Article Text

Abstract
Objectives—To examine the profile of regular attenders to an accident and emergency (A&E) department, and to estimate the percentage of the overall departmental workload attributed to this group of patients, together with the resultant cost to the department of these attendances.
Methods—A retrospective study of regular attenders to the A&E department at Hull Royal Infirmary was conducted between 1 January 1998 and 30 June 1998. The information gathered included age, sex, marital status, accommodation, investigations performed, concurrent alcohol use, presenting complaints and disposal.
Results—The A&E department at Hull Royal Infirmary sees approximately 87 000 new patients per year. Forty regular attenders presented 475 times in six months accounting for 1.1% of the departmental workload. The most common presenting complaints were overdose (27.4%), minor injuries (19%), alcohol intoxication (14%) and seizures (10.5%). Eighty per cent of patients were single and 7.5% were of no fixed abode. A total of 191 admissions resulted and the cost to the department for investigations performed was between £2709.59 and £3739.85. The cost of inhospital admissions was in excess of £34 000.
Conclusion—Improved management of these patients together with a reduction in their alcohol intake may lead to a significant reduction in both workload for accident departments and hospitals and in the number of regular attenders.
- regular attender
- cost
- investigations
Statistics from Altmetric.com
A number of studies identify alcohol1 and homelessness2 as factors associated with frequent and often inappropriate attendance at emergency departments, the second group of patients often using emergency departments as a substitute for primary care.2 Li et al3 have estimated the annual rate of alcohol related emergency department visits in the USA at 10 visits per 1000 population, while Yates et al4 demonstrated in their study that 13.2% of their patients tested positive for alcohol. The number of attendances by homeless patients has been calculated at 1.3 per 1000 adult attendances.5
The aim of this study was to profile our “regular attenders” to identify how many actually fit the category of “regular attenders” and estimate the percentage of the overall workload of the department attributed to this group of patients. In addition, we also aimed to examine the number of alcohol related attendances and the proportion of patients classified as having no fixed abode. The range of presenting complaints, investigations performed and the cost of these together with the disposal of these patients were also analysed.
Methods
There seems to be no standardised definition of a regular attender. Several definitions have been proposed, all of which have been arbitrarily chosen, ranging from two or more visits per year6 to more than 10.7 We defined a regular attender as anyone attending the department on average at least once per month over the study period. Therefore, anyone with at least six attendances over the six month period was included for analysis.
A retrospective observational study was performed over the period 1 January 1998 to 30 June 1998 to identify all patients with at least six attendances to the accident and emergency (A&E) department at Hull Royal Infirmary.
These patients were identified by means of a thorough search of the departmental computer database together with an examination of the “regulars folders” kept in the department. Patients were allocated “regulars folders” based on the number of previous attendances. Finally, all A&E cards were examined to avoid missing any eligible patients.
Data collected included age, sex, marital status, accommodation, number and variety of presentations, history of concurrent alcohol or drug use, investigations performed and disposal from A&E.
The cost of the investigations undertaken was calculated on the basis of these being carried out both in hours and out of hours, as it was not always possible to accurately establish when these had been performed. Each department responsible for performing these investigations was contacted to establish their cost. The cost of admission was based on an average cost for an inpatient episode of £200 per night. The inpatient case notes were retrieved to identify the duration of inhospital stay.
Results
A total of 191 “regular attenders” folders are kept in our A&E department, however of these only 40 (20.9%) met the criteria of at least one presentation each month for six months. Eighty one patients (42.4%) attended less than six times while 70 (36.6%) did not present at all during the study period. Therefore, 151 patients (79.1%) previously labelled in our department as regular attenders did not fit the above criteria.
The following analysis is of those 40 patients with at least six attendances in the six month study period.
