Article Text

Abstract
Background and purpose Ambulance workers could benefit from a method for early identification of incidents likely to result in long-term emotional sequelae. There is evidence that persistence of some measures of anxiety beyond the first week after an incident is associated with sequlae. In this study we test the hypothesis that persistence of self-identifiable components of the acute stress reaction as early as a few days post-incident is associated with sequelae.
Method 228 ambulance workers volunteered to complete surveys on occurrence and persistence of physiological, behavioural and emotional responses to an index critical incident in the past, as well as symptoms of depression, post-traumatic stress, somatisation and burnout at the time of the survey. Data were analysed for associations between duration of each reaction and present symptoms. Using cut-off scores for the outcomes, we tested the RR of high scores in each of three situations: occurrence of the reaction, persistence of reaction beyond one night and persistence beyond 1 week.
Results Prolonged duration of all five acute stress reaction components was associated with all four outcomes, with the strongest associations being with post-traumatic stress and depression symptoms. The occurrence of physical symptoms of arousal is an immediate predictor of long-term sequelae. Three other components—disturbed sleep, irritability and social withdrawal—provide potential indicators of long-term emotional sequelae as early as 2 days post-incident.
Conclusion Four easily identifiable responses to a critical incident can potentially be used for early self-identification of risk of later emotional difficulties. These findings should be submitted to prospective testing.
- Critical incidents
- ambulance workers
- posttraumatic stress
- early intervention
- nursing
- pre-hospital
- prehospital care
- first responders
- psychology
- psychological conditions
Statistics from Altmetric.com
- Critical incidents
- ambulance workers
- posttraumatic stress
- early intervention
- nursing
- pre-hospital
- prehospital care
- first responders
- psychology
- psychological conditions
Background and purpose
Ambulance workers frequently encounter stressful or ‘critical’ incidents that can result in significant emotional sequelae, such as depression and post-traumatic stress symptoms1 and burnout.2 Somatisation, the expression of emotional difficulties through somatic symptoms, has also been reported in ambulance workers.3 Early identification of incidents that are likely to have later sequelae would potentially facilitate early intervention, which would help maintain operational readiness. Ambulance workers are often reluctant to report emotional distress for a number of reasons, such as difficulty identifying emotions, shame at feeling distressed and fear of stigma.4 There is some evidence that both intensity of distress5 and its persistence in the early post-incident period6 predict later sequelae. There is also evidence that persistence of anxiety,7 insomnia8 and increased heart rate9 beyond the first week are associated with later sequelae. The acute stress reaction (ASR)10 11 is a response to exceptional stress that usually lasts 2–3 days. In this study we test the hypothesis that the post-incident occurrence and persistence of five common and self-identifiable components of the ASR is associated with the risk of later sequelae.
Method
Participants and procedure
Ambulance workers, both front-line and supervisors, were recruited from attendees of a mandatory continuing medical education programme in a large urban Emergency Medical Services organisation. A recruitment letter informed ambulance workers on leave. Subjects completed their choice of paper or web-based survey. Participants' names were entered into a draw for monthly prizes worth up to $600. Nine hundred and six ambulance workers were informed of the study. Of the 635 who signed consent forms, 243 completed the questionnaire package, and 228 (36%) provided usable data on recovery from at least one ASR component. Research ethics board approval was obtained.
The 228 participants in this analysis included 146 (64%) men and 81 (36%) women (one not answered). Mean age was 37.5 (SD 9.3, range 22–59). Level of training (beginning with basic) was distributed as 96 (42%) level 1, 41 (18%) level 2, 83 (36%) level 3, 4 (2%) supervisors, 4 (2%) not answered. Mean years of service were 7.6 (SD 3.3, range 1–12). Seventy-five (33%) were single, 138 (61%) married or common-law and 14 (6.1% divorced or separated; 1 not answered). These demographics were representative of the organisation, except that female gender and highest level of training were over-represented. In the organisation, 24% of ambulance workers are female and 25% have level 3 training.
