Article Text

Abstract
Objective—To study an established triage nurse x ray requesting system to determine whether sending defined groups of patients for radiography before assessment by doctors or emergency nurse practitioners (ENPs) resulted in shorter waiting times for patients without compromising quality of care.
Methods—Prospective randomised controlled study of “walking wounded” patients attending a district general hospital. Data were collected over two separate two week periods, six months apart, in the middle of two senior house officer appointment periods. A total of 675 patients were entered into the study. Analysis of results was achieved using standard statistical methods.
Results—Altogether 335 patients were in the nurse x ray group and 340 in the control group. The triage categories of the groups were similar. A 36% mean time reduction of 37.2 min (95% confidence interval 30.2 to 44.2, p=0.000) from time of triage to time of treatment decision was achieved in the nurse requested group. Triage nurses requested 8% (p=0.002) fewer x rays than doctors or ENPs and had a 6% higher positive “hit” rate (p=0.03).
In 7.8% (26 cases), patients in the triage nurse group were judged to require radiographs or further views by the doctor or ENP; of these, 11 cases showed a positive finding on radiography. The time from triage to assessment by doctor or ENP was not lengthened by prior requesting of radiography (nurse x ray group 64.4 min, control group 63.7 min, p=0.79).
Conclusions—A triage nurse x ray requesting system speeds up the progress of walking wounded patients through the department without compromising service quality. Further benefits are staff and patient satisfaction and a greater sense of team working for all staff.
- radiology
- nurse requested radiography
- triage
- x rays
Statistics from Altmetric.com
One of the major problems facing many accident and emergency (A&E) departments is how to cut down waiting times. A precise figure is not available, but in our department we estimate that over 50% of patients attending the A&E department do so for minor injuries and many of these require radiography. We therefore proposed that if nurses could request x rays at triage, the patient could have the x ray taken while waiting to be seen by a doctor or emergency nurse practitioner (ENP).
In theory, this system could have many advantages. The total time spent by patients in the department should be reduced, the patients have a feeling of progress, and doctors/ENPs could see patients with radiography already requested, thus enabling them to see and decide on treatment with one consultation.
This would therefore save time for patients and reduce the number of consultations needed by doctors. Additional benefits might include patient and staff satisfaction.
The nurse requested x ray system at the Norfolk and Norwich Hospital was set up after a preliminary study carried out by Davies and Finlayson in 1992.1 Their hypothetical study showed an 89% correlation between nurse and doctor x ray requesting with only 6% of patients having radiography requested by a nurse that would not have been requested by a doctor. There was a low positive hit rate for radiographs of elbows, knees, and femurs. This study was carried out on nurses with no previous experience or training of x ray requesting. Subsequently a protocol based system was set up whereby triage nurses could request x rays (table 1).
Summary of Norfolk and Norwich Hospital triage nurse requesting protocol
However it is important to be sure that nurses are able to request x rays appropriately, that there is a time saving in practice, and that the system is satisfactory to patients and staff alike. There is a possibility that nurses may over request or request inappropriate views, thereby negating any potential advantage of this system, as was found by Thurston and Field.2
This study was a randomised controlled trial. It assessed the timing and the quality of x ray requesting of a well established triage nurse requested radiography system in our A&E department.
Methods
SETTING
The study was carried out in the A&E department of the Norfolk and Norwich Hospital. This is the principal hospital of the Norfolk and Norwich Healthcare NHS Trust. The main A&E department sees 59 000 new patients per year; we do not under normal circumstances accept or lodge direct general practitioner to specialty referrals.
Triage is performed on arrival, using the British Association for Accident and Emergency Medicine national triage guidelines, developed by the Manchester Triage Group.3 Patients with limb injuries may then be sent for radiography by the triage nurse before medical or ENP assessment, according to protocols developed by the A&E and radiology departments. On return from x ray, they assume their “place in the queue” according to triage category and time of arrival (fig 1).

Diagrammatic representation of patient progress; group A refers to patients allocated to the nurse and group B the control (doctor/ENP) group.
