Article Text

Abstract
Objectives: To quantify the health gains and costs associated with improving ambulance and thrombolysis response times for acute myocardial infarction.
Design: A computer simulation model.
Patients/setting: Patients experiencing acute myocardial infarction in England.
Interventions: Improving the ambulance response time to 75% of calls reached within 8 minutes and the hospital arrival to thrombolysis time interval (door-to-needle time) to 75% receiving it within 30 minutes and 20 minutes, compared to best estimates of response times in the mid-1990s.
Main outcome measures: Deaths prevented, life years saved, and discounted cost per life year saved.
Results: Improving the ambulance response to 75% of calls within 8 minutes resulted in an estimate of 5 deaths prevented or 57 life years saved per million population per year, with a discounted incremental cost per life year saved of £8540 over 20 years. The corresponding benefit of improving the door-to-needle time to 75% of myocardial infarction patients within 30 minutes was an estimated 2 deaths prevented and 15 life years saved per million population per year, with a discounted incremental cost per life year saved of between £10 150 to £54 230 over 20 years. Little further gain was associated with reaching the 20 minute target. Combining ambulance and thrombolysis targets resulted in 70 life years saved per million population per year.
Conclusions: Improving ambulance response times appears to be cost effective. Reducing door-to-needle time will have a smaller effect at an uncertain cost. Further benefits may be gained from reducing the time from onset of symptoms to starting thrombolysis.
- MI, myocardial infarction
- CHD, coronary heart disease
- DTN, door-to-needle
- NICE, National Institute for Clinical Excellence
- NSF, National Service Framework
- UKHAS, United Kingdom Heart Attack Study
- computer simulation
- thrombolysis
- ambulance response time
- myocardial infarction
- cost effectiveness
Statistics from Altmetric.com
- MI, myocardial infarction
- CHD, coronary heart disease
- DTN, door-to-needle
- NICE, National Institute for Clinical Excellence
- NSF, National Service Framework
- UKHAS, United Kingdom Heart Attack Study
Two proved lifesaving treatments in the management of acute myocardial infarction (MI) are resuscitation from out of hospital cardiac arrest and restoration of blood flow to the blocked coronary artery (using thrombolysis and aspirin and/or primary angioplasty).1–3 In a cardiac arrest resulting from ventricular fibrillation or pulseless ventricular tachycardia, rapid defibrillation is required to return the heart to spontaneous output before brain and cardiac death occurs. Thrombolysis limits damage to the heart muscle and its consequences. Standards of care for these treatments in the National Service Framework (NSF) for Coronary Heart Disease for England in 20004 include an ambulance response for life-threatening calls within 8 minutes and 60 minutes call-to-needle time for eligible thrombolysis patients.
The aim of this study is to quantify, using a computer simulation model, the health gains and the costs associated with moving from practice in the mid-1990s to meeting the NSF ambulance and thrombolysis targets.
METHODS
Coronary heart disease computer simulation model
This paper describes results derived from a discrete event simulation of the treatment of coronary heart disease (CHD), from the first onset of angina, or MI, to age 85 years or death.5 A further simulation to model interventions for preventing of CHD was developed in parallel.6 Both simulations were written using patient orientated simulation technique software (POST) with a Delphi interface.7 They were used to test the cost, effect, and overall cost effectiveness of treatments and interventions, based on the most recent published data available.
In the treatment model, simulated patients transfer between stable and unstable angina, MI, and sudden cardiac death,6 There is an arbitrary cut-off point of 85 years because older patients have multiple diseases and it is difficult to isolate the data relating to CHD. In discrete event simulation, an event is a point in time at which a patient’s state changes (for example, a patient joins a waiting list or has an MI). The transitions between events are based on risks such as age, severity of coronary artery disease, and previous history of CHD. Times between events are sampled from the relevant distribution for each patient, depending on the events and risk group. Parameter estimates are based on best evidence through searching the Cochrane database, MEDLINE and EMBASE, checking grey literature, and in discussion with experts. The simulation output has been validated against current routine sources of data.8,9,10,11,12,13,14 In this research, we are looking at implications of faster access to treatment for MI and so MI is in the centre of the simplified diagram of patient flows in the model shown as fig 1. For more details of the simulation model construction and assessment of model validity please see www.emjonline.com/supplemental/ and/or reference 5.

Simplified diagram of the coronary heart disease (CHD) treatment model. MI, myocardial infarction.
The simulation (see fig 1) describes the flow of patients from disease or treatment state to the next. Separate spreadsheet models described:
-
the effects of faster ambulance arrival times on death rates both before and after admission to hospital with MI
-
the effect of varying the provision of thrombolysis and the timing of thrombolysis on the relative risk of death for patients after admission to hospital.
