Article Text

Abstract
Aim: Airway management is a core aspect of emergency medicine. The technique of rapid sequence intubation (RSI) creates continuing debate between anaesthetists and emergency physicians in the UK, although similar complication rates for emergency department (ED) RSI have been shown for both specialties. This study examined prospectively collected data on every ED RSI performed in a university hospital in Glasgow over 5 years.
Methods: Data were prospectively recorded for every attempted RSI in the ED on a dedicated form (as used in previous studies) between January 1999 and December 2003. Immediate complications were specifically sought in the questionnaire, as was the immediate destination on leaving the ED. The χ2 test was used for categorical data.
Results: On average, 51 ED RSI were performed annually (range 42–60). Emergency physician RSI for trauma increased from 32% (7/22) in 1999 to 75% (21/28) in 2003 (χ2 = 9.32, df = 1, p = 0.002) and for non-trauma from 62% (18/29) in 1999 to 79% (23/29) in 2003 (χ2 = 2.08, df = 1, p = 0.15). Complication rates for emergency physician RSI decreased from 43% (3/7) to 14% (3/21) for trauma (χ2 = 2.55, df = 1, p = 0.11) and from 28% (5/18) to 4% (1/23) for non-trauma (χ2 = 4.44, df = 1, p = 0.035). This compares with mean complication rates for anaesthetists for trauma of 17% and for non-trauma of 22%. Incidence of hypotension decreased in all groups; however, oxygen desaturation is now the most common complication. The rate of ED RSI prior to computed tomography (CT) scans increased in both the trauma (79% v 42%; χ2 = 7.42, df = 1, p = 0.0065) and non-trauma (48% v 17%; χ2 = 5.85, df = 1, p = 0.016) groups.
Conclusion: Emergency physician performed ED RSI is increasingly common but is not associated with overall higher numbers of RSIs being performed in the ED. Effective pre-oxygenation should be emphasised during training.
- ED, emergency department
- RSI, rapid sequence intubation
- rapid sequence intubation
- emergency physician
- anaesthesia
- intensive care
- complication
Statistics from Altmetric.com
Rapid sequence intubation (RSI) is a continuing source of debate between anaesthetists and emergency physicians. The debate has primarily focused on success and complication rates and the possibility that emergency physician RSI will increase the numbers of inappropriate intubations.1–3 Previous studies have shown that similar complication rates for RSI are seen in both specialties.2,4
No previous UK study has examined trends in the practice of RSI in the emergency department (ED) over an extended period of time. This study examines prospectively collected data on every RSI performed in the ED of a single teaching hospital in Glasgow over 5 years to identify trends and to determine how ED RSI has evolved in this centre during that time.
METHODS
The study was undertaken in an ED seeing 45 000 new patients annually. Data were prospectively recorded for every attempted RSI in the ED on a dedicated proforma identical to that used in previous studies.2,4 Data were collected between January 1999 and December 2003. The questionnaire specifically sought to identify immediate complications resulting from the procedure, and the patient’s immediate destination on leaving the ED. RSI in the ED was strictly defined as given previously.2,4 Regular checks were made to ensure that no intubation attempt had been overlooked; during the daily handover meeting, all intubations were identified and the duty consultant ensured that data forms had been completed for each intubation. Data were entered onto a Microsoft Excel spreadsheet for analysis.
RESULTS
Annually, a mean of 51 ED RSIs were performed (range 42–60). Emergency physician RSI for trauma increased from 32% (7/22) in 1999 to 75% (21/28) in 2003 (χ2 = 9.32, df = 1, p = 0.002) and for non-trauma from 62% (18/29) in 1999 to 79% (23/29) in 2003 (χ2 = 2.08, df = 1, p = 0.15) (fig 1).