DATA COLLECTION
Data were collected over two separate periods of two weeks each. The weeks were chosen to be in the middle of our senior house officers' six month attachments, thus ensuring that the doctors involved in the study were “of average experience” for British A&E senior house officers (SHOs).
All patients who presented to the department during the study period and who were eligible for a nurse requested x ray according to our departmental guidelines (table 1), were entered into the study.
Patients were randomly allocated into the study group (group A) or the control group (group B) by instructions contained in a sealed envelope. The envelopes were randomised using random number tables.
The triage nurses were able to request x rays on patients allocated to group A, if they felt it was appropriate. However the triage nurse was not allowed to request an x ray on patients allocated to group B, even if she/he would have done so under normal circumstances. These patients were made to wait to see a doctor/ENP, before a decision was made as to whether radiography was necessary or not (fig 1). In either group, if the triage nurse judged that immediate analgesia was required, this was administered according to current protocols after consultation with the SHOs or ENPs while the patient was waiting for radiography or formal SHO/ENP assessment. For each patient in the study the following information was collected:
Triage category.
If an x ray had been requested.
The time at every stage through the department: triage, doctor/ENP consultation, time finished in the x ray department, review by the doctor/ENP, and time the doctor/ENP had finished making their assessment.
The time needed for treatment after a diagnosis had been made was not recorded, as this was considered irrelevant to the study, as we were concentrating on the time saved before “decision to treat”.
The part injured.
Whether the x ray had a positive finding. This was defined as a fracture or dislocation (our department does not have a protocol, which allows triage nurses to request x rays for foreign bodies). Scaphoid injuries were excluded from this analysis as it is difficult to know whether there is a fracture present from radiography alone.
Whether further x ray views were needed.
In order to identify missed fractures, the computer records of 100 patients from the study groups were checked to see if they had reattended the department in the one month after their initial attendance.
For the purposes of this study doctors and ENPs were considered as a single group, distinct from triage nurses. This assumption was separately validated in a study comparing the x ray request rate and results of ENPs and doctors who were involved in the study.
Analysis of the results took place using spreadsheet and statistical software packages. Continuous data was analysed using the Mann-Whitney U test and categorical data using a χ2 test.
Results
Three hundred and thirty five patients were randomised to group A and 340 were randomised to group B. Thirty two group A patients and 31 group B patients were excluded from data analysis. The reason for all the exclusions was improper completion of the study proforma. After these exclusions, data for 303 patients in group A and 309 patients in group B were analysed.
Groups A and B were shown to be broadly similar by triage category and site of injury (tables 2 and 3).
Patients entered into the study; group A refers to patients allocated to the nurse and group B the control (doctor/ENP) group
Numbers of x rays requested by nurse or doctor, with result, by site of injury; group A refers to patients allocated to the nurse and group B the control (doctor/ENP) group
Ninety five per cent of patients entered into the study were of triage category 4. The number of patients in other triage groups was 31 in total. Because of this small number, the analysis of these groups has not been documented here.
For the purpose of this study, doctors and ENPs have been treated as one group. We validated this assumption by comparing the x ray requesting behaviour of doctors with ENPs. The x ray request rate was 76% in both groups and the percentage of x rays with a positive finding was 44% compared with 50%, with a higher positive hit rate for ENPs. The ENPs have all undergone recognised national training courses. All are of grade F or above and have extensive A&E experience. The higher “hit” rate is probably explained by the fact that they were using broadly the same protocol as the other nurses, and certain requests are not permitted—for example knees. In addition, ENPs work alongside the doctors, and will see patients after triage nurse requested radiography in the same way.