These relative risks were then incorporated into the simulation model in order to assess the life years saved under different policies.
Sources of data
To address the cost effectiveness of the NSF ambulance and thrombolysis targets, all parameter estimates not directly affected by changing ambulance and thrombolysis timings were fixed. For more details, please see www.emjonline.com/supplemental/. Ambulance and thrombolysis data were extracted from three datasets: Heartstart Scotland (1991–98), the United Kingdom Heart Attack Study (UKHAS)(1994–95), and the West Midlands Thrombolysis Project (1995–98).1,9,15
Ambulance response time and survival
In the UKHAS, 61% of patients had witnessed cardiac arrests or MIs.9 The Heartstart study provided data by ambulance response times on the survival rate to hospital admission for patients where resuscitation was attempted. The 8 minute ambulance response target was estimated by moving the 75% quartile in Heartstart Scotland of 10.4 to 8.0 minutes. To achieve this, all calls that occurred between 8.0 and 10.4 minutes were added to the baseline frequency of calls in each time band (0–8 min) in proportion to the number of calls in these bands. The 25% of baseline calls that occurred after 10.4 minutes were each decreased by a simple downward shift of 2.4 minutes (table 1). To obtain a new survival rate to hospital arrival for patients experiencing a witnessed cardiac arrest or MI, the percentage frequency in each time band was multiplied by the survival rate for that time band and summed over all time bands.1 The overall estimated change in survival rate for all cardiac arrests or MIs was applied to the survival rate in each age/sex band.
Ambulance response time distribution for cardiac arrest patients at baseline and for achieving the National Service Framework target
UKHAS showed that cardiac arrest survivors were four times more likely to die prior to hospital discharge than other patients with an acute MI. We have assumed therefore that the additional patients who survive as a result of faster ambulance times have this poorer inhospital survival rate, thus reducing the overall hospital survival rate. We explored the impact of changing this mortality rate in a sensitivity analysis using a hypothetical assumption: that cardiac arrest survivors have an inhospital survival rate similar to those who do not experience an out of hospital cardiac arrest.
Thrombolysis timing
In the UKHAS about 50% of acute MI patients at hospital arrival were diagnosed as having experienced a definite MI and received thrombolysis.8 We assessed the effect of reducing the median time from hospital arrival to thrombolysis for such patients—that is, door-to-needle (DTN) time. Another 10% of patients had a definite MI and indications for thrombolysis but did not receive it. The effect of providing thrombolysis for such patients was also assessed.
Estimates of thrombolysis efficacy were taken from a meta-analysis.2 Data for efficacy were related to the time interval from onset of symptoms to administration of thrombolysis—that is, a relative mortality risk of 0.70 was associated with a time interval of up to 1 hour; 0.74 for 2–3 hours; 0.79 for 4–6 hours; 0.85 for 7–12 hours and 0.98 for more than 12 hours. The effect of using efficacy estimates from a more recent meta-analysis,16 which showed greater efficacy in the first few hours, was estimated in a sensitivity analysis. Long term follow up data show that following thrombolysis, there is little evidence that further lives are saved after 45 days.17 We have therefore assumed that thrombolysis only affects inhospital mortality rates.
In the West Midlands Thrombolysis Project, which provided data on event times for patients with definite MIs diagnosed at hospital arrival,15 the 75th percentile DTN time was 80 minutes. To derive a frequency distribution in which the 75th percentile DTN time was 30 minutes, we multiplied each individual patient’s DTN time by three-eighths and calculated new symptom-to-needle times. It was thus possible to derive the change in efficacy arising from the faster DTN times (see table 2) from the symptom-to-needle times. A similar approach was used to derive the distribution for the 20 minute DTN target. The overall change in hospital survival, taking into account both those who require thrombolysis and those who do not, was applied to the survival for each age/sex group.
Distribution of time from hospital arrival to thrombolysis (door-to-needle time) for eligible patients (excluding the 10% of patients who fail to receive treatment), baseline and proposed for achieving the National Service Framework 30 minute target
Costs
The Review of Ambulance Performance Standards estimated that the cost associated with attaining a 75% ambulance response time within 8 minutes would be £15 million for England (excluding London).18 This cost was scaled to the total population being modelled, up-rated to year 2000 costs and applied as a fixed cost in the scenarios which used relative risks arising from a 75% response time target. These costs compared well with the actual spend by the Department of Health on improving ambulance response times, which was around £18 million per annum for the whole of England from 1999 to 2002. The Department of Health expects the ambulance response target to be met overall but acknowledges that there will be significant variation between NHS ambulance trusts.19
Unit costs of thrombolytic drug treatment were taken from the British National Formulary.20 The cost of streptokinase and alteplase was £83 and £735, respectively. It was assumed that 83% of patients received streptokinase and 17% alteplase (as found in the UKHAS) with just one administration of the relevant drug. Reteplase and tenecteplase were not widely available at the time and we did not include them in the model.
