Article Text

Statistics from Altmetric.com
A 14 year old boy presented to the accident and emergency department of a district general hospital with a 24 hour history of a painful swollen left eye, exacerbated by movement. A history of allergy to dog hair was noted. On examination there was unilateral periorbital swelling of the left eye with a normal conjunctiva (fig 1). An allergic reaction was diagnosed and treated with piriton and sodium chromoglycate eye drops.

Left sided periorbital swelling and proptosis.
Two days later at review he was systemically unwell and had a temperature of 39.3°C. The left sided periorbital swelling had worsened. Visual acuity and fluorescein staining were unremarkable. He was noted to have bilateral large erythematous tonsils. It was felt at that time to be a worsening allergic reaction. However, oral flucloxacillin was added, and ophthalmology review was arranged for the following day.
Ophthalmology assessment four days after the onset of symptoms revealed the salient features of a recent upper respiratory tract infection and a long history of a blocked left nostril and snoring.
On examination there was proptosis, swollen and erythematous eyelids, chemosis of the sclera, and restricted eye movements. There was pronounced left maxillary tenderness.
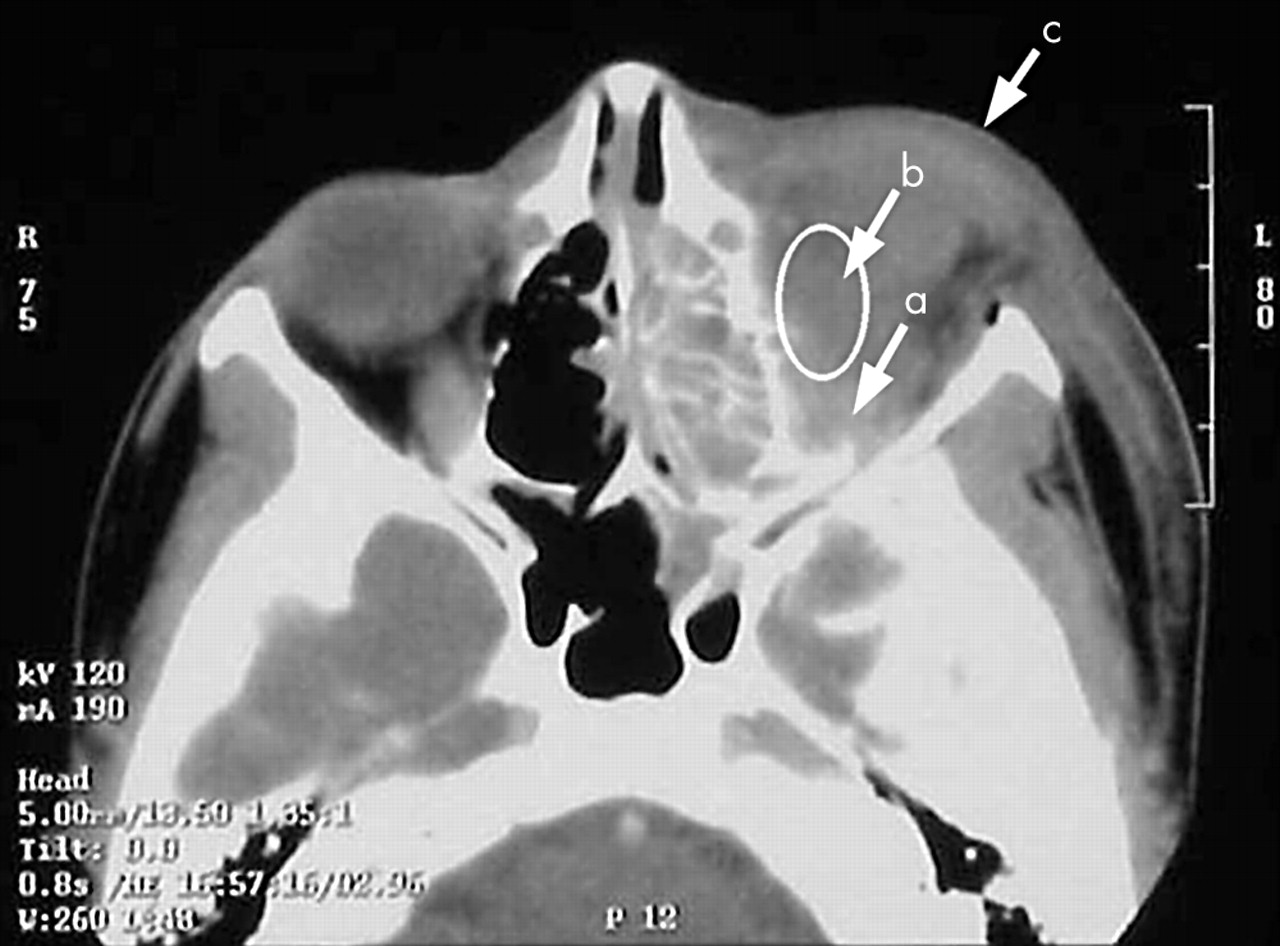
Blood tests revealed white cells of 18×109/l with a neutrophilia and C reactive protein of 128. Urgent computed tomography demonstrated left proptosis with considerable soft tissue swelling (fig 2). All sinuses on the left were filled with fluid. There was enhancing inflammatory tissue in the inferior aspect of the orbital floor, with associated gas. The optic nerve and orbital soft tissue were enlarged. The diagnosis of left orbital cellulitis secondary to maxillary sinusitis was made and the patient was admitted under the care of ENT and ophthalmologists.