{kind=link}
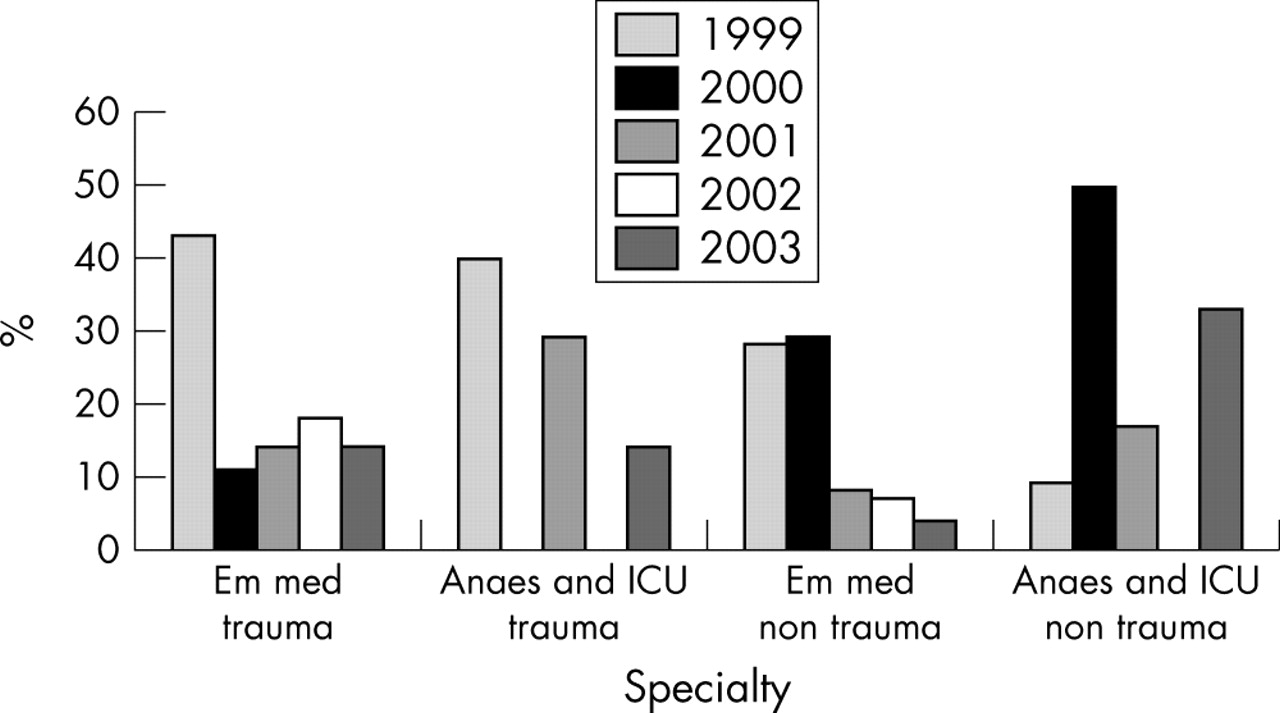
Percentage complications by year and specialty.
Complication rates (defined as number of patients with one or more complications, not individual complications) for emergency physician RSI decreased from 43% (3/7) to 14% (3/21) for trauma (χ2 = 2.55, df = 1, p = 0.11) and from 28% (5/18) to 4% (1/23) for non-trauma (χ2 = 4.44, df = 1, p = 0.035). This compares with overall complication rates for anaesthetists for trauma RSI of 18% (6/34) and for non-trauma RSI of 22% (9/41), with no obvious trends in the patterns of complications noted. Complications varied between trauma (oesophageal intubation) and non-trauma (cardiac arrest and vomiting).
The incidence of hypotension decreased in all groups; however, the incidence of oxygen desaturation is high and is now the commonest complication. The majority of desaturations occurred in patients intubated by emergency physicians.
The rate of ED RSI prior to computed tomography (CT) scans increased in both the trauma (79% v 42%; χ2 = 7.42, df = 1, p = 0.0065) and non-trauma (48% v 17%; χ2 = 5.85, df = 1, p = 0.016) groups. There was no observed increase in the proportion of direct admissions from the ED to the intensive care unit.
DISCUSSION
Over time, the observed complication rate for emergency physician performed RSI in the ED decreased.
The finding of oxygen desaturation as the commonest complication for emergency physicians suggests that greater emphasis should be put on formal pre-oxygenation as an essential part of RSI. It may also reflect the decreased oxygen reserve in critically ill patients who need immediate intubation by emergency medicine staff. However, a short period of preoxygenation (ventilation with high flow oxygen via a bag valve mask device or Mapleson C circuit while drugs are drawn up and preparations are made for intubation) may improve oxygenation and decrease the incidence of this complication.
Our results suggest that higher proportions of patients are being intubated prior to CT scan. Skills in intra-hospital transfer for emergency physicians (for example, to the CT room) are likely to be required if this trend is repeated in other centres.
It is reassuring to note that the absolute number of patients requiring RSI has not increased despite the increased involvement of emergency physicians. The continuing involvement of senior emergency medicine, anaesthesia, and intensive care specialists is likely to be the main factor behind this, as it suggests that few ED patients are inappropriately subjected to RSI. The higher complication rate for anaesthesia staff is likely to reflect the fact that most difficult airways are triaged to anaesthetists and intensive care specialists rather than emergency physicians.
The study is limited by the honesty of the person completing the form. It is possible that a few cases may have been missed but this is unlikely to have significantly affected the results.
The applicability of this study is limited to centres in the UK with emergency physicians who are committed to providing an advanced airway service in close collaboration and with the support of anaesthetic and intensive care medicine colleagues. We acknowledge that not every ED in the UK will fulfil these criteria and this may limit the applicability of our results.
In conclusion, complication rates for emergency physician performed RSI have improved over time. The lack of increase in ED RSI numbers suggests that patient selection criteria by emergency physicians are appropriate.
Complications
Immediate post-intubation destination from the ED
Acknowledgments
We would like to thank all the emergency medicine, anaesthesia, and intensive care medicine staff and the emergency department nurses at the Southern General Hospital for contributing data to this study. We also acknowledge the key role of the Scottish Trauma Audit Group in creating and providing the form used for data collection for this and other studies.
Footnotes
-
Competing interests: C Graham is a member of the committee developing the UK Emergency Airway Course.