Article Text

Abstract
Needle aspiration is a recognised emergency treatment of spontaneous pneumothorax and in the case of suspected tension is usually performed before chest radiography. Three cases are described of apparent life threatening haemorrhage after anterior aspiration in the second intercostal space, mid-clavicular line (2ICS MCL) requiring resuscitation, and transfer to a cardiothoracic unit. In these patients there was no evidence of haemothorax on initial presentation. Lateral needle aspiration, in the site recommended for chest drain insertion, the 5th intercostal space, anterior axillary line (5ICS ALL) is technically easy and may be a potentially safer option for decompressing pneumothoraces.
- tension pneumothorax
- decompression aspiration
Statistics from Altmetric.com
Anterior needle aspiration in the 2ICS MCL is the recognised treatment for pneumothoraces using standard ATLS1 and British Thoracic Society Guidelines (BTS).2 The BTS guidelines state that an axillary approach is an alternative to the 2ICS MCL but no precise point is identified. For suspected tension pneumothorax aspiration is usually done before chest radiography as delay could lead to a cardiorespiratory arrest. Anterior decompression is theoretically safe and can be performed rapidly as all necessary equipment is at hand. However, we report three cases of life threatening haemorrhage, which appeared to follow anterior needle aspiration. Initial examination/chest radiography, had shown no evidence of haemothorax. After aspiration chest radiographs showed haemopneumothoraces requiring drain insertion and transfer to our cardiothoracic unit.
CASE 1
A 27 year old man presented with sudden right chest pain and shortness of breath. Chest radiography showed a right tension pneumothorax with no evidence of fluid level. Needle aspiration in the right 2ICS MCL was performed (dressing and puncture wound confirmed site), after this chest radiography showed haemopneumothorax. On formal drain insertion in the 5 ICS ALL a total of two litres of blood was drained. The patient was resuscitated, transfused, and transferred to a cardiothoracic unit for further treatment. He required video assisted thoracoscopy for on going bleeding, and a persistent air leak. At video assisted thoracoscopy blood clot was adherent to the anterior lung surface with a contused area of presumed iatrogenic injury. He made an uneventful recovery.
CASE 2
A 24 year old man presented with right sided chest pain and shortness of breath. Chest radiography confirmed a pneumothorax with no fluid level. Needle aspiration in the 2ICS MCL (puncture wound confirmed site) was performed. Post-aspiration chest radiography showed an improvement of the pneumothorax and no fluid level. He was discharged after observation, but returned the next day with increasing pain and shortness of breath. Chest radiography showed a haemopneumothorax with evidence of an apical collection. The patient had 1.2 litres blood loss after insertion of a chest drain requiring resuscitation, transfusion, and transfer to a cardiothoracic unit. The bleeding resolved and he was managed conservatively with good outcome.
CASE 3
A 27 year old man presented with left sided chest pain and shortness of breath. Chest radiography confirmed a tension pneumothorax with no fluid collection. Aspiration in 2ICS MCL followed by chest radiography, suggested a fluid collection. Chest drain insertion was followed by 1.5 litres bleeding and he was resuscitated, transfused, and transferred to our cardiothoracic unit. Emergency thoracotomy was performed for ongoing bleeding and haemodynamic instability (consultant preference). A large quantity of clot was evacuated and apical pleurectomy performed. The patient made an uneventful recovery.
DISCUSSION
Most pneumothoraces are uncomplicated by cardiorespiratory compromise and symptomatic patients can be managed by aspiration or intercostal drains depending on the size of the pneumothorax. Success rates for aspiration vary from 68% 3 to 75%.4 Emergency decompression in the 2ICS MCL can be life saving in tension pneumothorax and although quick and reputedly safe most are performed in the accident and emergency department by comparatively junior doctors who may have limited experience. This may be exacerbated by the urgency of the clinical picture. Data on the incidence of needle aspiration in spontaneous pneumothorax and its complications are limited. In a study of 6241 major trauma patients with suspected pneumothoraces 108 (1.7%) underwent needle thoracostomy with two iatrogenic pneumothoraces reported and no other complications. 5 Variation in chest wall thickness, insufficient cannula length, and inexperience in performing aspirations contribute to inadequate needle aspirations, and may increase the risk of complications.6,7 The internal mammary artery and branches medially and the subclavian vessels superiorly are closest to the 2ICS MCL. Intercostal vessels may also be damaged.
The cases presented occurred over a six month period and drew our attention to the possibility that the proximity of the 2ICS MCL approach to the above vascular structures could result in injury. The aspiration sites were all identifiable by the puncture wounds and all corresponded to the 2ICS MCL. These patients all required resuscitation and two required surgery. Although it is impossible to conclude that the haemorrhage was caused by the anterior aspiration it is a clear possibility because of the lack of evidence for haemothorax as part of the initial presentation. Other considerations developed the theory of potential danger with the anterior approach. After lung collapse vascular adhesions may bleed freely into the pleural space,8 which in the volumes involved in our three patients would be evident on percussion or on chest radiography. Initial chest radiographs all showed pneumothoraces with no fluid levels, which suggest that bleeding occurred at a time, separate from the pneumothorax. In the two cases that proceeded to surgery no bleeding vascular adhesions were seen. Unfortunately surgery could not confirm which vascular structure had been damaged; however, this is often notoriously difficult unless there is active bleeding. In all three cases the blood loss was substantial requiring active resuscitation. In the second patient whose haemothorax was confirmed the following day, we were concerned that the apical cap on the chest radiograph represented a haematoma from iatrogenic injury to the subclavian vessels.
