Article Text

Abstract
Objectives: Little has been reported of the demographic and temporal variations in accident and emergency (A&E) attendances despite the importance of this information in planning services. The purpose of this paper to is to explore the variations in attendance patterns across the West Midlands region of the NHS.
Methods: The data were obtained from the A&E minimum dataset from a sample of 13 hospitals. Arrival dates and times, age, and sex of all patients attending A&E in the year from 1 April 1999 to 31 March 2000 were analysed to look at the pattern of attendance by hour, day and month, age, and sex.
Results: No differences were found in attendance patterns in respect to sex. Attendances by children under 15 years peaked in the evening between 18:00 and 19:59. In contrast, peak attendance in those over 15 years was between 09:00 and 11:59. The percentage of “out of hours” attendances in this dataset was highest in the under 1 age group (58.5%), the 15–24 age group (57.1%), and the 25–44 age group (54.6%). The highest proportion of patients attended A&E on a Monday, while the percentage of weekend attendances decreased with age. In children aged 1–14 years there were more attendances in summer than winter. In those aged under 1 and over 65 there was a winter peak with December having the most attendances.
Conclusions: No sex differences were found in the temporal attendance patterns at A&E. However, many differences were found in the attendance of different age groups. These differences are of great importance in the planning of services, and further research is required to explain the reasons behind these variations.
- demography
- attendance patterns
Statistics from Altmetric.com
There has been much work undertaken on the numerous factors that influence a person's desire to attend accident and emergency (A&E), however little has been reported on the variations in when people attend. Murphy has reduced the factors that act on a person's decision to visit A&E to the individual's perceived appropriateness of the condition, accessibility of A&E, and the availability of alternative medical services.1 These factors do not just determine a person's decision to go A&E, but also have an impact on the temporal pattern of attenders.
Those studies that have reported temporal variations have been specific to certain populations rather than all attenders. For example, studies looking at major trauma report that patients are more likely to arrive at A&E “out of hours” (between 18:00 and 08:00) or on Fridays, Saturdays, and Mondays, and that there would only be one such case a month during office hours (08:00 to 18:00) at an average A&E.2,3 For minor injuries, most patients present in the late morning and early afternoon, and only 6% present in the period from 1 am to 8 am.4 There is some evidence of monthly fluctuations in attendance at A&E. The highest incidence of major trauma has been reported to occur between May and July, with fewer cases in February and March.2 Presentations for medical conditions also vary throughout the year, for example attendances for respiratory conditions such as influenza and bronchitis tend to be higher in the winter months.5
Little is known of the demographic variation in attendances. Just as demography is an important factor in describing the variations observed in the incidence of clinical conditions, it is probable that it will assist in the explanation of much of the variation in attendance levels in A&E.
The purpose of this paper to is to explore the demographic variations in the temporal attendance patterns across the West Midlands Region of the NHS. Such an investigation has never previously been possible before because of the lack of available data from a large number of A&E departments.
METHODS
The data used in this study were obtained from the A&E minimum dataset, which is collected in computerised Acute Trusts A&E departments. The analyses were based on the data collected from 13 of the 21 Trusts in the West Midlands NHS region that operated a 24 hour A&E. All hospitals used were district general hospitals. Table 1 describes the Trusts in terms of their location—that is, whether they serve an urban or rural area, and their total A&E attendances in the year 1999/2000.
Description of Trusts used in the study
Arrival dates and times, and age and sex of all patients (new and follow up) attending A&E in the year from 1 April 1999 to 31 March 2000 were analysed. Arrival date and time indicate the time of registration in the department. Date of birth and sex were self reported. Age was calculated using the date of birth and date of arrival fields. The data were analysed to look at the pattern of attendance by hour, day and month, and by age and sex.
RESULTS
There were a total of 963 195 attendances during the study period, ranging from a low of 29 136 to a high of 146 306 at each Trust. Altogether 23 400 (2.4%) of the records were missing one or more of the necessary fields; date of birth, sex, date of arrival, and time of arrival. These records were excluded leaving 939 795 for analysis. Table 2 shows the number of attenders included in the study and the age and sex distribution.
