’s life was threatened acutely by acute heart failure, accidents, shootings, or stabbings. Time of day at which the whole protocol took place was registered; for the outcome measure cortisol was labelled as “circadian high” between 4 and 10 am and as “circadian low” outside this time frame. The above mentioned categorisation revealed four between-subjects scenarios.
Salivary cortisol was analysed with a time resolved fluorescence immunoassay, in which a stable cortisol-biotin conjugate was used in combination with rabbit cortisol antibodies for assessment of cortisol concentrations. The lower detection limit was 0.1 nmol/l. Intra- and inter-assay variability were <10% and <12%, respectively. Endocrine reactions were defined following Fischer and colleagues6 as reactions of a minimum 2.5 nmol/l cortisol above baseline values.
After testing differences in mean baseline cortisol excretion between the four described scenarios: (1) mean endocrine reaction per scenario was described; and (2) a between subjects multivariate analyses of variance was performed with cortisol excretion as dependent variables and the two factors (severity and time of day) as independent variables.
RESULTS
In total, 54 emergency protocols were monitored, time framed, and labelled as severe or not severe. Because of intervening tasks for the subjects during the recovery time of the protocol, 21 protocols were interrupted and could not be included for analysis. Of the remaining 33 protocols, 16 were categorised as the scenario of “not severe and during the circadian low period”, five as “not severe and during circadian high period”, seven as “severe and during the circadian high period”, and five as “severe and during the circadian low period”. In total, results include data from 17 of the 20 subjects.
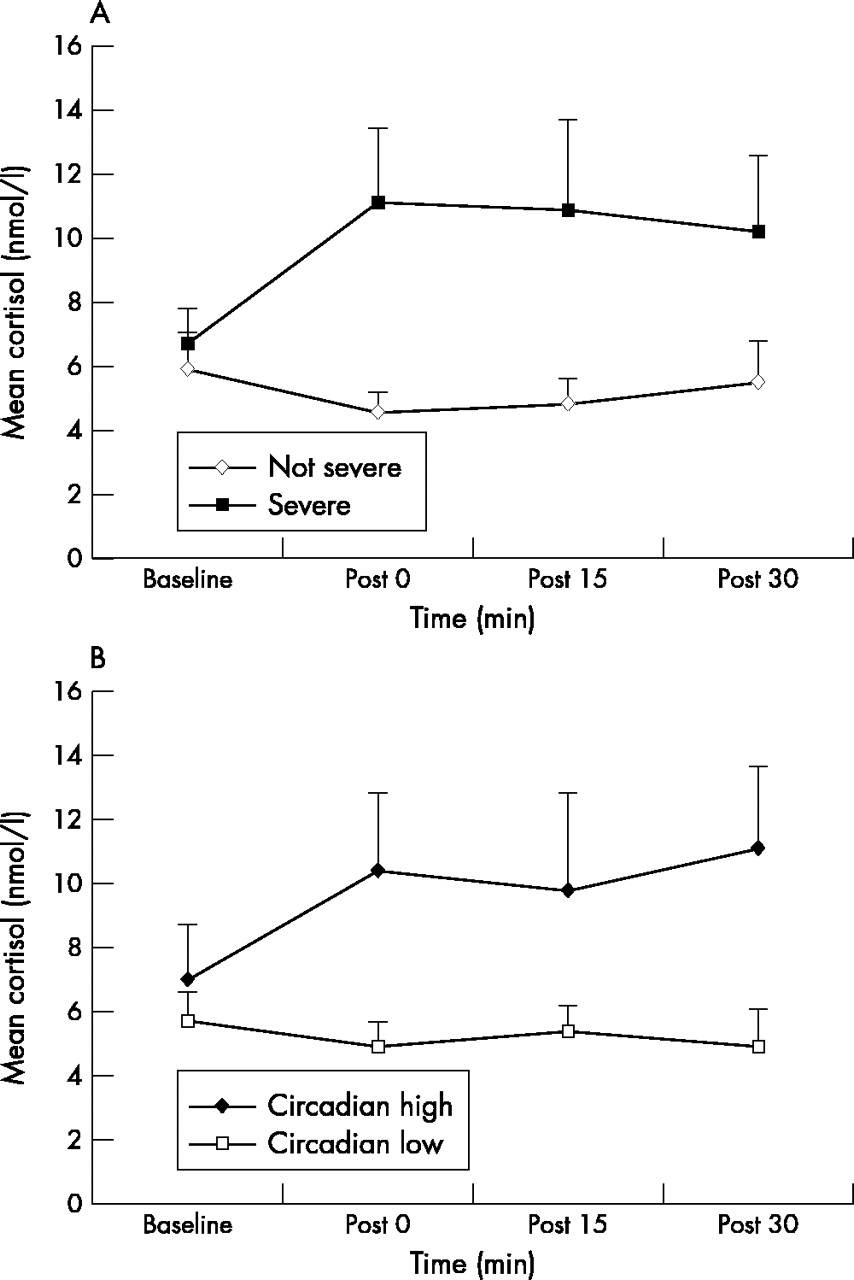
At baseline, no significant differences in cortisol excretion between the four scenarios were found. Both severity of patients (fig 1A) and time of day (fig 1B) showed significant effects in reactivity (post 0: p = 0.00 and p=0.01, respectively) and recovery (post 15: p = 0.02 and p = 0.09, respectively; post 30: p = 0.07 and p = 0.01, respectively). Endocrine reactions6 compared to baseline occurred during treatment of the severe patients (post 0: mean reaction = 4.4 nmol/l) and continued during recovery (post 15: mean reaction = 4.1 nmol/l; post 30: mean reaction = 3.4 nmol/l). No endocrine reactions were observed on average during or after non-severe emergencies, irrespective of time of day.

{kind=link}
Cortisol reactivity (nmol/l) during handling of patients in emergency situations (n = 33) and during recovery in ambulance workers. (A) Severe v non-severe patients. (B) Circadian influence of peak time (circadian high) v outside peak time (circadian low).