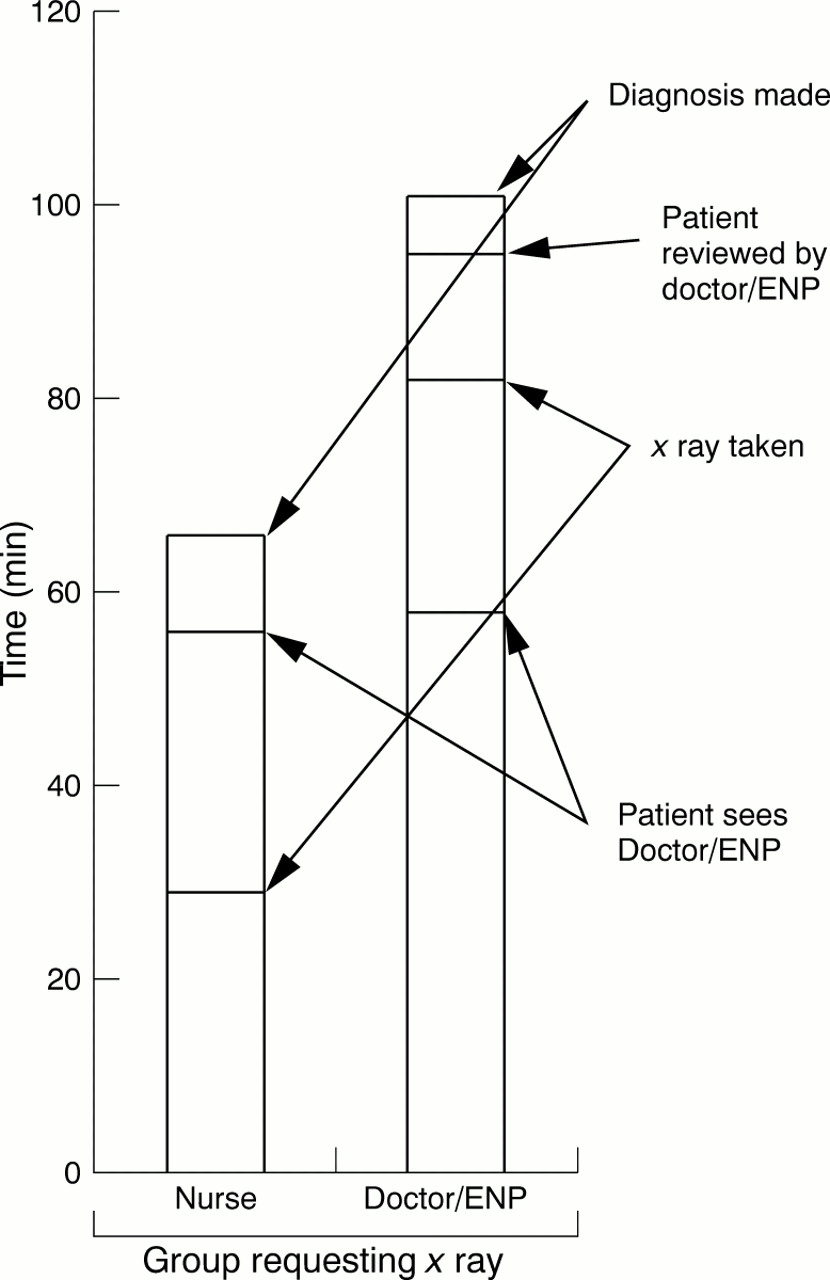
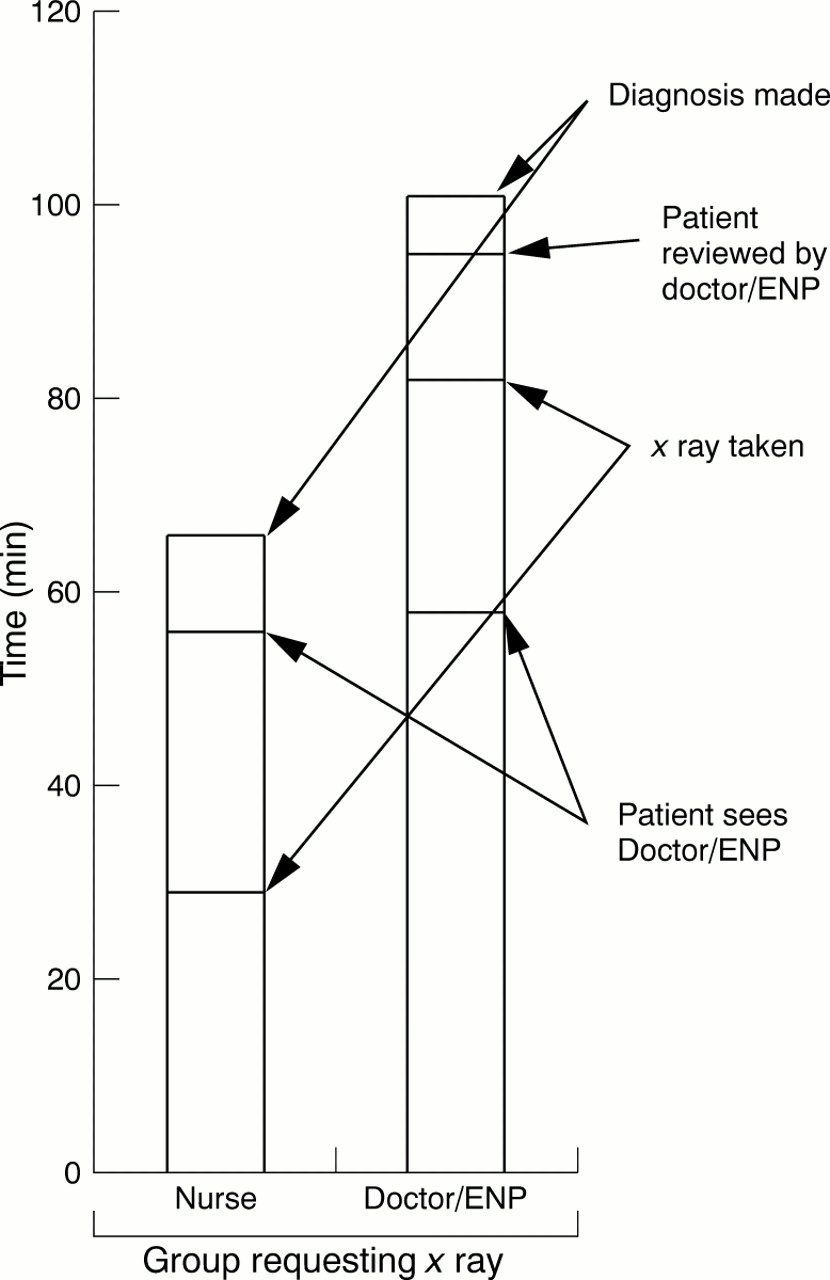
The steps in the triage to treatment decision pathway for each group are illustrated in fig 1. The mean total time for patients from arrival in the A&E department to when the doctor/ENP had finished assessing their injury was 65.5 min (95% confidence interval (CI) 60.5 to 70.5) for patients allocated to the nurse (group A) and 102.7 min (95% CI 96.4 to 109.0) for those in the doctor/ENP (control) group (group B) (fig 2). This represents a (36%) time saving of 37.2 min (95% CI 30.2 to 44.2) for patients who had nurse requested radiography (p<0.000, Mann-Whitney U test).
{kind=link}
{kind=link}
Patient progress and mean waiting times at each stage.
By contrast, patients in whom no x ray was requested in either group had almost identical transit times through the department (group A 64.4 min, group B 63.7 min, difference p = 0.79, Mann-Whitney U test).
It was noted that the time from triage to first being seen by a doctor/ENP was the same for both groups, regardless of whether they had a nurse requested x ray while waiting. The breakdown of the patient's passage through the department is illustrated in fig 2.
Two hundred and eight (68%) patients in group A had an x ray requested by the triage nurse. This compares with 237 (76%) in group B who had an x ray requested by the doctor/ENP. Triage nurses therefore requested on average 8% fewer x rays than doctors/ENPs (p = 0.002, χ2 test).
Of those patients in group A, 26 (7.8%) subsequently went on to have radiography (or further radiography) requested by the attending doctor/ENP. The notes of each of these cases were checked to establish the circumstances.
One of these was because the triage nurse had requested the wrong view, in the opinion of the doctor; the triage nurse had requested a view of the wrist and the doctor required a view of the hand. Both views were normal.
Of the remaining 25 cases, 11 (44%) had a positive finding on radiography. Of these, five were injuries that were over one week old and one had an associated head injury. Although our protocols allow triage nurses to x ray old injuries, they are taught to be cautious of doing so. The triage nurse for the case with an associated head injury suspected a skull radiograph might also be requested for the patient (which it was). Our protocols exclude skull radiographs from the nurse requested system. The patient was therefore not sent for x rays of his limb injuries, in anticipation of a repeat visit to the x ray department. In the remaining five cases, who turned out to have a positive finding on radiography, there was no obvious reason for the failure to request radiographs.
