Article Text

Abstract
Objectives: To identify the causes of acute headache presenting to the emergency department (ED), assess the adequacy of history, examination, and investigation, and determine which clinical features are predictive of secondary headache.
Method: A retrospective study of alert (GCS⩾14) patients presenting with headache, to an ED over a one year period. Patients were followed up for three months. The adequacy of history, examination, and investigation were compared with published standards. Analysis using Bayes’s theorem determined which clinical features were predictive of secondary headache.
Results: Headache in alert patients accounted for 0.5% (n = 353) of new patient episodes, 81.2% (n = 280) of patients had a primary headache disorder. One patient (0.3%) had an adequate history recorded. No patient had a complete examination recorded. Seventy seven (21.8%) patients underwent computed tomography of the head; 80.5% (n = 62) were normal. Lumbar puncture was performed in 23 (6.5%) cases; 18 (78.3%) were normal. A number of clinical features were found to be predictive of secondary headache.
Conclusion: Headache is an uncommon symptom in alert patients presenting to the ED. The recorded history, examination, and subsequent investigation do not comply with published standards. A number of predictive features have been identified that may permit the development of a clinical prediction rule to improve the management of this patient group.
- headache
- SAH, subarachnoid haemorrhage
- ED, emergency department
Statistics from Altmetric.com
Headache is one of the commonest neurological symptoms and is an almost universal experience for adults. Headaches fall into two categories of primary, non-organic headache, and secondary, organic headache. It is the second that usually requires investigation in the emergency department (ED). However, all patients complaining of headache should be approached in the same way, with meticulous attention to the history and examination. If in doubt, patients should be investigated and observed, with expert opinions being sought when appropriate.
Studies have shown that among those secondary headaches presenting to the ED, 63% represent systemic infection, 4% are post-traumatic headaches, 0.1% are attributable to space occupying lesions, and <1% are attributable to subarachnoid haemorrhage (SAH).1 In 1989 Fodden and colleagues reviewed 130 patients presenting to an ED with headache, and followed them up for two years. They found that this presentation represented only 0.36% of new patient attendances but 16% of these patients had serious neurological pathology. The authors comment on the low attendance rate of patients with this problem, but the high incidence of serious pathology detected.2
If serious pathology is suspected or the diagnosis remains unclear, investigation may be indicated. Edmeads points out that investigation is necessary when the patient complains of the worst headache ever, onset of headache with exertion (more suggestive of SAH or raised intracranial pressure), reduced alertness or cognition, neck not perfectly supple (implying blood or pus in the cerebrospinal fluid (CSF)), any abnormality on examination (including fever), or worsening under observation.3 The accurate diagnosis of SAH is a cause of ongoing concern for emergency medicine doctors. It is vital to obtain a careful history and thorough examination that will provide clues to the final diagnosis, as it is known that early surgery improves outcomes.4 Computed tomography is useful in patients suspected of having a secondary headache.5 In suspected SAH it is the initial investigation of choice, and may show subarachnoid blood in 95% of cases on the day of the bleed, declining to 90% after one day.6 If computed tomography is normal all such patients should have a lumbar puncture performed and the CSF examined for blood, and centrifuged looking for xanthochromia in the supernatant. It is recommended that the lumbar puncture is not performed until at least 12 hours after the onset of symptoms, which will detect xanthochromia (by spectrophotometry) in 100% of cases.6,7
This study aims to identify the causes of acute headache, in alert patients presenting to the ED, assess the adequacy of history, examination, and investigation, and determine which clinical features predict the presence of a secondary headache.
METHOD
A retrospective study was performed in the ED of the Northern General Hospital, Sheffield, a large urban teaching hospital. All patients with a primary presenting complaint of headache attending the ED between 1 January and 31 December 2000 were eligible for inclusion. Patients were excluded from the study if any of the following were present: age <16 years; post-traumatic headache; headache not the primary presenting symptom; notes not available for review; Glasgow coma score (GCS) <14 (eye opening = 3, motor function = 6, verbal response = 5).
A search of the ED database was carried out to identify all patients eligible for inclusion. For each patient the ED notes and, where relevant, inpatient notes were reviewed. For each included patient a standardised data collection form was completed, recording demographic and clinical information, as well as final diagnosis. Final diagnosis was taken to be that recorded by the ED doctor for patients discharged and the diagnosis recorded on the discharge summary for those admitted.