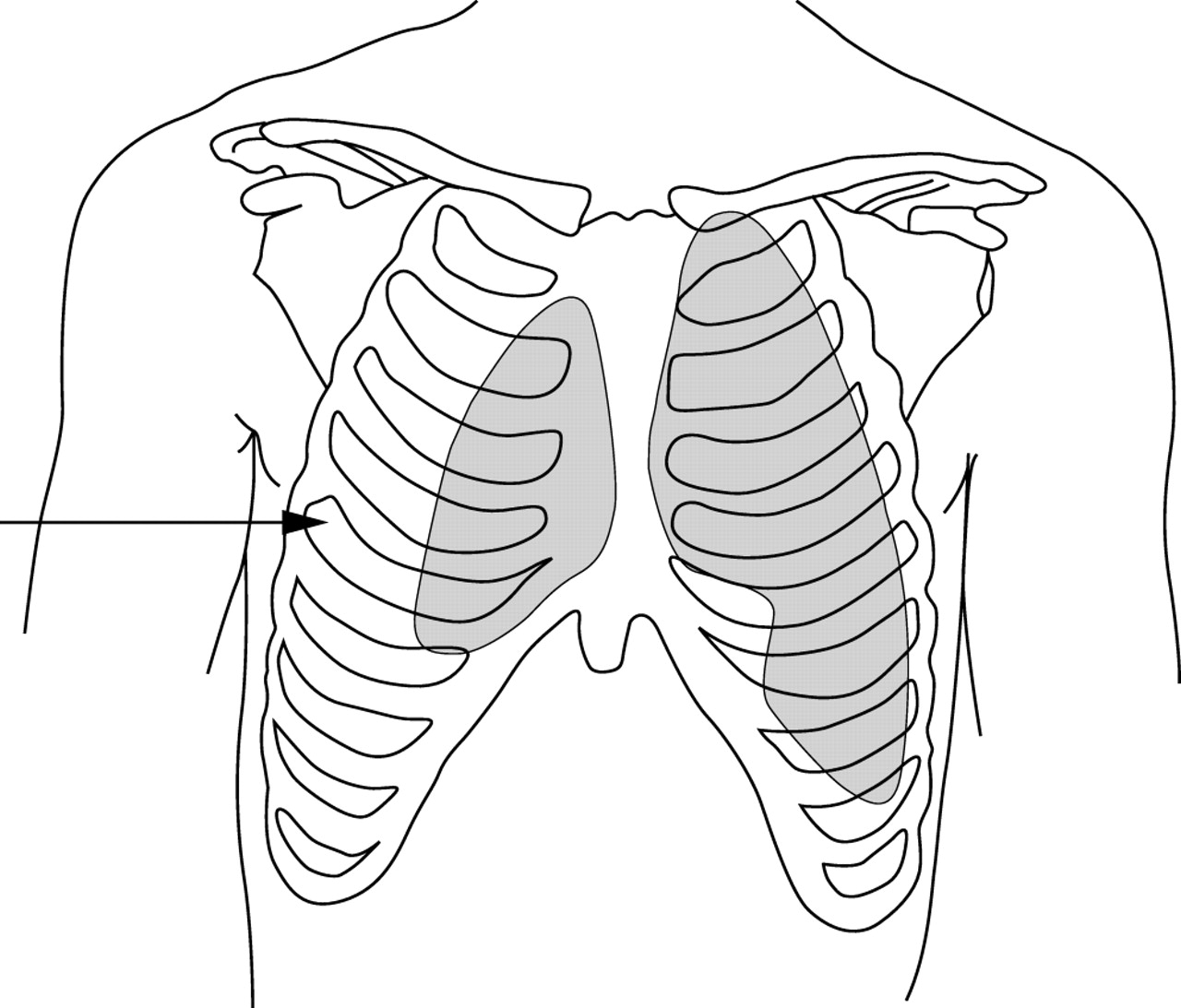
For chest drain insertion ATLS guidelines clearly recommend an approach from the 5th intercostal space, anterior axillary line (5ICS ALL) as drainage of both air and fluid is possible, and the entry point is high enough to minimise the chance of abdominal injury. In the BTS guidelines an axillary approach is also suggested although no precise point is identified. With most significant and especially with tension pneumothoraces, radiography shows a moderate or large lateral air space with the lung collapsed down towards the hilum (fig 1). The fact that these patients are often lying supine may suggest this procedure may be more suitable for patients with large pneumothoraces. Lateral aspiration in 5ICS ALL, is technically easy and may provide a safer option for decompressing spontaneous pneumothoraces, as it avoids major vessels and the lung that lie closer to the anterior chest wall.

{kind=link}
Arrow showing location for needle thoracocentesis in the 5th intercostal space, anterior axillary line.
Contributors
Randolph Rawlins initiated the reporting of this finding and was responsible for intellectual input. He is the corresponding author and is guarantor for the information in this paper. Cornelia S Carr was responsible for intellectual input, editing, and writing the final draft. She reviewed the literature and references. Karen M Brown was responsible for producing the line diagram showing the site for aspiration as well as reformatting, referencing, and resubmitting the article after the firsts reviewers comments. C R Cameron Is the senior author and consultant thoracic surgeon. He was responsible for overseeing this paper, advising and making recommendations for the final paper.