Article Text

Abstract
Objectives—The Royal College of Surgeons (RCS) Report on the management of patients with head injuries under the chairmanship of Professor Galasko, published in June 1999, made important recommendations that will have a profound effect on the organisation of management of head injuries and major implications for resources. The Eastern Region carried out an audit study to determine the provision of current services available, to assess the shortfall and likely resource implications for the implementation of the report and hence lay the foundations for a strategic plan for change across the region.
Methodology—A series of interviews with all 20 accident and emergency (A&E) departments across the Eastern Region and the two regional neuroscience units (RNU) was undertaken. The results of the survey and the implications of the implementation were fed back to and discussed at a multidisciplinary regional seminar.
Results—There is considerable variation and major deficiencies in the service provision currently available for the management of head injuries in the Eastern Region. There are major deficiencies in A&E resources, care of moderate head injuries and rehabilitation and follow up of patients. There is a significant shortfall in resources for the implementation of the recommendations.
Conclusion—There are major deficiencies in the overall management of head injuries. Although the RCS Galasko Report recommendations were agreed to be very desirable, they cannot be implemented without a large increase in resources in terms of funding, staffing and training.
Statistics from Altmetric.com
“The maintenance of the status quo in the provision of services to patients with head injuries is not a viable option.”*
In June 1999, the Royal College of Surgeons (RCS) in England published the Report of the working party on the management of patients with head injuries under the chairmanship of Professor Galasko.1 The report's recommendations will have a profound effect on the organisation of the management of head injury and important implications for the resources (both staffing and physical) in accident and emergency (A&E) departments, observation wards, neuroscience, neurointensive care and rehabilitation units. In February 2000, a second report, Safe neurosurgery2 from the Society of British Neurological Surgeons was published; its recommendations include emphasis on strategic resource, service and workforce planning, standards for neurosurgery and information, audit and clinical governance issues.
To make the connection between these two important national reports and the action required, the Eastern Region Specialised Commissioning Group (ERSCG) worked closely with the Academic Neurosurgery Unit at Addenbrooke's Hospital in Cambridge and the Essex neurosciences centre at Oldchurch Hospital, Romford. In February 2000, the Eastern Region started a Head Injury Resource Audit Study to assess the resource implications and to produce a strategic plan for change across the region. The overall objectives of the study are:
-
To determine the current provision and pattern of care pathways for patients of all ages seen in A&E departments after head injury with and without multiple trauma.
-
To look at current resource utilisation at various stages of care of such patients.
-
To determine the likely pattern of future resource utilisation in the event of adoption of the guidelines of the RCS.
Three methods are being used to achieve the above objectives. A retrospective review of statistics and management of all patients with head injuries admitted to Addenbrooke's Regional Neurosurgical Unit (RNU) in 1999 was carried out to provide an understanding of the perception of severity of head injury and reasons for transfer. The second method, of which this is a report, was a series of interviews with A&E departments followed by a multispecialty feedback seminar. Finally, prospective audits during the implementation process are planned to provide quantitative data with regard to epidemiology and resource utilisation and will be conducted at Addenbrooke's and selected district general hospitals (DGHs).