Three months after the patient’s initial attendance the hospital database was searched for any subsequent ED or hospital episodes. Where there were further ED or hospital episodes, or the patient had died the relevant notes were reviewed. For the purpose of analysis patients were assigned to one of the following groups:
-
Abnormal examination—patients found to have an abnormality on neurological examination
-
“First or worst” headache—patients with a normal neurological examination presenting with their first or most severe episode of headache.
-
Usual headache pattern—patients with a normal neurological examination who had previously suffered headaches of the same character and severity.
-
Indeterminate—all patients who did not fit the criteria of any of the preceding three groups.
The data were analysed to examine how each group compared with the published recommendations outlined below. Analysis using Bayes’s theorem determined which demographic or clinical features were predictive of secondary headache. Using Bayes’s theorem is equivalent to multiplying the likelihood ratio (that is, the ratio of the proportion of those with the disease that have the symptom, to the proportion of those without the disease but who also have the symptom). In this case the “disease” is secondary headache. The likelihood ratio was then converted to a “weight of evidence” using Good’s method.8 Deriving weights of evidence has been applied in the fields of gastroenterology and rheumatology.9,10
History
A number of key points referred to as the “headache history” have been outlined by Freitag and Newman (table 1).5,11 These were taken to be the standard used for comparison in this study.
Examination
Marks has stated that all patients presenting with headache should have a physical examination including assessment for neck stiffness, rash, a full neurological and ENT examination, and blood pressure measurement.12 This was taken to be the examination standard used for comparison.
RESULTS
During the period studied there were 77 421 new patient episodes. Four hundred and thirty six (0.6%) eligible patients were identified from the ED database. Of these patients, 83 were excluded: 44 had a post-traumatic headache; three were under 16 years; four did not present with headache; 16 had a GCS of less than 14 (13 had SAH, two had migraine, and one patient was post-ictal); notes were unavailable in 16 cases. Alert patients presenting with headache represented 0.5% of new patient episodes (n = 353).
Figure 1 shows the age/sex distribution of the study group. The median age range was 26–35 years old.

Age/sex distribution (n = 353).
Data regarding final diagnosis were available for 345 patients (97.7%) (table 2). Two hundred and eighty (81.2%) patients were diagnosed as having a primary headache disorder, 65 (18.8%) patients had a secondary headache.
Discharge diagnosis by category
History and examination
Only 1 of 353 (0.3%) sets of case notes met the standard for history taking outlined in table 1. No patient had a complete assessment recorded, as suggested by Marks.12
Computed tomography