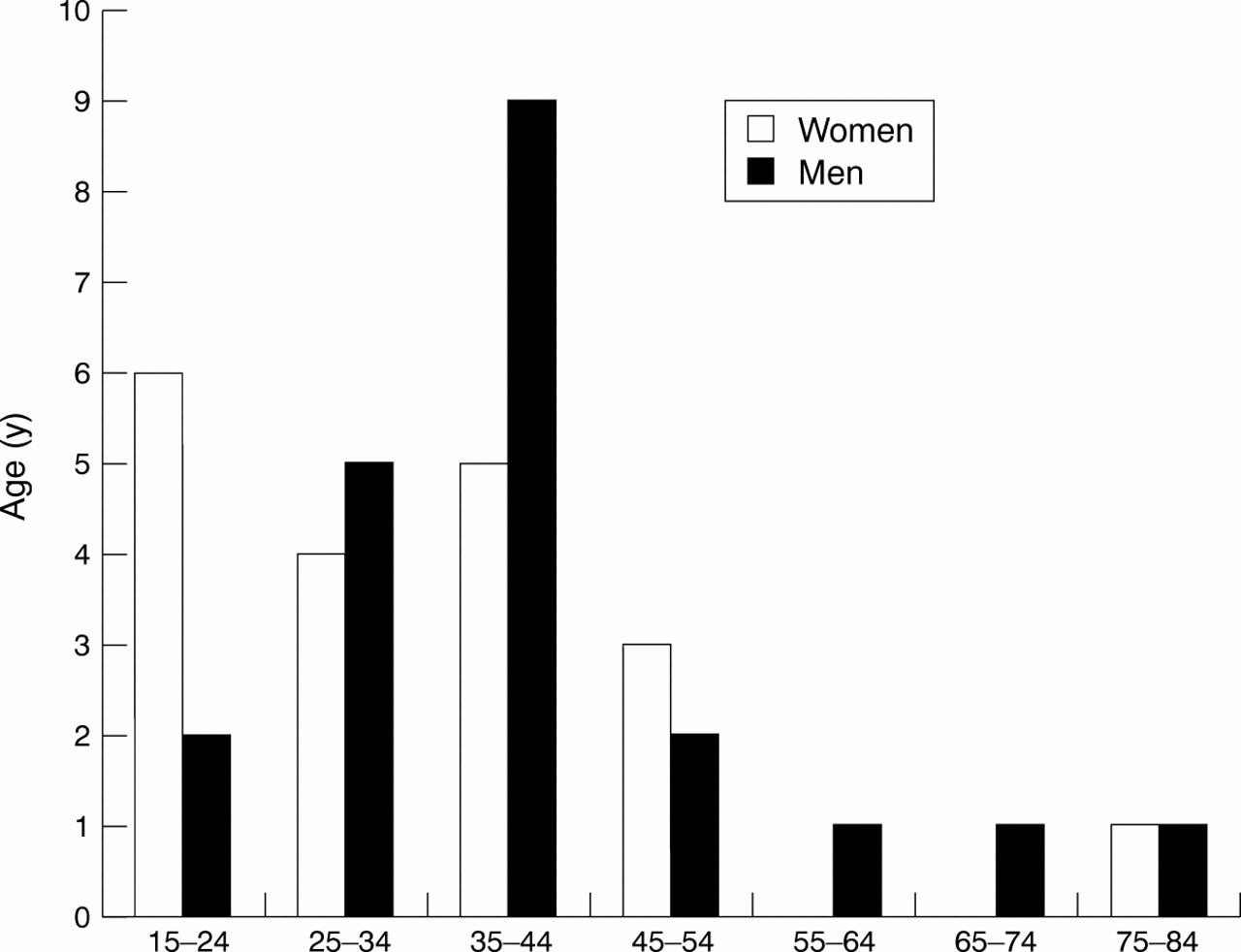
Age distribution showed a peak between 35–44 years for men (43%) while women were fairly equally distributed between the ages of 15–54 years (fig 1). There were almost equal numbers of women (19) and men (21). The vast majority (80%) of regular attenders were single, with 67.5% living at home, 25% in hostel accommodation and 7.5% of no fixed abode (table 1).
Demographic profile of regular attenders
{kind=link}
Regular attenders: number of attendances for patients per age group.
In total there were 475 presentations (range 6–47), one patient having presented 47 times and another 39 times over the six month period. Overall this group accounted for 1.1% of all A&E attendances—that is, 1.1% of 43 327—by the nature and complexity of their presenting complaints, they probably represented more than 1.1% of the workload of the department.
The most common presenting complaints were overdose (27.4%), minor injuries (19%), alcohol intoxication (14%) and seizures (10.5%). Deliberate self harm accounted for 7.5% of the total. Some 26.9% of all presentations were associated with concurrent alcohol use, while a history of concurrent drug use was noted in less than 1% of all presentations (table 2).
Presenting complaints
The most commonly performed investigations in A&E were dipstick testing, alcometer, urea and electrolytes, full blood count, paracetamol and salicyclate levels. The cost of these investigations is estimated between £2709.59 and £3739.85. It was not possible in all cases to establish when these investigations were performed so a range of prices was used to include both the minimum and maximum cost. Furthermore, there was no price breakdown available for in departmental investigations such as dipstick testing and alcometer.
Over 40% of all attendances resulted in admission and the specialties under which these were admitted are detailed in table 3. This compares with an admission rate of 20.3% for all patients attending our department during this period. Some 58.7% of patients were discharged directly from the A&E department. Included in this figure are the 76 times that patients did not wait to be seen. Only two patients were not admitted at any time, while one patient was admitted 21 times and another 14 times (table 3). It was possible in 177 of the 191 admissions (92%) to identify the primary reason for admission. Overdoses accounted for 69 admissions, alcohol intoxication for 36, seizures for 29 and chest pain for 23. However, it was only possible to identify the duration of inhospital stay in 134 of the admissions (70%). The combined total for these was 172 days stay in hospital. Based on an average cost of £200 per night per admission, the resultant cost of these 134 admissions was approximately £34 400.