In attempting to reduce time to thrombolysis, a number of strategies have been tried such as improving communication between ambulances crew and receiving hospitals, and moving thrombolysis to the accident and emergency department. Some studies have shown that increasing deployment of nurses to coordinate assessment and initiation of thrombolysis can achieve the 30 minute DTN target.21,22 In each study, more than four experienced cardiac nurses were trained to undertake this new role. However, there was little information on the extent of additional staff requirements. We assumed that one to five additional F or G grade nurses would be needed, with an annual salary of between £22 500 and £25 000 (plus 40% overheads, at 2000 prices) for a population of about 250 000 (the average catchment of a hospital providing thrombolysis, based on information from the Myocardial Infarction National Audit Project (MINAP)).23 These costs were scaled up to a population of one million, and applied in the scenarios about faster access to thrombolysis.
Derivation of cost per life year saved
The estimated life years saved each year was the difference between the total number of patient life years in the simulated scenario, with the changed relative risks, compared to the base run. The costs in the model, which were the estimated NHS costs, for the treatment of coronary heart disease were compared between the scenarios. The annual incremental cost per life years saved of each scenario compared to baseline were accumulated over 20 years; costs were discounted at 3.5% and benefits were discounted at 3.5%, as recommended by the National Institute for Clinical Excellence (NICE).24 The discounted costs per life year saved were averaged over the 20 years.
Simulations and sensitivity analysis
A simulation was run for all CHD patients arising from a population of 0.5 million people, for 20 years with 100 replications. The results were scaled to a population of one million. The main scenarios were as follows:
(1) 75% of “life-threatening” calls to receive an ambulance response within 8 minutes.
(2) 75th percentile of distribution of DTN time for thrombolysis is 30 minutes (with the existing proportion of patients receiving thrombolysis).
(3) 75th percentile of distribution of DTN time for thrombolysis is 20 minutes (with the existing proportion of patients receiving thrombolysis).
(4) 75th percentile of distribution of DTN time for thrombolysis is 30 minutes (including the additional eligible patients (10% of the total) who currently fail to receive thrombolysis).
(5) Combination of scenarios 1 and 2.
The results from each scenario were compared with the baseline values, shown in the relevant tables, which relate to the position in England in the mid-1990s. We explored the sensitivity of the results to the following scenarios:
(6) The mortality rate for cardiac arrest survivors. For the ambulance response scenario 1, those cardiac arrest survivors were assumed to have a similar in-hospital survival rate to those who did not experience an out of hospital cardiac arrest.
(7) “Best” ambulance scenario. The distribution for ambulance response time gives the same target response times but was skewed to the left. All response times over 2.4 minutes were decreased by 2.4 minutes, unless they became negative in which case they were zero.
(8) “Worst” ambulance scenario. The distribution for ambulance response times gives the same target response times but the response times were reduced by the minimal amount possible to achieve that target.
(9) Increasing the target ambulance times. 90% of “life-threatening” calls to receive an ambulance response within 8 minutes. The distribution for ambulance response times is calculated in a similar way to that for scenario 1.
(10) Higher relative risks for reducing mortality. For thrombolysis scenario 2, we used Boersma et al’s16 relative mortality risk estimates.