Instruments
Critical incidents
We asked participants how many critical incidents they had experienced. We defined critical incidents as ‘calls that have generated unusually strong feelings, either because of the incident itself, or how it was handled or some other reason’. In order to identify an index incident, participants were asked to identify an incident that was ‘still troubling’. Those who could not identify a still troubling incident were asked to identify an incident that ‘had been troubling in the past’. Failing this, they were asked to describe ‘a composite of a number of critical incidents’. Finally, those who were unable to describe a composite were asked to describe ‘one of your worst calls’. We also inquired about how long ago the index incident took place, or over what time period in the case of the composite.
Duration of reactions to critical incident
We measured five components of the ASR in response to the index critical incident. The components measured were physical reactions (‘like sweating, shaking and pounding heart’), distressing feelings (‘like fear, anger, horror, guilt, shame worry or sadness’), disturbed sleep (‘sleep disrupted by the incident’), irritability (‘irritable, mean or snappish’) and social withdrawal (‘if you withdrew or pulled back from other people’). For each dimension, participants reported the occurrence in response to the incident and how long it took to get back to normal by choosing one of seven options: (i) did not have this reaction; or returned to normal (ii) soon after the call (a few hours), (iii) by the next night, (iv) by the next week, (v) by the next month, (vi) within a few months or (vii) still not normal.
Psychological symptoms at time of the survey
Centre for Epidemiological Studies Depression Scale, short form
This 10-item scale is the short version of the CES-D. Responses rated the frequency of depressive phenomena on a four-point scale from 0 (rarely or none of the time, less than 1 day) to 3 (all of the time, 5–7 days). The scale is scored as the sum of all item scores. CES-D-10 scores show concurrent validity with measures of positive affect (r=−0.63) and poor health status (r=0.37). The 10-item scale is highly correlated with the CES-D, which has been validated against clinical diagnoses of depression.12 The cut-off score for the CES-D has been validated with and the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV), major depression. The CESD-10 cut-off score of 10 discriminates consistently with the cut-off score for the original.13 Internal reliability was 0.77.
Impact of Events Scale-Revised (IES-R)
This 22-item measure of traumatic stress probes the intensity of responses to a particular event on a 5-point scale from 0 (not at all) to 4 (extremely). The scale is scored as the mean of item scores. The IES-R yields three subscales (avoidance, intrusion and hyperarousal) and a total score. The three subscales have strong internal consistency and satisfactory test-retest reliability.14 The correlation between the Mississippi Scale for Combat-Related PTSD, Civilian Version and the three subscales of the IES-R were: Intrusion, r=0.53, Avoidance, r=0.55 and Hyperarousal, r=0.55.15 A cut-off of ≥1.5 has been used to identify possible cases. Internal reliability for total scale was 0.91.
Brief Symptom Inventory (BSI) somatisation subscale
The BSI is abbreviated from the Symptom Checklist 90-Revised. The seven-item somatisation scale probes how much the participant was distressed by the discomfort of a physical symptom using a 5-point scale, from 0 (‘not at all’) to 3 (‘extremely’). The SCL-90 has demonstrated reliability and validity.16 The BSI-somatisation scale has been validated against the SCL-90R and comparable scales of the MMPI. To identify cases, a cut-off was set at the value of the mean+1 SD in a non-psychiatric patient normative sample (cut-off=0.69).17 Internal reliability was 0.79.
The time period for the three scales above was altered from the standard ‘over the last week’ to ‘your current or most recent block of shifts on duty’ because in a pilot study ambulance workers reported that psychological distress was worse during blocks of shifts on than during time off.