Disposal of patients
Discussion
A number of studies report that alcohol is closely related to attendance with minor injuries at A&E departments.1, 8–10 Maguire11 has shown in his study that 19.3% of consecutive acute admissions were alcohol related and similar results have been reported by Taylor.12 Maguire also identified that 67% of overdoses were related to alcohol, while, Van der Pol et al,13 have not found alcohol to be a major factor in A&E attendances in the elderly.
Little et al,2 have shown that homeless people may be using the A&E department as a substitute for primary care and that alcohol plays a large part in homeless people seeking medical help in A&E. Our study shows that homeless people accounted for 7.5% of our regular attenders.
A literature search using Medline and Embase has not yielded any studies reporting the cost of investigations and admissions for regular attenders in the A&E department. We estimated the cost of investigations performed to be approximately £2709.59–£3739.85, while the cost for 134 admissions was £34 400. The latter cost was based only on 70% of admissions. It is probable that the total figure for all admissions and investigations, had all case notes been available, would have approached £50 000. If all attendances to our A&E department were equally expensive, then the total cost per year would be over £9.3 million. It is therefore clear from our study that a small group of patients account for a disproportionately large number of attendances (1.1%), cost and admissions. This correlates well with the work of Kne et al7 who identified that 1.9% of their emergency department visits were attributable to 76 frequent attenders.
Although 40 patients accounted for 1.1% of all attendances they in fact account for a far greater amount of both doctors' and nurses' time than most A&E patients. Various reasons may explain why such a small group of patients may take up a disproportionately large amount of staff time. These include the greater complexity of their presenting complaints highlighted by multiple previous attendances, social background, lack of accommodation, concurrent alcohol use and the need to involve other health care professional such as psychiatrists and social workers.
The profile of a “regular attender” based on our results is a single person who lives at home and is aged between 35–44 for men, while for women the age spread is a lot wider (15–54). This correlates well with the work of Murphy et al,14 who identified that frequent attendance to their A&E department was associated with being male, single, poor and increasing age.
A number of reasons may exist as to why such a small number of our perceived regular attenders presented during the time span of our study. As we have already mentioned, 7.5% are of no fixed abode and thus may move between different health regions and simply not have been in Hull at this time. Others may have gained access to alcohol detoxification programmes or achieved improvements in medical and psychiatric management of their conditions. These suggestions concur with the work of Kne et al,7 who identified changing patterns of frequent use over time, which were influenced by substance abuse and psychiatric problems.
It has been shown that compassionate management of homeless adults decreases repeat visits.15 A history of concurrent alcohol consumption was detected in 26.9% of our patients. Overdose, deliberate self harm and alcohol intoxication accounted for 48% of these patients' attendances. Therefore, we suggest that improved compassionate care and, alcohol advice and support services input into these cases could significantly reduce the numbers of reattendances.
This may be achieved in a number of ways such as employing an alcohol advisor to work alongside the two social workers and community psychiatric nurse already in place in the A&E department at Hull Royal Infirmary. Greater availability of and access to alcohol detoxification units may serve not only to get these patients over their acute crises but also to break the cycle of repeat attendances to the A&E department. Some of our regular attenders may also benefit from a multidisciplinary case conference to assess the reasons for and frequency of attending the A&E department and thereby implementing a structured plan of action to tackle these various factors. Additionally improvements in medical management, especially in relation to seizures and chest pain, may have a considerable impact in reducing the number of attendances (19.1%) and admissions (52 of 191) attributed to this group of patients. Finally, improved accessibility to primary care facilities may help to remedy the present situation.
All of the above issues when taken into consideration could result in considerable financial savings and reductions in the numbers of repeat attendances in addition to a significant reduction in the amount of medical and nursing time spent treating this group of patients.
We recognise that our paper is retrospective and is based on the experience at only one hospital, that there are missing data on the duration of some of the admissions, and that it was not possible to randomly choose a representative group of non-regular attenders matched for age, sex, social class and clinical condition. None the less we feel that it provides a valuable insight into the frequency of attendances and admissions of our regular attenders in addition to the costs associated with these.
Conclusion
Regular attenders to A&E departments account for a large proportion of the workload and place a financial burden on these departments as a result of the associated investigations and hospital admissions involved. Reductions in their alcohol consumption and improved medical and psychiatric care may lead to a substantial fall in the number of regular attenders with resultant savings to the health system.
Acknowledgments
Contributors
Richard Lynch devised a data collection form, performed the data collection, analysed the data, collected and read the references for the paper and wrote the substance of the paper. Ian Greaves formulated the idea for this paper, coordinated the project and assisted in devising tables, writing the discussion and corresponded with the editors. Richard Lynch will act as guarantor for this paper.
References
Footnotes
-
Funding: none.
-
Conflicts of interest: none.