Article Text

Abstract
Objectives: This study was designed to investigate the effect on skin temperature of different methods of use of a hydrogel dressing.
Methods: Twelve volunteers had temperature measured under a hydrogel dressing with different combinations of air movement and bandaging.
Results: A large drop in skin temperature was only achieved when the dressing was left exposed with air movement over the surface of the dressing.
Conclusions: A temperature that gives effective analgesia is not reached if the dressing is used in accordance with the manufacturer's instructions (covered with an insulating layer). This explains the authors' observation that paramedics and patients often leave these dressings uncovered.
- burns
- hydrogel dressing
Statistics from Altmetric.com
Burns are common injuries, but their management can be complex 1 and there are scarce data to define optimal initial treatment. A hydrogel dressing (Waterjel) is commonly used by ambulance service personnel in the prehospital treatment of a burn.2 These dressings are non-adherent and are available in sizes ranging up to a “whole body” sheet. Analgesia is provided by cooling 3 from evaporation of water and volatile substances. The manufacturer recommends that the dressing is covered, however we have observed that patients often arrive in the accident and emergency (A&E) department with these dressings uncovered. We therefore investigated the effect of different methods of use of a hydrogel dressing on skin temperature.
METHODS
The sample size was calculated assuming a clinically significant difference of 4° degrees (the difference between normal skin temperature and the analgesic threshold of 28°) using a β value of 0.9 and an α value of 0.05. Ethics committee approval was obtained. Twelve normal volunteers were studied in a temperature controlled laboratory. Skin temperatures were measured on the dorsal surface of both forearms, with one arm being tested and the other being used as a control.
The skin temperature was recorded for 15 minutes before the application of the dressing, for 20 minutes with the dressing in place, and then for five minutes after removal of the dressing (20 minutes approximates to the transport time to hospital). The combinations of dressings studied were:
-
Hydrogel dressing alone
-
Hydrogel dressing wrapped in a thick bandage
-
Hydrogel dressing with air movement
-
Hydrogel dressing wrapped in thick bandage with air movement
Air movement was created by a desktop fan at a standard distance and setting. These combinations were used to re-create conditions commonly found in the prehospital care of patients with burns.
RESULTS
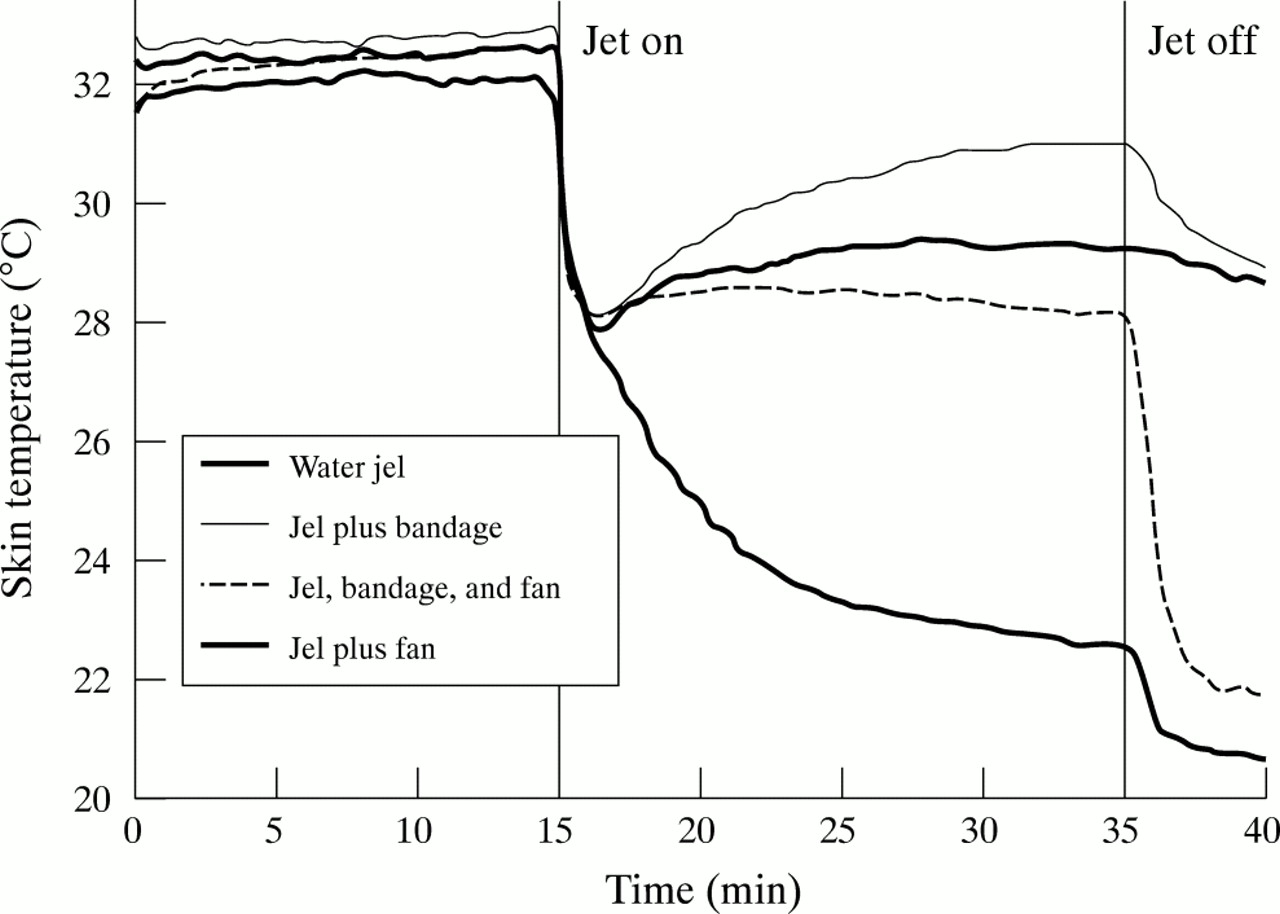
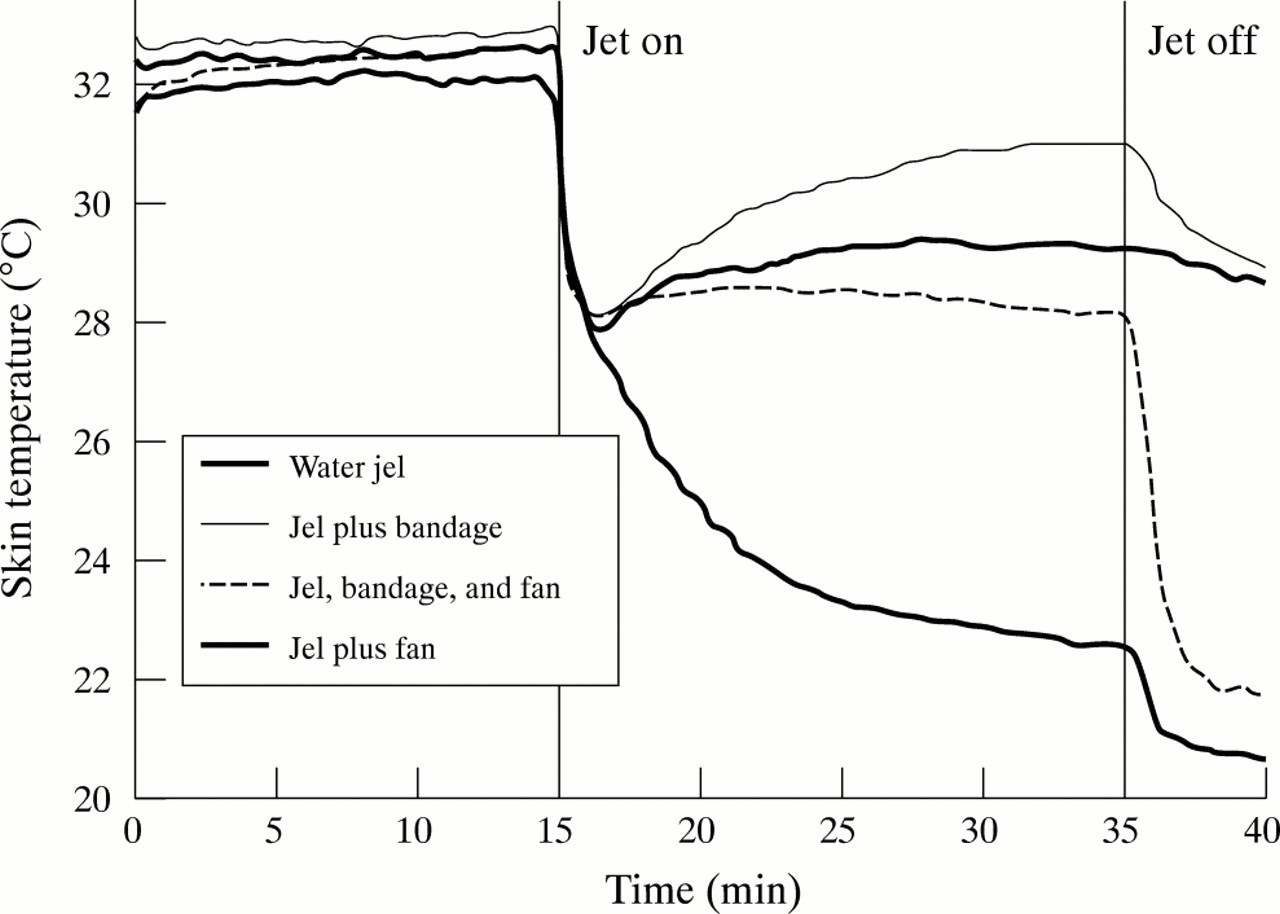
The pattern of change of skin temperature with time under each of the dressings is shown in figure 1. On initial application all dressing combinations cooled the skin to give some analgesia, however only one of the conditions (airflow over the dressing with no bandage) resulted in a skin temperature low enough to give analgesia throughout. With air movement over the area, there was a large additional drop in skin temperature after removal of the dressing.
{kind=link}
Change in median skin temperature with time.
DISCUSSION