Of the 14 cases in group A who were x rayed on the doctor/ ENP's request, but who did not have a positive finding, three were over 1 week old and three were assessed as not needing an radiography according to the Ottawa ankle rules by the triage nurse.
Of those x rays that were requested, 113 (54%) in group A and 113 (48%) in group B had a positive finding. This demonstrates that x rays requested by the triage nurse had a 6% greater chance of having a positive finding than those requested by the doctors (p = 0.03, χ2 test).
Discussion
This study indicates that the system of triage nurse requested radiography in our department results in a saving of 37 minutes per patient, in other words, a 36% reduction in pre-treatment time spent in the department. This is supported by audits from other departments,4 many of which report a quicker transit time for patients; time saved has been quoted as being between 20 and 39 minutes.
From our experience after analysis of comments from our patients, the time spent waiting when there is a perceived lack of activity or attention is more important than time spent during active treatment. We wish to emphasise that the quoted statistics refer to the delay before diagnosis and not the total time spent in the department.
In addition we have shown that nurses can be trusted to request x rays appropriately. They have a lower request rate, and a higher positive hit rate, than the doctors/ENPs with whom they were compared. The x ray request rate and positive hit rate for our doctors and nurses compares favourably with previously reported figures.2, 5, 6
There is a different emphasis for nurses requesting x rays; they do not have to take responsibility for treatment decisions made about a patient. The emphasis for triage nurses is placed on confirming fractures or dislocations; this differs from the pressures on doctors and ENPs, who may request an x ray to exclude pathology. Nurses can therefore afford to radiograph only those patients who are likely to have a fracture or dislocation, thus accounting for the lower radiography request rate and the higher positive hit rate. It is also how the system should function.
After their x ray, a doctor or ENP then reviews all patients. A patient who does not have an x ray requested by the triage nurse, but is subsequently sent to x ray by a doctor/ENP, is in the same position as if the system of nurse requesting did not exist (that is no net loss or gain in time spent in the department). However, if a triage nurse requests radiography that would not have been requested by the doctor/ENP, the patient will have been unnecessarily exposed to radiation in addition to the costs of the x ray to the department. Therefore, nurses should be encouraged to be frugal with their x ray requesting, to avoid an excessively high x ray rate.
Not all previous publications have been in favour of triage nurse requested x rays. A study by Thurston and Field showed a net mean time saving of only four minutes per patient and an x ray over request of 6%.2 They concluded that nurse requested radiology was of no value to A&E departments. However their study involved nurses with variable experience in x ray requesting (personal communication). We suspect the reason their study showed no advantage of the system was due to the inexperienced staff and the protocols used.
Two other studies showed a time saving of between six and 19 minutes in transit time through the department per patient.7, 8 Despite only moderate time savings, they both supported the continuation of nurse initiated radiography because of the high staff and patient satisfaction associated with the change in procedure.
As a consequence of carefully designed protocols, a one day training programme, and seven years of acquired experience, the system in our department reduces the overall waiting time for patients and enhances the quality of our service. In addition, it is well received by patients, doctors, ENPs, and nurses alike. The team working in the department has been enhanced and there has been better communication between the A&E service and radiology. We plan to continue and further develop the system.
Conclusion
This study demonstrates significant potential advantages to A&E departments of adopting a triage nurse requested x ray system. A 36% pre-treatment time saving for patients and advantages in patient and staff satisfaction was achieved, with no decrease in quality of x ray request or quality of service.
Clearly, the time saved applies only to the group of patients who are eligible for nurse requested radiography—that is approximately 25%–30% of walking wounded patients. Other strategies exist to attempt to reduce waiting times for other groups of patients.
Acknowledgments
We acknowledge and thank the nursing and medical staff of our department. We also gratefully acknowledge the support of the radiology department without whom our system could not operate.
Footnotes
-
Conflict of interest: none.
-
Funding: none.