Demographic breakdown of A&E attenders
Some 56.6% of the attenders in this dataset were male. However, there were no significant differences between the temporal attendance patterns of the two sexes, so the following results refer to differences in attendance by age.
Figure 1 shows the general attendance pattern by hour and day, using the whole years' data. This however, masks any variation in attendance throughout the year and by different age groups.
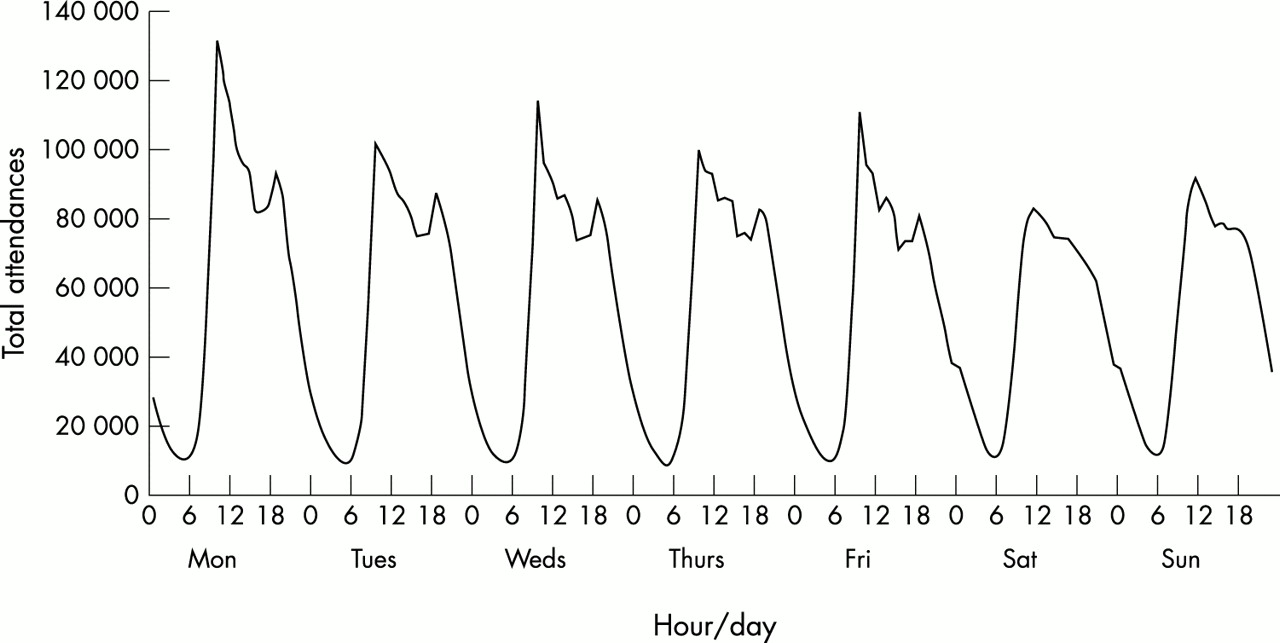
Total attendances at A&E by hour and day.