Maslach Burnout Inventory Human Services Survey-Emotional Exhaustion scale
This questionnaire enquires about present job-related feelings. Responses describe the frequency of phenomena in seven categories from 1 (never) to 7 (every day). There is strong psychometric evidence of both reliability and validity for three subscales. A cut-off of 27 on the 9-item emotional exhaustion subscale was used to identify burnout, based on the recommendations of the scale's authors.18
Data analysis
The independent variables in this analysis were the occurrence and persistence of five components of the ASR in response to the index critical incident. Time to recovery was measured with a seven-category ordinal variable, in which responses were ordered chronologically but with variable time periods between categories. Recovery curves were plotted as the percentage of participants not yet recovered at each time point. Spearman's rank order correlations were calculated to measure the association between five ASR component recovery trajectories and four measures of current psychological symptoms (depressive symptoms, post-traumatic stress symptoms, professional burnout, somatisation symptoms).
To determine if specific durations of components were associated with risk of subsequent high psychological distress, outcome variables were dichotomised using cut-off scores. Component recovery scores were also recoded into dichotomous variables. Three time-based cut-offs were tested: occurrence of component (any/none), persistence of component after one night (yes/no), persistence of component after 1 week (yes/no). For each dimension of component recovery, we tested the RR and OR of high depressive, post-traumatic, burnout and somatisation symptoms at each of these three time points. Significance was set at p<0.05, two-sided tests. Statistics were performed with SPSS (16.0) and with online calculators of risk metrics.19
Results
Critical incidents
Data on number, types and time elapsed since the index critical incident are presented in table 1.
Data on all critical incidents experienced and the index critical incident
Distribution of symptom scores
Depressive symptom scores (CESD-10) were approximately normally distributed (mean 7.4±4.5). When completing the IES-R, 56 participants (25%) identified the index event as a critical incident, 126 (55%) indicated some other experience and 46 (20%) did not specify an event. Post-traumatic symptom scores were non-parametrically distributed and skewed towards the minimum score (median 0.7, interquartile range 0.3–1.0). Somatisation symptom scores (BSI-somatisation) were non-parametrically distributed and skewed towards the minimum score (median 0.36, interquartile range 0.18–0.64). Burnout scores (MBI-EE) were approximately normally distributed (mean 21.9±11.5).