Methodology
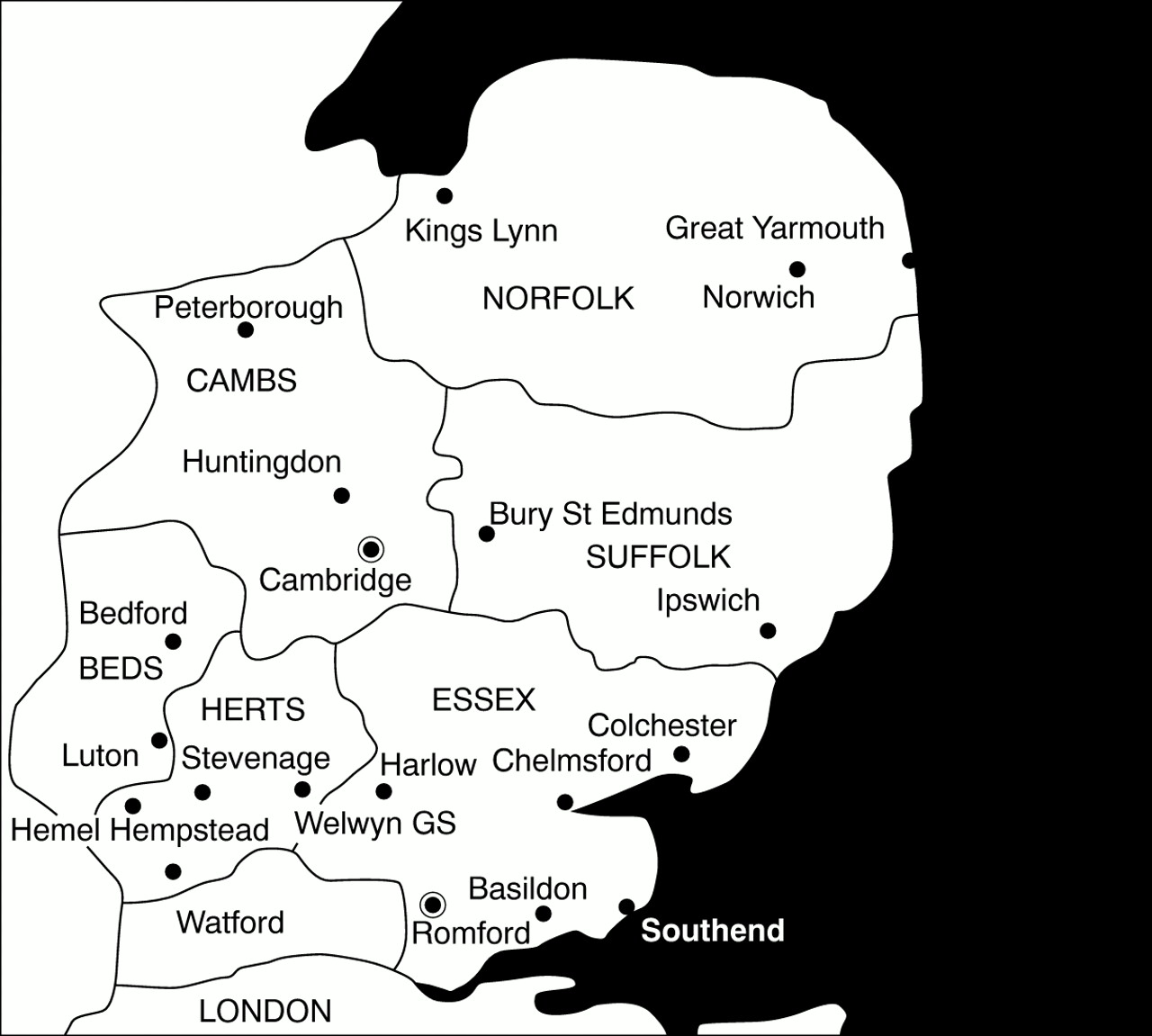
The Eastern Region (fig 1) covers six counties, and serves a catchment area of around 5.4 million people. There are 20 acute hospital trusts with major A&E departments, all receiving patients with head injuries. The 20 departments are led by 42 A&E consultants. In 1999 there were 1 221 000 new patient attendances. The RNU at Addenbrooke's Hospital receives head injury patients from 9 of 10 DGHs in the northern part of the region (serving Cambridgeshire, Norfolk, Suffolk and Bedfordshire). In 1999, 246 patients with head injuries were admitted to Addenbrooke's RNU. The RNU at Oldchurch Hospital is one of the neuroscience centres serving six DGHs in Hertfordshire and Essex in the south of the region. The remaining southern DGHs refer to either Cambridge or London RNUs.

{kind=link}
Map of Eastern Region with its 20 acute hospital trusts and A&E departments and two regional neurosciences units.
Accurate statistics on the number of patients with head injuries attending the 20 A&E departments in the region are not available. We estimate, however, that there are 14 000 patients needing inpatient hospital admission assuming similar incidence as other studies.3 We estimate, 500 would be severe head injuries (Glasgow Coma Scale (GCS) 3–8), 650 moderate (GCS 9–12) and the remaining 12 850 mild (GCS 13–15).