It is probable that, through experience, prehospital personnel have realised that for the dressing to remain an effective analgesic there must be air movement over the surface (patients also learn this and are sometimes seen blowing on their own dressing). This explains our observation that Hydrogel dressings are often left uncovered. This will optimise analgesia, but if the dressing covers a large area the patient will be exposed to the risk of excess heat loss and hypothermia. This effect is probably most marked in children, because of the larger surface area/mass ratio.
The finding of a large additional drop in temperature after the dressing was removed was unexpected. This effect may be attributable to exposure and subsequent evaporation of volatile substances and water in the residual layer of gel that is left on the burn after removal of the dressing. A&E staff should be aware of this potential problem and ensure that evaporation is immediately prevented, perhaps by covering the burn with clingwrap.
The cooling curves on burnt skin may be different from those in this volunteer study. However, from these results we would suggest that a hydrogel dressing without a cover is an appropriate prehospital dressing for small burns, giving analgesia without risk of hypothermia. For larger burns, especially in children, an alternative dressing that does not lead to heat loss should be used.
Contributors
Tim Coats initiated the project, coordinated the developement of the protocol, supervised the study, and led the writing of the paper. Caroline Edwards, Richard Newton, and Elisha Staum participated in the design of the study, carried out the data collection, discussed the data interpretation, and reviewed the paper.
Funding: Anthony Hopkins Memorial Fund.
Conflicts of interest: none.