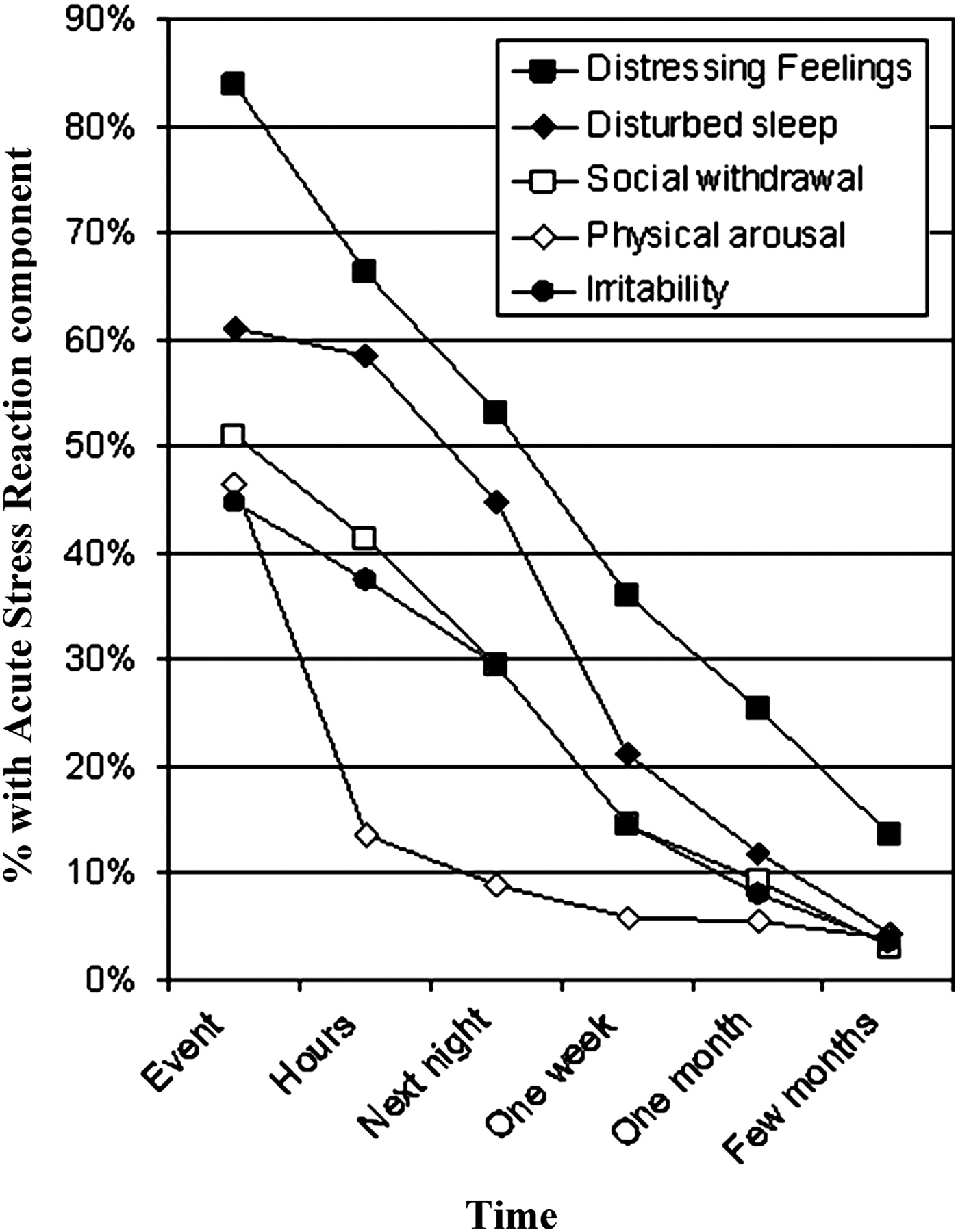
Occurrence of ASR components and timing of recovery
Data on the frequency of the five types of ASR components, and time to recover from them are presented in table 2, and illustrated in figure 1.
Occurrence and persistence of five components of the ASR after an index critical incident

Time to recovery from five components of acute stress reaction.
Relation of duration of ASR components to psychological symptoms
Time to recover from ASR components was significantly and positively correlated with current psychological distress for each of depressive symptoms, post-traumatic symptoms, somatisation symptoms and professional burnout (figure 2). The strength of this correlation was weak for recovery from distressing feelings (Spearman's ρ ranging from 0.15 to 0.22 for four psychological outcomes) and weak to moderate for recovery from each other component (Spearman's ρ ranging from 0.23 to 0.36, all p<0.05).

{kind=link}
{kind=link}
Relation between recovery from acute stress reaction components and subsequent psychological distress.
Among the participants of this study, high depressive score (CESD-10≥10) was present in 55 (24%), burnout (MBI-emotional exhaustion ≥17) was present in 67 (29%), high post-traumatic symptoms (IES-R≥1.5) were present in 19 (8%) and high somatisation symptoms (BSI-somatisation ≥0.69) were present in 36 (16%). For each dimension of recovery, we tested the RR and OR of high symptom scores at three time points: (i) any occurrence (ii) persisting at least one night, and (iii) persisting at least 1 week. The RR of post-traumatic symptoms (table 3) increases dramatically if any of the components persist beyond one night. The increase in RR ranged from more than doubling (RR=2.4 for distressing feelings) to an almost eightfold increase (RR=7.9 for social withdrawal). RR of high post-traumatic symptoms is highest using the 1-week criterion for each component of recovery.
Persistence of reactions to critical incidents and risk of high post-traumatic stress symptoms
Table 4 shows that physical reactions, disrupted sleep, irritability and social withdrawal are each associated with at least a doubling of the RR of high depressive symptoms if they persist beyond one night. The RR associated with these components is not substantially higher when a 1-week persistence criterion is used. The presence of any (ie even non-persistent) physical reactions more than doubles the risk of high depressive symptoms (RR=2.6), but RR is not higher with more persistent reactions.