RESULTS
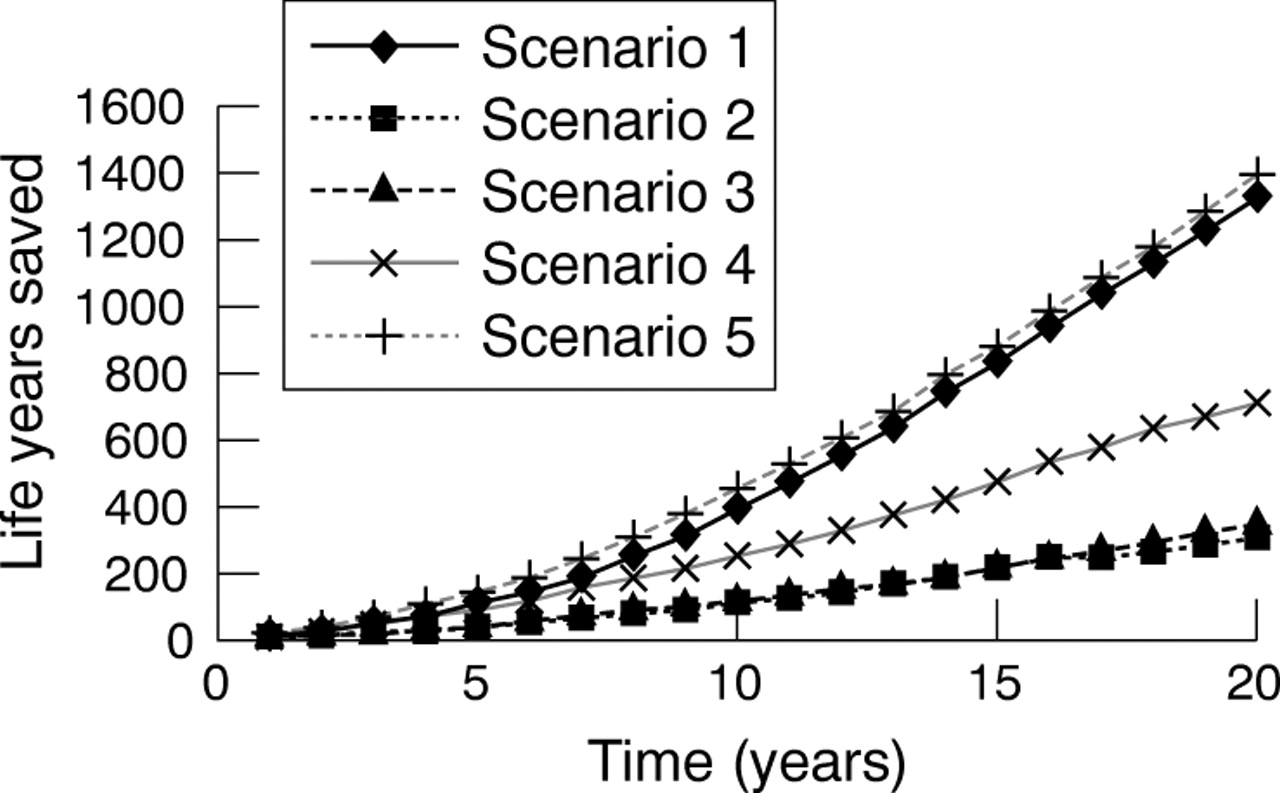
The estimated number of deaths prevented per million population per year ranged from two to seven across the five main scenarios, and life years saved from 15 to 70 (table 3). The standard deviations of these results show that in different populations the outcome may vary considerably. Based on the average values, the ambulance target generated 42 more life years saved than were saved by achieving the 30 minute DTN target. Little difference was found between the 30 minute and 20 minute DTN targets. Increasing the use of thrombolysis to a further 10% of patients had similar benefits to improving DTN times to a 75th percentile of 30 minutes. Figure 2 shows that the difference in the cumulative number of lives saved between these scenarios increases over the 20 year simulation.
Average and 95% confidence intervals (for 100 replications for coronary heart disease (CHD) patients in 500 000 population) of estimated average annual values of CHD life years saved (undiscounted) and deaths prevented for a population of one million
{kind=link}
{kind=link}
Undiscounted cumulative lives saved over a 20-year simulation run.
Sensitivity analysis
The results for the sensitivity analyses are shown in table 4. Assuming that cardiac arrest survivors had the same in-hospital mortality rate as those who did not have an out of hospital cardiac arrest (scenario 6) increased the estimated life years saved per million population by 48. The results are shown to be sensitive to the ambulance response profile and the worse and best scenarios ranged between 35 and 81 (scenario 8 and 7). Increasing the ambulance response to 90% within 8 minutes (scenario 9) would result in a further 28 life year saved over scenario 1. The benefits of thrombolysis were sensitive to the efficacy estimates; the use of Boersma et al’s15 data improved the life years saved to 24 for the 30 minute DTN scenario.
Sensitivity analysis: estimated average annual values of coronary heart disease (CHD) life years saved (undiscounted) and deaths prevented for a population of one million
Ambulance response time cost effectiveness
The marginal annual cost of achieving the 8 minute target was estimated at £448 100 for a population of one million. The estimated discounted incremental cost per life year saved, to age 85, accumulated over 20 years and divided by 20 to get the average per year, was £8540. The cost effectiveness ratios are much less favourable in the short term with an accumulated value of £19 110 per year at 5 years and £12 400 per year at 10 years.