When severe emergency periods occurred during circadian high periods, endocrine reactions occurred immediately after termination of the emergency period (post 0: mean reaction = 6.8 nmol/l), and still continued during recovery (post 15: mean reaction = 7.4 nmol/l; post 30: mean reaction = 6.6 nmol/l).
DISCUSSION AND CONCLUSIONS
The results of this study showed that the severity of the patient and time of day are predictors of neuroendocrine reactions and lack of recovery in experienced medical staff. During (reactivity) and after (lack of recovery) severe emergency situations, and mainly during morning hours, endocrine reactions in cortisol excretion were found.
The fact that the measurements were taken in the natural work environment was the main cause of the interruption of about one third of the original observed emergency periods because in these cases, continuing intervening tasks were asked for during the “experimental recovery time”.
Fischer and colleagues6 showed that job experience had a protective effect on the magnitude of the physiological response during stressful situations in acute medical care. With this finding in mind plus the aforementioned knowledge about ongoing tasks, the present results might be even more worrying for less experienced staff.
From the present study a suggestion could be to plan more flexible breaks for medical staff with comparable tasks by allowing some mental rest for endocrine recovery after treatment of patients in acute life threatening situations during the morning hours.
Because cortisol is seen as one of the important biomarkers for allostatic load,3 physicians and paramedics should understand that repeated exerted efforts towards patients in high emergency situations might influence the risk of developing adverse health reactions in the future.
Acknowledgments
This project was mainly funded by The Netherlands Organization of Scientific Research (NWO-PVA). The samples were analysed in the Centre for Psychobiological and Psychosomatic Research of Trier, Germany in the laboratory of Prof. Clemens Kirschbaum.
J Sluiter, M Frings-Dresen, and A van der Beek were executive of or responsible for the project. J Sluiter wrote the first draft, which was read, supplemented, and approved by the other two authors.
REFERENCES
COMMENTARY
The main finding is that male ambulance paramedics have a higher salivary cortisol response to severe situations than to not so severe situations. This is not surprising, but it is shown in an elegant and professional way. The conclusions, however, are controversial.