After discussions with the Academic Neurosurgery Unit at Addenbrooke's Hospital, chief executives of NHS Trusts within the region were initially contacted by the clinical director of the ERSCG (GC), in January 2000 in the form of a general letter. This provided background information and reasons for the proposed study, emphasising its importance. Organisation of meetings with A&E consultants was begun in February, 2000. A&E consultants were contacted by HMS and sent background information as to the purpose of the study and the interviews. They were asked to inform and invite any other key clinicians in the management of head injury at their hospital, for example, general and orthopaedic surgeons, general physicians, feriatricians, paediatricians, ITU/anaesthetic consultants and rehabilitationists.
Twenty interviews in all were held at all the DGHs including the two hospitals with the RNUs. JDP, GC, and HMS conducted the interviews in the north of the region, and JK, GC, and HMS in the south. JDP and JK visited each other's units. Each meeting typically took about one to two hours entailing face to face discussion with key clinicians following a semistructured interview format. A proforma was used that covered key questions concerning current arrangements for assessment, computed tomographic (CT) scanning, admission, transfer, rehabilitation and follow up of head injured patients, as well as resource implications of implementing the RCS Report recommendations. The British Association of Accident and Emergency Medicine (BAEM) Report Implementing the Galasko Report on head injury care—implications for A&E departments4 was used to define adequate resource requirements in A&E departments (box 1). Other issues considered were review of documentation, record keeping, communication with the neurosurgical service, responsibilities, and the sequence of decision making. After the visit, each hospital was sent a draft report of their interview to check for factual correctness and to make any further comments.
Findings from each hospital visited were analysed, summarised and compared and the resulting report formed the basis of discussion at a multispecialty feedback seminar entitled, Head injury—time for change. It was attended by 82 people: 29% A&E senior medical, 12% neurosurgery, 27% rehabilitation, 27% other specialist staff and 11% other key personnel in trust and health authority management. The objectives of the seminar were to disseminate the findings of the survey and to discuss the consequences for the planning process by highlighting in systems terms the blocks, deficiencies, delays and difficulties. It was also hoped the seminar would enable exploration of proposed solutions in terms of workforce, collaborative communication systems, records, electronic and written guidance and aspects of clinical management of head injuries.
The seminar covered all the stages of head injury management, with reports on the experiences of an already operational observation ward at Addenbrooke's Hospital, the impact of neurointensive care on head injury outcome and the implications for the management of head injury. The current management of moderate head injuries was discussed extensively as there were many concerns. The implications of the survey findings for A&E departments, neurosurgery and rehabilitation were also specifically discussed. Many of the issues raised during the seminar complemented those in the survey findings.
Findings
The following is a synopsis of the results of the survey and the discussions of the seminar. The results of the survey are grouped into seven key areas based on the interview and key recommendations from the RCS Report. Tables 1A and 1B show the current resources and facilities available in the northern and southern parts of the region respectively. Table 2 is a description of the current situation, as found, in the whole region. We summarise the findings below.
Summary of current resources for head injury (HI) management
1 A&E DEPARTMENTS: ROLE, FACILITIES, AND RESOURCES
RCS Report recommendation: Consultants in A&E medicine should have responsibility for initial assessment of and decision-making regarding all patients with head injuries (page 2).
All 20 hospitals meet this recommendation.
RCS Report recommendation: “a period of training in neurosciences should be an integral part of the higher specialist curriculum of the CME of all A&E consultants” (page 37) and “Management of head injuries is a recommended part of the training of doctors in A&E medicine”. (page 2)
At 70% of the hospitals, A&E consultants had some experience in neurosurgery as part of their training and background. All specialist registrars in the Anglian Deanery receive a minimum of two months training at the RNU in Cambridge. There are no formal courses however that will provide continuing medical education on head injury management for senior staff.
RCS Report recommendation: “Patients with minor head injuries who require admission to hospital for observation for up to 48 hours should be admitted under the care of the A&E department to a short stay observation ward. (page 2) . . .and should no longer be admitted under the care of general and orthopaedic surgeons.” (page 3)
At only three hospitals visited were minor head injured patients, who require observation for up to 48 hours, admitted under the care of the A&E department. Another two A&E departments were scheduled to open observation wards at the end of 2000 and manage minor head injury patients (both hospitals have done so by January 2001). Three hospitals have plans for an observation ward, but there are concerns that the necessary increase in both medical and nursing staff would not be funded (in two the funding has been agreed but in one funding has not been agreed as yet). This problem was apparent in two other hospitals where observation wards remain unused because of lack of staff.