Persistence of reactions to critical incidents as predictors of high depressive symptoms
The RR of somatisation and burnout with delayed recovery from ASR components follows a similar pattern but the relation is not as strong. RR of high somatisation is approximately doubled if components last more than one night for all components except distressing feelings, which do not contribute to risk. RR does not increase appreciably beyond the one night criterion. With respect to burnout, there is a modest relation (RR from 1.6 to 2.2) between the occurrence of physical reactions, irritability, disturbed sleep, social withdrawal and burnout symptoms, but the risk does not increase as appreciably over time. For each psychological outcome ORs (the odds of a high symptom score/the odds of a low symptom score when the criterion is met) are somewhat higher than RR but occur in essentially the same pattern.
Discussion
Among ambulance workers, the duration of ASR components after a critical incident is associated with poor long-term psychological outcomes. Longer duration of recovery for each of the five components was most strongly associated with increased risk of post-traumatic stress symptoms, and the recovery duration for four components was also strongly associated with depression symptoms. The recovery duration of components was more weakly associated with the prevalence of somatisation symptoms, and least to burnout. Despite the somewhat weak association of recovery duration of components with somatisation symptoms, the RR of somatisation symptoms is nonetheless doubled if some of the components persist beyond one night post-incident. This suggests that the association of somatisation with critical incidents, a subject that has not been previously studied, deserves further attention. Burnout may have the weakest association with post-critical incident recovery because it is caused by many factors, including chronic workplace stressors.
There are four signs of acute stress that can be identified within 2 days of a critical incident that are associated with at least a doubling of the RR of high post-traumatic, depressive and somatisation symptoms. These are the occurrence of any physical arousal symptoms or the persistence of insomnia, irritability or social withdrawal beyond one night post-incident. The potential for recognising by the second post-incident day that the risk of long-term psychological sequelae is high has substantial appeal because swift identification presents the possibility of early intervention such as workplace support and possibly cognitive-behavioural therapy.20 This will be valuable for ambulance workers who, as a group, have difficulty identifying critical incidents and prefer intervention soon after the incident. Furthermore, the signs and symptoms that indicate elevated risk are physiological and behavioural, which appear to be more readily identifiable than emotions for ambulance workers. Self-identification may reduce the stigma and loss of control involved in organisational screening.
Study limitations and future directions
While the association of prolonged reactions to critical incidents and subsequent psychological symptoms is consistent with a causal relation, the study design precludes drawing any conclusions about causality. Further, we do not know what other stressors either concurrent with or following the index critical incident may have contributed to long-term outcomes. It should be emphasised that the outcomes of the current study are self-reported symptoms and not psychiatric diagnoses. Further research could include objective measures of symptom burden, diagnosis and functional impact. Other limitations of this study include self-selection of subjects, which may have introduced a biased sample and a low participation rate. The issues raised in this study require further investigation in research designed to overcome the limitations of a retrospective study.
Conclusion
In this cross-sectional study, we found that prolonged duration of five components of the acute stress reaction following a critical incident is associated with increased symptoms of post-traumatic stress and depression, and to a lesser extent, somatisation and burnout. Three of the components studied—disturbed sleep, irritability and social withdrawal—provide potential indicators of later significant symptoms as early as 2 days post-incident. The existence of physical symptoms of acute distress is a potential indicator of later symptoms even before 2 days. These indicators offer the possibility of early self-identification of later psychological difficulties, which is particularly useful for at-risk occupations such as first responders. The findings of this study should be submitted to prospective testing.
References
Footnotes
Funding Tema Conter Memorial Trust, 10480 Islington Ave, Suite 6, Kleinburg, Ontario. Canada L0J 1C0.
Competing interests None.
Ethics approval This study was conducted with the approval of the Sunnybrook Hospital and Mt Sinai Hospital, Toronto, Canada.
Provenance and peer review Not commissioned; externally peer reviewed.