{kind=link}
{kind=link}
CT scan showing the orbit with the optic nerve (a), compressed by the orbital abscess (b). Proptosis and soft tissue swelling (c) is also shown.
The patient underwent emergency endoscopic drainage of left orbital abscess, endoscopic sinus surgery, and subcutaneous abscess aspiration resulting in a noticeable reduction in proptosis. Maximum dose intravenous cefuroxime and metronidazole were started. Microscopy and culture revealed Streptococcus millieri. Though showing steady improvement after surgery, the patient returned to theatre two days later for aspiration of the subcutaneous cheek abscess and repeat antral wash out. He was discharged home three days later and was well at his six week outpatient follow up appointment.
DISCUSSION
Orbital cellulitis is an emergency. It is important that it is recognised early and managed aggressively. Although the incidence of orbital cellulitis has remained low with better primary health care and availability of a broad range of antibiotics, it is often a difficult problem to manage and may cause blindness if left untreated because of optic nerve compression. Both orbital abscess and cavernous venous thrombosis may lead to intracranial spread of infection, such as meningitis or cerebral abscess with high morbidity and possible mortality.
The serious risk of complications in such cases was made clear by Hodges et al1 who studied the outcome in orbital cellulitis in a developing country. They found a high rate of complications, 52% blind on admission, with no improvement after treatment and a mortality of 4% because of cavernous venous thrombosis. These results reflected the delay in presentation in this population.
Box 1 illustrates the differential diagnosis of periorbital swelling.
Box 1 Differential diagnosis
-
Preseptal cellulitis
-
Orbital cellulitis/abscess
-
Dacryocystitis
-
Trauma
-
Allergic eye
-
Uveitis
-
Neoplasm
-
Eyelid insect bite
The orbital septum is a thin membrane that originates from the orbital periosteum and inserts into the anterior surfaces of the tarsal plates of the eyelids. The septum separates the superficial eyelid from the deeper orbital structures, and it forms a barrier that prevents infection in the eyelid from extending into the orbit. Preseptal cellulitis differs from orbital cellulitis in that it is confined to the soft tissues that are anterior to the orbital septum.
Orbital allergic reaction includes, conjunctival injection, blepharitis, periorbital dermatitis, and oedema of the eyelid.2 Pruritis and oedema are the most common clinical findings, although this is usually bilateral.
Table 1 shows the main differences in presentation between cellulitis and eye allergy.
Difference in presentation
Within the accident and emergency or general practice setting it is important to recognise an infected eye that requires urgent specialist referral.
The distinction between preseptal cellulitis and orbital cellulitis is important, but this is often difficult clinically and can be made by the appropriate specialist who has access to investigations such as CT scans.
Sinusitis is the most common predisposing factor to orbital cellulitis and abscess formation. Figures of 60%–91% of orbital cellulitis secondary to sinusitis have been reported.1,3–6 Ethmoidal and maxillary sinuses are most commonly affected.3,4,7,8 Bacterial orbital cellulitis attributable to sinusitis is primarily a disease of the paediatric population,3,4 although it can affect any age group. Ferguson et al4 found that 91% of the paediatric population with orbital cellulitis had sinusitis, with 38% having multiple sinus involvement. Some studies report a peak incidence between 6–15 year olds,4 while others report a bimodal distribution, with another peak in incidence at 60–70 years. There is also a male preponderance to the condition,1,4,5,8,9 although no satisfactory explanation can be offered for this observation. A seasonal variation4 is attributable to the increased incidence of upper respiratory tract infection at these times of the year.
Box 2 Important lessons
-
Unilateral swelling of the orbit is more likely to be infection than allergy
-
Early referral from primary care or A&E is essential to avoid serious complications
-
Close cooperation between paediatrics, ophthalmology, and ENT is vital to ensure optimum patient management
Administration of oral antibiotics may change the presentation, which may be relevant if the patient has already seen their general practitioner or been admitted to a paediatric/other ward. It is not uncommon for children to be admitted to a paediatric ward with an orbital infection. Hereafter there may be a delay in further investigations and specialist referral, as the urgency of the condition may not be fully appreciated.
It is well reported that CT is the investigation of choice3–10 for orbital cellulitis, permitting accurate localisation of the sinus infection and grading of the orbital inflammation. Studies have shown that 30% of patients with suspected preseptal cellulitis have evidence of orbital involvement on CT scan.6
General management principles should include (1) obtaining adequate specimens for microbiological studies; (2) high dose broad range of intravenous antibiotics; (3) changing antibiotics according to sensitivities; and (4) intervening surgically at the appropriate time. This is usually after 24 hours, if there is no response to medical management. The authors could find no agreed antibiotic regimen in the literature. Principles of surgical management include (1) temporary orbital decompression; (2) drainage of orbital or subperiosteal abscess, via external or endoscopic routes; and (3) drainage of effected sinuses.
There were no long term complications in this particular case, but it does highlight that orbital inflammation should not be immediately blamed on allergy. It needs sufficient evaluation to exclude cellulitis or abscess formation, even without clinically obvious sinusitis.
Orbital cellulitis usually presents to the general practitioner, paediatrician, or accident and emergency department. Rarely do the ENT surgeons or ophthalmologists see it initially. Multiple abnormalities may be present, so close cooperation between all these specialties is vital for the successful management of this condition.
The authors believe that all patients with orbital inflammation require hospitalisation and CT scan without delay. We agree with Tole et al6 who concluded that “A high index of suspicion and a low threshold for early specialist referral is required for optimal management of orbital cellulits”.
Linked Articles
- Primary Survey