RCS Report Recommendation: “The Observation Ward must be within or adjacent to the A&E department, be adequately resourced, appropriately staffed (both medical and nursing) and have a time limit of 48 hours.” (page 3)
A&E consultants were asked about the adequacy of staffing resources in their departments, based on the BAEM recommendations in The way ahead document of 1998.5 Of 20 hospitals, six felt they currently had an adequate number of consultants (30%), five adequate middle grade medical staff (25%) and five adequate nursing staff (25%). Only 20% (4 of 20) of A&E departments visited currently have three or more consultants as recommended in the BAEM report4 (box 1). Currently there are 42 consultants in the region. To achieve the levels recommended a minimum of 30 more consultants (an increase of 71%) are needed—12.5 more in the north of the Region and 17.5 in the south. Similar findings were recorded for junior medical and nursing staff. In 19 of 20 hospitals (95%) the A&E consultants agreed to manage head injuries given adequate resources as proposed by the BAEM Report (box 1). In half of the hospitals, there would be no space for an observation ward. A number of A&E consultants expressed concern as to the advantages, usage and resource implications of an observation ward in A&E.
2 CT, ON CALL RADIOLOGISTS, AND IMAGE TRANSFER
RCS Report recommendation: “Hospitals receiving patients with head injuries must have 24-hour CT head scanning, on-call radiologists and image transfer facilities to their named neurosurgical unit.” (page 8)
Emergency use of CT for head injuries has potential advantages: the possibility of early investigation of more patients can lead to “more rapid detection and neurosurgical treatment of intracranial complications, and conversely of avoiding inappropriate transfer to neurosurgical units” (page 57). There are therefore important implications for the subsequent progress and outcome of the patient.
All hospitals visited had 24 hour availability for CT seven days a week (100%). However, 35% (seven) of the hospitals reported problems in accessibility, caused by either lack of resources or liaison/communication problems in the request system in place. At three hospitals, insufficient radiologists affected accessibility. In two hospitals problems in liaison with the radiologists were reported, but in two hospitals consultant request for CT scans is not needed, and these delays were not experienced. Eighteen of 20 hospitals visited now have image transfer available (90%) and a new system to be installed in 2001 will link the 19th hospital to its RNU. Accessibility however was impaired by the unreliability of the system at five hospitals.
All A&E departments visited had written protocols for CT. Ten hospitals use the East Anglian guidelines, six the RCS, two the Advanced Trauma Life Support (ATLS) and one the National Hospital for Neurology and Neurosurgery, Queen's Square, guidelines.
3 REFERRAL AND TRANSFER TO NEUROSURGICAL UNITS
RCS Report recommendation: “Each A&E department should establish close relationships with a single named neuroscience unit to which patients needing neuroscience input should be referred `in all but exceptional cases,” (page 8, page 40).
The named neurosciences unit for the north of the region is Addenbrooke's, Cambridge, except for the Luton and Dunstable who refer to the Royal Free, London. In the south (Hertfordshire and Essex), Oldchurch, Romford is the neuroscience unit for six hospitals, the Royal Free for three, and the National Hospital for Neurology and Neurosurgery, London, for one. Ten hospitals reported problems, including lack of bed availability and liaison difficulties at their named neurosciences unit. Thus 50% would meet the RCS Report recommendation. Other neuroscience units used because of lack of bed availability were in Oxford, Nottingham, and London. All A&E consultants at the hospitals visited are able to refer patients directly, except at one hospital, which preferred not to because of repatriation problems. The orthopaedic and general surgical registrars in three other hospitals also refer the patients for the same reason.
RCS Report recommendation: “Transferred patients are to be resuscitated and stabilised, intubated and ventilated for transfer and accompanied by a senior anaesthetist” (page 8).
Sixteen of 20 hospitals (80%) reported appropriate transfer of patients. The four reporting problems were all in the south of the region and the difficulty was understaffing in the anaesthetic department. Two hospitals reported liaison problems in the transfer process. All hospitals had written guidelines for referral and transfer. The transfer journey times are shown in tables 1A and 1B. The mean transfer journey time for all hospitals was 40 minutes.