Hour of attendance
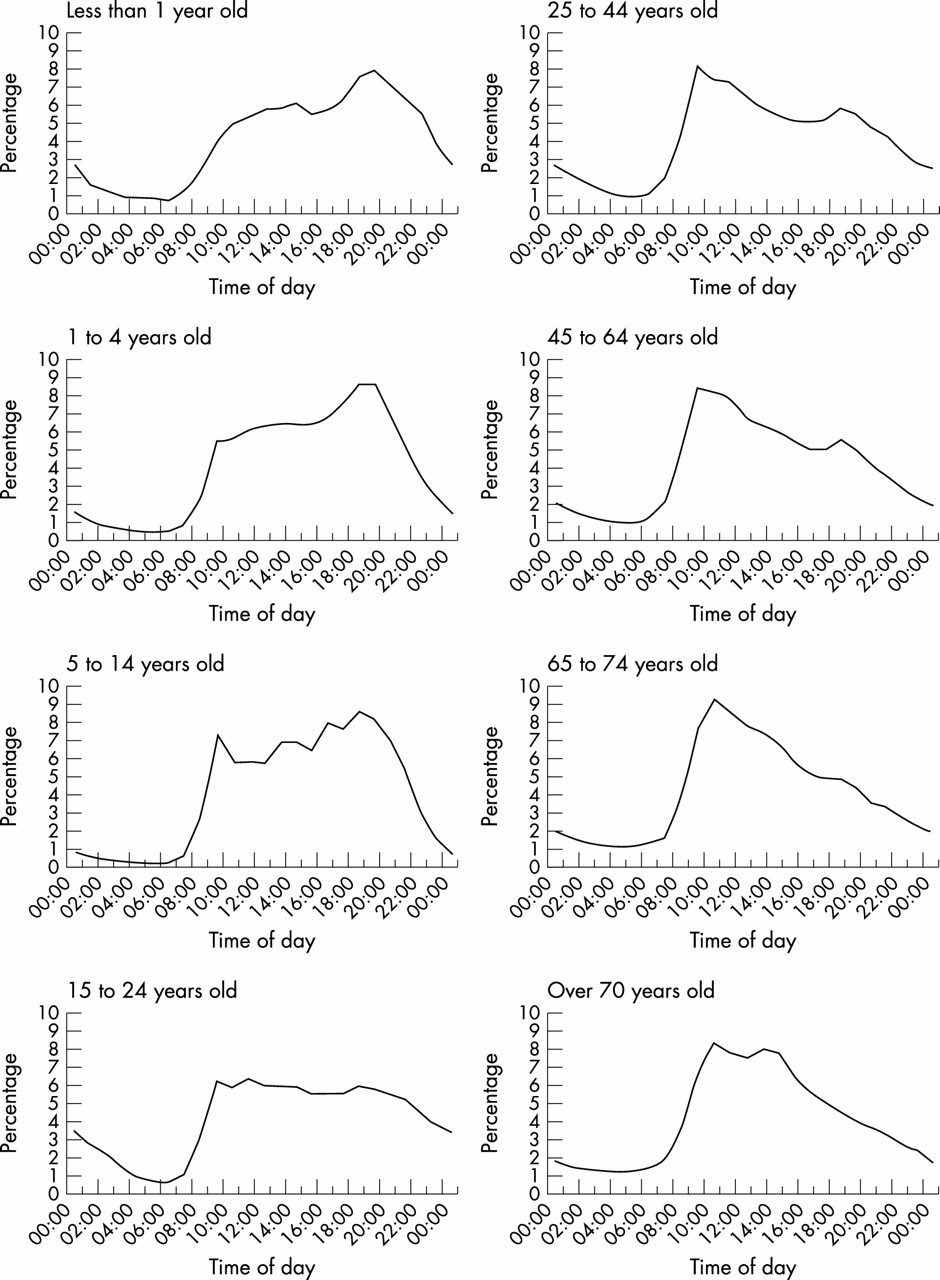
Figure 2 shows the attendance at A&E by hour in each of the eight age groups. The two youngest age groups, the under 1 years and 1–4 years had similar attendance patterns throughout the day, with peak attendance being in the early evening between 18:00 and 19:59. Attendance throughout the evening and night remained relatively high for the under 1 age group, with 48.4% of attendances being between 18:00 and 07:59. The number of 5–14 year old attenders was also highest in the early evening but the peak was less pronounced and there were more attendances in the morning than in the younger age groups.
{kind=link}
{kind=link}
Percentage of attendances within each age group by hour of arrival.
In the 15–24 year age group, attendances increased sharply after 07:00, peaking at between 09:00 and 10:59. After this peak attendances slowly declined. This age group had the second largest proportion of attendances through the night.