The paramedics have a high level of cortisol 30 minutes after the severe events. This is characterised as a “lack of recovery”; it is assumed that this is not “optimal neuroendocrine coping”, and changes in routines are suggested. Why? I would be more worried for patients, and for the paramedics, if they did not react to severe emergencies with arousal. Also, I would not be worried if this arousal lasts for 30 minutes. We are barely into the half life of plasma (and salivary) cortisol.
To the best of my knowledge, there are no hard data suggesting pathophysiological consequences of being awake, even wide awake, for hours on end. To refer to this as “stress” is just confusing and suggests relations that are not proven. However, feedback to the paramedics based on these interpretations may lead to constant worries. These are not based on facts, but may have potential after-effects. Only when the aftermath interferes with the restitution over the whole 24 hour period, potential health effects may occur, as shown elegantly in Sluiter’s previous work.1,2
The authors interpret their findings as a lack of “habituation”. The habituation term should perhaps be restricted to the abolishment of the orienting response to a non-signal stimulus. However, they refer to the fact that arousal persists even if the paramedics have been exposed to similar situations before. From coping theory one might expect at least a reduction in the response with increasing experience, and increasing trust in one’s skill in handling these emergencies. The data do not allow conclusions on this. It seems reasonable to assume that such a reduction may have occurred, but the arousal does not reduce to zero. This would be incompatible with the high performance and the handling of strong emotions involved in medical emergency care.
AUTHORS’ REPLY
WIDE OR QUITE AWAKE IS NOT THE PROBLEM …
We agree completely with Ursin that part of the neurophysiological response of paramedics to severe emergencies could be defined as arousal (although we did not use this label). In addition, we agree that “activity” or, more precisely, multiple energetic mechanisms are responsible for acute adaptation to the changing environment and these reactions might be expected to be found during work in these and every worker. However, we believe that this “extra” arousal that Ursin is referring to (on top of the expected circadian level of activity because workers generally are “quite awake” during working time) would be shown as adrenaline or noradrenaline excretions and not necessarily as extra cortisol excretion. This differential hormonal reactivity pattern between the catecholamines and hormones of the hypothalamo-pituitary-adrenocortical axis has been shown in several worker studies.
Secondly, the conclusions of our study do not mention any “perils”or other consequences of being wide awake. Our concerns with repeated rises in acute cortisol excretion in these workers is based on the increased risk for adverse long term health consequences of these paramedics when their goal is to keep on working in the same jobs for another 20 years. Cortisol is seen as the biomarker of stress reactions and one of the biomarkers of allostatic load. Studies testing the allostatic load theory of McEwen, Seeman, and colleagues confirm that chronic health consequences occur through repeated ups and downs of physiological responses that impact on the wear and tear of a number of organs and tissues and can predispose the organism to disease.1,2
Thirdly, the reason why Ursin believes that we interpreted our findings in terms of “lack of habituation” is unclear because no such statements were made in the article.
Finally, Ursin’s last argument is that nothing could be said about coping from these data. Healthy coping in terms of Ursin’s (and Eriksen’s) own cognitive activation theory of stress suggests that positive expectancy outcomes take place in the paramedic’s mind at the moment that the emergency call comes in (at baseline) because these workers are experienced and skilled in the task at hand. What might be expected, however, is that this “healthy coping” does coincide with more mental effort to prepare ongoing events and, therefore, will result in increased activity levels (which will mainly be shown through reactivity of catecholamines) but will not result in any rise of cortisol levels. It was not possible for the paramedics under study to predict the severity of these patients at baseline when the emergency bell rung, and data on the non-severe emergencies did show that the emergency call per se did not initiate a stress (cortisol) reaction after 20 minutes (the second measurement). Specifically, given the fact that coping is mostly better among experienced workers, such as the ones studied, compared to novice or less experienced workers, we did expres our concerns regarding cortisol reactivity in less experienced staff.
Footnotes
-
This project was partly funded by Netherlands Organisation of Scientific Research (NWO), Netherlands