4 CARE OF INTERMEDIATE HEAD INJURIES
RCS Report recommendation: “A&E departments should admit and supervise head injured patients for up to the first 48 hours' (page 2)... “They should no longer be admitted under the care of general and orthopaedic surgeons” (page 3) and those who require continuing care (ie. inpatient stay greater than 48 hours), should be the responsibility of the neurosciences departments” (page 3).
The RCS Report's definition of intermediate head injuries is: “Patients with a head injury who are admitted to hospital for more than 48 hours but who do not require intensive care and who do not require surgery” (page 15). At present, in 18 of the 20 (90%) hospitals visited, patients requiring continuing care exceeding 48 hours are cared for by either general or orthopaedic surgeons, based on local tradition, and at one hospital, by the A&E consultant. At only one hospital, Addenbrooke's, which is also a regional neurosciences centre, were these patients cared for by the neurosurgeons, as the RCS Report recommends (5%). There was no particular interest, expertise or lead in head injury management found among general or orthopaedic surgeons except one general surgeon. There were no designated wards or beds for head injuries except at the 2 RNUs and one DGH. Such patients were placed on general surgery or orthopaedic wards. Often, head injured patients are outliers. Six hospitals (30%), had written protocols for care and discharge of intermediate head injured patients. Only two hospitals (one RNU and one DGH) provide any continuity of care or follow up for these patients.
5 CHILDREN
RCS Recommendation: “All children (<16 years) requiring admission . . .should be admitted under the care of a paediatrician or paediatric surgeon trained in the care of children with head injuries” (page 5)
In 14 of 20 hospitals visited (70%), paediatric head injuries are looked after by paediatricians, paediatric surgeons, or jointly with another specialty, although all were placed on a paediatric ward. At other hospitals, children were cared for by the same specialty as adult head injuries. At all the hospitals visited, non-accidental injuries were admitted under paediatrics. The cut off age for paediatrics varied slightly from 10 to 16 years, the latter being in the majority. Only one paediatric department had a particular interest and expertise in acute and post-acute head injury rehabilitation. Generally speaking, in the north of the region, Addenbrooke's is the main receiving neurosciences unit for paediatric head injuries and in the south, Great Ormond Street. Other centres used by the 10 hospitals in the south of the region were the Atkinson Morley and St Mary's. Few problems were identified concerning severe head injured children needing to be transferred to a neuroscience unit. The lack of paediatric intensive care facilities at Oldchurch, the Royal London and the Royal Free meant greater delays in transfer occasionally for hospitals in the south of the region.
6 ELDERLY PATIENTS
RCS Report recommendation: “Elderly patients who do not require surgical intervention but are not fit for discharge after 48 hours should be transferred to the care of the local Department of Medicine for the Elderly where there should be input from the local neurologist and rehabilitation unit where appropriate” (page 5).
At 4 of 20 hospitals, elderly head injured patients are admitted to and cared for by geriatricians and at a further four, patients, where appropriate, would be transferred to the care of the geriatricians. (40% meet the RCS recommendation). At the other hospitals, elderly head injuries were admitted, as were other adults to either general surgery or orthopaedics, according to the tradition of the hospital. Two hospitals had no geriatrician, and in a further 10, there was no particular interest or expertise in management of head injuries. Rehabilitation facilities for elderly head injured were available at five hospitals.
7 REHABILITATION AND FOLLOW UP
RCS Report recommendation: “Post acute rehabilitation of head injured patients should not be managed on acute neurosurgical, general surgical, orthopaedic, or general medical wards . . . They require the expertise of trained rehabilitationists working in an adequately-resourced multidisciplinary rehabilitation unit” (page 11). “Referral for rehabilitation should be at as early a stage as possible and a specialist rehabilitationist involved, as this is important in the prevention of late complications” (page 33)
Both post acute and long term rehabilitation services to adults, the elderly and children were considered by those interviewed to be inadequate compared with the RCS report, and often with no formal structured system or service provision. A limited post acute rehabilitation service was provided at four hospitals. A limited long term rehabilitation service was provided at five hospitals. At two hospitals there were consultants with interest and expertise in long term rehabilitation of head injured patients and a third was served by a good community neuro-rehabilitation team, but again, there were gaps in the service. Very few appropriate rehabilitation units were identified in the region by those interviewed, who perceived that there were few suitable placements for head injured patients with behavioural disorders, but centres of excellence, including dedicated neuropsychologists, were identified (for example, the Lewin Unit, Cambridge, the Oliver Zangwill Unit, Ely, the Colman Hospital, Norwich and Icanho, the Suffolk Brain Injury Rehabilitation Centre, Stowmarket). Five hospitals had links, of varying strength, with Headway, the voluntary organisation for head injured patients and their carers.