The 25–44, 45–64, and 65–74 age groups all followed the same pattern of a sharp increase after 07:00, peaking between 09:00 and 09:59 in the older age group. There was also an early evening peaks but the magnitude of this decreased as age increased. The proportion of people attending at night decreased with age.
Day of attendance
As can be seen from table 3 the highest proportion of patients attended A&E on a Monday. Overall 16.0% of attenders visited the department on a Monday, ranging from 14.5% to 16.6% of each age group. This trend was followed in all age groups except those aged 1–4 years, where majority of attendances were on a Sunday.
Percentage attendance by day for each age group
In the 5–14 age group attendances were lower at the weekend than during the week, but this trend was reversed in the 15–24s with the exception of Mondays. In the 25–44 age group no clear pattern was shown. Attendances were relatively constant, with Mondays having slightly more and Saturdays slightly less than the rest of the week.
The 45–64, 65–74, and over 75 age groups all followed the same pattern, with most attendances on Mondays and Fridays and least at the weekend.
“Out of hours” attendances were classified as being between 19:00 and 07:59 Monday to Friday, and at anytime on a Saturday or Sunday. The percentage of “out of hours” attendances in this dataset was 52.3%. This was highest in the under 1 age group (58.5%), the 15–24 age group (57.1%), and the 25–44 age group (54.6%). “Out of hours” attendances were lowest in the 65–74 and over 75 age groups (48.1% and 47.7% respectively).
Month of attendance
Table 4 shows the attendances by month. In those less than 1 year old there was a marked increase in attendances in November and December. The percentage attendance reached 11.6% in December, which was the highest attendance in a single month of all age groups.
Percentage attendance by month for each age group
In children aged 1–4 years attendances were spread quite evenly throughout the months, with slightly more in summer than winter. In those aged 5–14 this trend was much more pronounced with 31.2% of patients attending between May and July.
In the 15–24 and 25–44 age groups attendances were relatively constant throughout the months, with the winter months being slightly lower. Attendances in the summer months were higher than those in winter in the 45–64 age group, with the exception of an increase in December. In the 65–74s and the over 75s this winter peak was much greater with December having the most attendances (10.1% and 10.5%).
DISCUSSION
No sex differences were found in the hour, day or month of attendance at A&E. However, many differences were found in the attendance patterns of different age groups.
Attendance patterns vary according to the type of incident, injury, or condition. For example, attendances after assault occur more frequently late at night and early in the morning, where as attendances after a fall tend to be during the day. This is attributable to the age groups associated with the types of incident. Assault is common among those aged 18–30 years,8 who tend to stay out later at night, and is related to alcohol consumption. Falls are common among all ages, but especially in the very young and very old.
A high proportion of people attending A&E are self referred, and this increases “out of hours” as general practitioner (GP) surgeries close.9 This can be seen especially in the younger age groups, where attendance peaks between 18:00 and 07:59. An increasing number of departments have senior cover until midnight.10 This seems to be appropriate, as the proportion of attenders arriving after midnight is low and decreases through the early hours of the morning. However, as stated earlier, workload during this time may include a relatively high proportion of major trauma.
Over 55% of those under 1 year old and over 50% of those aged 1–4 attended “out of hours”. Parents of young children may tend to take them straight to the A&E department instead of calling out a GP, or be directly referred to A&E by a GP. It is not known whether or not these children needed treatment in A&E, or could have successfully treated by their GP. Analysis of the associated triage categories may be one way of investigating this, however triage information is not routinely collected as part of the minimum dataset. These results may have implications for separately staffed paediatric A&E facilities, which will need different shift patterns to adult facilities as the pattern of attendance varies considerably.
Over 50% of the 15–24 age group attended “out of hours”. This age group accounts for a large percentage of violence related attendances, 43.3% of male and 34.6% of female assault attendances in this dataset. This is one of the reasons for the high level of “out of hours” attendances.