Thrombolysis time cost effectiveness
The annual cost of nurse initiated thrombolysis to meet the 30 minutes DTN time for thrombolysis was assumed to be between £135 000 and £752 500 per million population. The discounted incremental cost per life year saved, to age 85, accumulated over 20 years and divided by 20 to get the average per year, was estimated to be between £10 150 and £54 230. Again, the cost effectiveness ratios are less favourable in the short term with the cumulative values for the lower cost at £20 560 per year in 5 years and at £13 800 per year in 10 years.
DISCUSSION
This simulation model has indicated that it may be cost effective to improve both ambulance response and thrombolysis DTN times with results from a 20 year period or more. The costs per live years saved were well below the putative threshold set by NICE.25 Much greater benefits are achieved by reaching the ambulance response target; particularly with the higher 90% response target. However, the benefit of ambulance timing was sensitive to the assumption about the poorer inhospital survival rate for cardiac arrest survivors; though the weight of evidence suggests a poorer prognosis for these patients than MI patients who have not experienced a cardiac arrest.9 Further research is needed on the impact of faster ambulance times on inhospital mortality rates. Very little additional gain is achieved by moving from the 30 minute to the 20 minute NSF thrombolysis target, whereas ensuring that all eligible patients receive thrombolysis would be beneficial.
Although our model is based on UK data, our results would be applicable to other developed countries with similar emergency services. Since the 1990s, changes in practice have led to ambulance response times and speed of delivery of thrombolysis (sometimes involving use of newer agents) that are now more in line with the NSF targets.4
The cost effectiveness of achieving the ambulance target might be greater if non-CHD lives saved were included, but there were no data to estimate this. Furthermore, there are likely to be local variations in the feasibility and cost of achieving the target, particularly between urban and rural populations. The Review of Ambulance Performance Standards estimated that moving to the 75% target would gain 530 life years per million population per year at a cost per life year saved of £1100 which is more favourable than our estimates.18 This is likely to be optimistic because long-term mortality risk associated with MI was not taken into account. Pell et al showed that shorter ambulance response times increased the proportion of cardiac arrest victims receiving defibrillation and increased survival to hospital discharge; they estimated that a 90% 8 minute response time would save about 5–6 deaths per million population per year.26 These are close to our estimates.
Our thrombolysis results may have underestimated the absolute benefit by taking an optimistic baseline time distribution from the West Midlands Thrombolysis Project in which hospitals volunteered for the audit to promote improvement.27 There is wide variation in the cost effectiveness estimates for the 30 minute DTN target depending on the numbers of new nursing staff needed. There are other costs, which we have not taken into account, such as a possible increased need for coronary care unit (CCU) staff which would reduce the cost effectiveness.22 In common with other studies, we have not taken account of the cost of treating patients whose lives are saved but who acquire other diseases. These are likely to be considerable in the older population.
It is important to consider other approaches, to reducing time from symptom onset to starting thrombolysis. Public education on identifying heart attack symptoms might be expected to further increase lives saved. The SHARP study found that delays to hospital arrival were greater in those who contacted their general practitioners directly.28 However, studies evaluating educational campaigns designed to reduce delay between symptom onset and treatment of suspected MI have generated inconclusive results.29 Campaigns aimed at ensuring calls are made directly to the ambulance service may save some lives but may increase inappropriate calls and costs.30 Prehospital thrombolysis is increasingly available in the UK and could further increase lives saved especially in remote areas.31
In conclusion, improving ambulance response and inhospital time to thrombolysis appears to be cost effective. The absolute gain with improving ambulance response is much greater than that associated with further reducing DTN time for thrombolysis.
Acknowledgments
We acknowledge the funding from the National Central Health Outcomes Unit. The research has been done in conjunction with the London School of Hygiene and Tropical Medicine led by Dr C Sanderson, and has been supported by a steering group including representatives of the Department of Health, London. We are indebted to the contributors of study datasets and analyses beyond published work, in particular, Dr R Norris (UKHAS), Dr J Birkhead (West Midlands Thrombolysis Project) and Professor S Cobbe (Heartstart Scotland Study).
Authors’ contributions >DC wrote the first draft of the paper, and all authors contributed to the revision and agreed the final version. RD, PR, and JR conceived the study and oversaw the development of the model, and KC and RD were responsible for writing and running the model. DC and PR undertook background epidemiological research to identify parameter values, and JR advised on health economic aspects and TQ on clinical and NHS issues.
REFERENCES
Footnotes
-
Competing interests: TQ is a member of an advisory board for Boehringer Ingelheim.