RCS Report recommendation: “All patients attending hospital with a head injury should be followed up, initially by their G.P., including those with minor head injuries who did not require in-patient admission” (page 5) . . . “according to local arrangements which should be established” (page 34).
No formal systems of follow up were found for patients with minor head injury who were not admitted. These patients are simply given written advice and told to see their GP if any problems occur. There were no head injury follow up clinics for minor head injuries admitted, except at one hospital, where these patients are followed up by an A&E consultant. Head injury clinics at two hospitals were discontinued because it was felt they were counter-productive and/or inappropriate. There is some debate over the appropriateness of follow up for minor head injuries.
RCS Report recommendation: “All adult patients with intermediate and severe head injuries should be followed up. . . .The minimum follow-up is a neurological and neuropsychological assessment which should be undertaken two to three months after injury” (page 5).
Again, the only follow up for intermediate head injuries was offered at two hospitals. Severe head injuries treated at Addenbrooke's are followed up by the neurosurgery department, in collaboration with the Lewin Unit or Colman Hospital where appropriate. This includes some of those patients from DGHs in the region who were transferred. Long term follow up within the community is again a patchy and poorly resourced service, heavily dependent on voluntary organisations and lacking any formal structure.
RCS Report recommendation: “Community paediatricians or community Paediatric nurses should follow up children following admission for head injury.” (page 6)
A similar situation was found across the region for paediatric head injury follow up.
Discussion
The findings of this study show considerable variation and major deficiencies in the service provision currently available for the management of head injuries in the Eastern Region. The study highlighted significant shortfalls in resources for the implementation of the recommendations of the RCS Report. Table 2 clearly shows major deficiencies in A&E resources, care of moderate head injuries and rehabilitation and follow up of patients. The reality is a long way from the standards and recommendations of the report. All the participants in this exercise agreed that the current situation was unacceptable in many areas and that the recommendations of the Galasko Report, although very desirable, could not be implemented without a large increase in resources in terms of funding, staffing and training. Also, some of the proposals, such as care of intermediate head injuries, would need more discussion of their feasibility and implications for planning.
A&E ROLE AND RESOURCES
Minor head injuries (GCS 13–15 and admission <48 hours) were under the care of A&E staff in 3 of 20 hospitals in the region in April 2000 and 5 of 20 as from January 2001 (see table 2). In two hospitals, observation wards remain closed because of lack of funding. Adequate A&E staffing at all levels are currently available in only two hospitals (10%). Most A&E consultants in the region (95%) would agree to manage minor head injuries given adequate resources. However, it would be impossible to take on this role without the resources. The minimum requirements recommended by the BAEM are listed in box 1. The study highlights the shortfalls and the additional staffing and facilities that would be required. For example, an extra 30 consultants are needed to achieve the recommended levels, representing a 71% expansion from current levels.
The expertise and training is already partly in place: emergency medicine is the only specialty, apart from neurosurgery, where there is formal training for registrars and consultants in head injury care. In 70% of A&E departments, one or more consultants had had some training in neurosurgery as registrars. The Anglia A&E specialist registrar training programme has now introduced a three to four month full time secondment at the Addenbrooke's RNU. This will ensure that all new A&E consultants will be trained in the management of head injuries. There is a need however for continuing medical education for senior medical staff to maintain their skills and to ensure uniformly high standards of care. In June 2001 a one day course was organised at Addenbroke's Hospital for senior A&E staff as recommended by BAEM.4
Galasko recommends that minor head injuries requiring admission should be looked after in an observation ward. Box 2 summarises what we believe to be the essential requirements for an observation ward. This is based on three years' experience at the Addenbrooke's A&E department and the consensus achieved through discussions at the seminar. In addition, strict protocols and structured care pathways would need to be in place to ensure adequate management of all head injuries (and in particular moderate head injuries), including rehabilitation and follow up. The establishment of an observation ward would achieve additional benefits: other short stay patients could be cared for here. The ward would function as an extra resource and safety net for A&E and the hospital. It would improve teaching and training of A&E staff and increase the acute bed capacity in a hospital as recommended by the National Bed Enquiry6 and hence lead to better utilisation of elective ward beds.