Most A&E attendances were made on a Monday. This phenomenon was found in all age groups except the very young. Many of these may be because people who injure themselves at the weekend do not visit A&E immediately, as they do not the consider themselves to need immediate treatment. They then seek attention later.11
Attendance throughout the week varied in several ways, the main one being that the proportion of weekend attendances decreased with age. In those over 65 years, this may be because they have less contact with people and have no means of transport to the hospital. Weekend attendance is also lower in the 45–64 age group. This may be attributable to the attendance patterns of the upper end of the age group, distorting that for the lower end. Younger people tend to participate in more sports events, and are more likely to be involved in an assault or a road traffic accident at the weekend.
Attendances were higher during the summer months for most ages except the very young and very old. This was quite marked in the 15–24 age group where attendances were highest between May and July. The Violence Research Group analysed assault attendances for seasonality and found that attendances after assault peaked during the summer months between July and September and were at their lowest between February and April.8 The 15–24 age group accounts for a large proportion of assault attendances, hence similar seasonal patterns are observed.
After the age of 65 there was a marked increase in the number of attendances in December, and a smaller increase in January. Older people are more susceptible to respiratory illness such as influenza and bronchitis, which are more prevalent during the winter months. These can be complicated by other medical conditions, leading to more severe illness.12 Falls also account for a lot of A&E attendances in older people, when they tend to injure themselves in late autumn and early winter.
Information collected by the Department of Health shows that in winter 1999/2000 A&E attendances were high from week 48 to week 1.6 Research has shown that there is a strong link between a recent decrease in temperature and an increase in the incidence of bronchitis, and is an important factor in influenza epidemics.7 This is particularly significant in December and may explain some of the increases in A&E attendance during the winter months.
Monthly attendances at A&E will vary year to year, partly because of the incidence of influenza and other respiratory infections that commonly occur in winter. This study is based on one year of data, therefore may not be generalisable to other years.
Among child injuries boys are more often victims than girls, with most injuries occurring during the summer months.13 During this time children are on school holidays and have more free time to take part in activities or are enticed out by the lighter nights and come into contact with busy roads. However, road traffic accidents represent only a small proportion of child accidents, most are “leisure” accidents, which increase as free time increases. This is reflected in the fact that the peak incidence of child pedestrian and bicyclist injuries occur during the summer months and afternoon hours.14 Nearly 90% of paediatric bicycle accidents occur during daylight hours, with 65% occurring between 15:00 and 18:00 hours.15
It is important to consider the whole A&E population and their attendance patterns, as the numbers attending determines the staffing and support services levels required.16 It is important in determining whether there is a need for 24 hour a day consultant cover, or 16–18 hours a day and when those hours should be.10 It also has importance outside A&E in the planning of social, preventive, and intermediate care services, especially in regard to vulnerable groups such as the young and the elderly.
This study was based on one year of attendance data, therefore some of the age groups contain small numbers. It would be useful to expand the number of years included in the analyses to see whether the same patterns are observed, especially for the month of attendance. It should be noted that the analyses were based on a sample of Trusts that submitted data, so may not be generalisable to the region as a whole or to other parts of the country. However, some clear differences in attendance patterns between different age groups have been observed and it would be interesting to see if these were repeated in other areas of the country.
There will be further investigation by cause of injury or nature of the illness to understand the underlying variations in the temporal attendance patterns by age. The study does not look at the pattern of contacts with other services, such as the number of people contacting their GP and then attending A&E, or calls to NHS Direct. This would be important for looking at whether A&E remains for many the first port of call.
Acknowledgments
This project is funded by the Department of Health Public Health Development Fund. The authors would like to thank the Trusts and Health Authorities involved for making the data available, and Dr Matthew Cooke for his comments on the paper.
Contributors
Richard Wilson was responsible for initiating and coordinating the project. Amy Downing collected, analysed and interpreted the data, and is the guarantor of the study. Both authors designed the study and jointly wrote the paper.
REFERENCES
Footnotes
-
Competing interests: none declared.