MODERATE HEAD INJURIES
The care of this category of patients gives rise for concern. The study found that in only two hospitals were there designated beds for these patients and their management was often unsatisfactory in that there were no clearly defined care pathways and little interest or expertise in head injury management among surgeons.
The RCS Report recommends that such patients should be the responsibility of clinical neurosciences. Issues such as increase in workload, the necessity and appropriateness of the care of all patients with LOS >48 hours being supervised by neurosurgery, would need to be resolved. The survey findings were compounded by an audit carried out by general surgeons in one of the DGHs of the region where 73% of head injured patients under their care were social admissions. A recent survey from Glasgow7 shows that only 17% of all head injury admissions remain in hospital for more than 48 hours and of these only 20% stay because of head injury alone. The remaining patients had other comorbidities or social reasons necessitating further hospital stay. Therefore, it seems that this recommendation is not realistically achievable, and not in fact necessary, given the current restraints in NHS funding and the large number of issues in health care provision in the UK competing for limited resources.
The problem of moderate head injuries can be broken down into a more manageable size by dividing the group into three categories: paediatric (<16 years), adult (16–64 years), and elderly (65 + years). Children will receive a reasonable standard of care under the paediatricians, and the often multiple problems of the elderly are more effectively looked after by physicians expert in the care of the elderly. Of course, all of these patients may benefit form neurorehabilitation. The needs of the adult group need to be tackled at different levels.
The organisation of regional neurosurgical facilities and responsibilities is based on “hub and spoke” arrangements to be replaced by service frameworks. Such an arrangement is already in place and is one of the strengths of the current service. This concept could be fostered and developed further for the benefit of patients with moderate head injuries by developing regional and or national guidelines, streamlining communications (expose the barriers, for example, phone advice), increasing neurosurgery sessions in the DGHs including neurosurgery opinion for moderate head injury inpatients, organising training programmes and study days on head injury management and establishing care plans at each stage of head injury management. Assistance and involvement of the RNU will foster a sense of partnership. Such programmes are already partly in place but are rather ad hoc.
At the same time measures can also be put in place that will enhance existing arrangements and improve the care of moderate head injury patients. The following measures or suggestions have been discussed: identifying clear responsibility for care that might vary at each hospital according to the current situation. There are suggestions to develop a multidisciplinary team headed by a head injury coordinator or lead consultant with an interest in head injury that will take over the care of this group. Another suggestion was to utilise the neurologists. Such a multidisciplinary team would also assist in improving the post acute rehabilitation service.
The development of clear care pathways with identification of the appropriate patients and written protocols, to include those patients who return from RNUs for rehabilitation would be helpful. The care of these patients would be facilitated by designated head injury beds or “clustering” of patients. Some of the above measures could be achieved by reorganisation but there are resource implications for their implementation.
REHABILITATION
The study showed a similar picture of inadequate service and resources in this area but a detailed assessment of the extent of the problem was outside the remit of this study. There was a general consensus of opinion on the need for greater continuity of care through integrated, interdisciplinary care pathways at both post acute and long term rehabilitation stages. The development of a multidisciplinary team led by a consultant with an interest in rehabilitation was thought to be an essential requirement that will bridge the existing gap and improve the service. The team should include nurses, occupational therapists, clinical psychologists, physiotherapists and perhaps a head injury coordinator. The second stage of our study includes a detailed review if rehabilitation services. In addition, the limitations of the rehabilitation and follow up of children with moderate and severe head injuries in the East Anglia Region are currently being tackled by specific proposals from Addenbrooke's Hospital for a regional solution to the problem.
Conclusion
The Eastern Region head injury resource audit study is the first regional approach in the UK towards implementing the Galasko Report. It was initiated as a proactive response to the recommendations of a report, which, if implemented, would have a profound effect on the management of head injury nationwide. It has clearly shown major deficiencies in A&E resources, care of moderate head injuries and rehabilitation and follow up of patients. The RCS Report recommendations are very desirable but without resources and refinement, the recommendations cannot be implemented. The next stage, a much more difficult task, is the implementation of the findings of this study. It is planned to take each component forward and fill the gaps in the service framework.
Box 1 Optimal resource requirements for a medium sized A&E department* (+/− 50 000 annual attendances). It is based on the reported judgement of A&E consultants
-
A one in three consultant on call rota or better
-
Two to three sessions a week of senior medical time on the ward
-
Two or more medical staff on site at all times
-
Four observation beds, preferably within a six to eight bed A&E facility
-
Two qualified nurses at all times in addition to the A&E department complement
-
24 hour computed tomography
-
24 hour on call radiologist
-
Telemetry links with on call neurosurgeon
-
Adequate neurosurgical beds—ITU, observation, postoperative and rehabilitation wards
-
Liaison meetings involving A&E, neurosciences, anaesthetics and radiology with joint production and updating of local procedures and policies
-
Good quality comprehensive discharge advice
-
Four to five clinic slots a week involving three to four hours of specialist nurse time and two hours of senior medical time
-
Access to a regional neuropsychology service
-
One day training for all medical and nursing staff, repeated every three to five years
-
One session image interpretation training for medical staff
-
Six weeks off service secondment for higher specialist trainees
Box 2 The role of observation wards in the management of minor head injuries
REQUIREMENTS
-
Adequate, dedicated, trained staff
-
Colocation with A&E department preferable
-
Closely monitored protocols for admission and discharge
-
Minor head injuries, GCS 13–15, to be admitted with LOS < 48 hours
-
Access to computed tomography, telemetry, and interpretation
-
Clearly defined care pathways for moderate head injuries (LOS > 48 hours)
-
Specific training programmes in head injury management for all staff
BENEFITS
-
It contributes to good and efficient standard of care for head injuries.
-
It is an additional A&E resource and safety net
-
It benefits the hospital
-
It improves teaching and training of A&E staff
ISSUES
-
Adequate neuroscience resources for all severe head injuries
-
Responsibility for care of moderate head injuries (placement, protocols, rehabilitation, and follow up)
-
Readily available advice from RNU for moderate head injury
Acknowledgments
We would like to thank all the A&E consultants and other staff who participated in the study and all those who took part in the multidisciplinary seminar. We would apologise to any professional groups or individuals who may perceive that this wide ranging study has failed to acknowledge their contribution to the care of our head injured patients, but there is an urgent imperative to implement the Galasko report. The prospective studies now planned for the Eastern Region will allow any omissions in this report to be corrected.
Contributors
HMS organised the interviews and the seminar, participated in the interviews and compiled the survey report. JDP, JK, and GC generated the concept of the audit and participated in the interviews and the seminar and CM participated in the seminar and wrote the paper. The guarantor of the paper is C Maimaris.
Footnotes
↵* Porter J, Swann I, et al. Implementing the Galasko Report on head injury care—implications for A&E departments. London: BAEM, June 2000.
-
↵* RCS. Report of the working party on the management of patients with head injuries. London: 1999:6.
-
Funding: H Seeley has been partly funded by the Eastern Region Specialised Commissioning Group.
-
Conflicts of interest: none.
-
The following hospitals participated in the regional study: north of region: Addenbrooke's Hospital, Cambridge, Cambs, Hinchingbrooke Hospital, Huntingdon, Cambs, Peterborough Dsitrict Hospital, Peterborough, Cambs, James Paget Hospital, Gorleston, Great Yarmouth, Norfolk, Queen Elizabeth Hospital, King's Lynn, Norfolk, Norfolk and Norwich Hospital, Norwich, Norfolk, Ipswich District Hospital, Ipswich, Suffolk, West Suffolk Hospital, Bury St Edmunds, Suffolk, Bedford General Hospital, Bedford, Beds, Luton and Dunstable Hospital, Dunstable, Beds. South of region: Hemel Hempstead Hospital, Hemel Hempstead, Herts, Lister Hospital, Stevenage, Herts, Queen Elizabeth II Hospital, Welwyn Garden City, Herts, Watford General Hospital, Watford, Herts, Basildon Hospital, Basildon, Essex, Broomfield Hospital, Chelmsford, Essex, Colchester General Hospital, Colchester, Essex Princess Alexandra Hospital, Harlow, Essex, Southend General Hospital, Westcliff on Sea, Essex, Oldchurch Hospital, Romford, Essex.