Seventy seven (21.8%) patients underwent head CT during their hospital attendance, 44 (57.1%) of these were performed while the patient was under the care of the ED. Sixty two scans (80.5%) were normal. Seven scans (9.1%) demonstrated SAH and one (1.3%) demonstrated an intraparanchymal haemorrhage. The remaining seven scans (9.1%) showed cerebral or cerebellar infarcts.
Lumbar puncture
Lumbar puncture was performed in 23 (6.5%) patients. One patient refused the procedure. In four cases the procedure was unsuccessful. The CSF was normal in 18 patients and in one patient showed features consistent with viral meningitis.
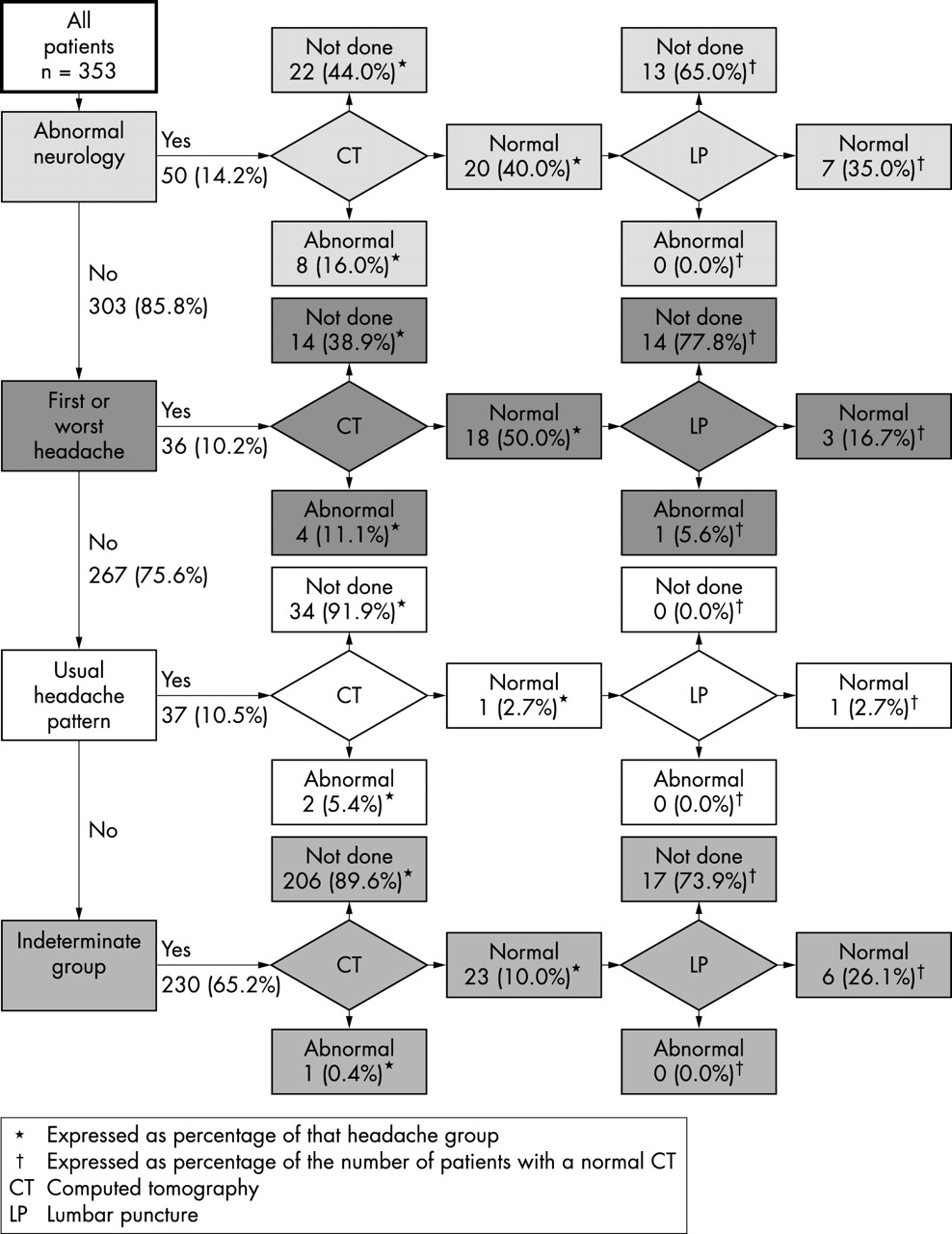
With regard to investigation the study group can be considered in the four groups outlined above. Figure 2 summarises the investigation of these groups.
{kind=link}
{kind=link}
Investigation of patients presenting with headache.
Abnormal neurology
Of the 50 patients found to have an abnormality on neurological examination, 13 (26.0%) were discharged from the ED without investigation, three (6.0%) patients were discharged from the ED after a normal head CT. One (2.0%) patient self discharged from the ED after a head CT revealed a cerebral infarct. Thirty one (62.0%) patients were admitted to hospital.
First or worst headache
Of the 36 patients who presented with their “first or worst” headache, 10 (27.8%) were discharged from the ED without investigation. Sixteen (44.4%) patients underwent CT in the ED. A further 10 (27.8%) patients were admitted before any investigations had been completed and six (16.7%) subsequently underwent CT. Of 18 patients who had a normal head CT scan, only four (11.1%) underwent lumbar puncture. It was not clear from the subjects’ case notes why lumbar puncture had been omitted.
Usual headache pattern
Thirty seven (10.5%) patients presented with their usual pattern of headache and no recorded abnormality on neurological examination. Thirty (81.1%) patients were discharged from the ED without investigation. Of the seven (18.9%) patients admitted to hospital, one underwent CT in the ED and a further two during their inpatient stay. One scan was normal, the remainder showed cerebral infarcts.
Indeterminate group
Two hundred and thirty patients (65.2%) did not meet the criteria to be included in any of the preceding groups. One hundred and eighty six (80.9%) were discharged from the ED without investigation. Two patients were discharged from the ED after a normal CT scan. Of the 42 patients admitted to hospital, 22 (9.6%) underwent CT. One scan showed a cerebral infarct, the remainder were normal. Six patients underwent lumbar puncture, all were normal.
Follow up
At three month follow up two (0.6%) patients had died. In both cases this had occurred during their initial admission. One patient died as a result of the SAH with which they presented to hospital, the other death occurred in a patient who presented with headaches resulting from superior vena cava obstruction complicating a bronchial carcinoma. Fourteen (4.0%) patients had subsequently attended the ED or been admitted to hospital with headache. Eight (2.3%) patients were diagnosed as having a primary headache. Four (1.1%) patients had a secondary headache consisting of systemic infection (n = 2, 0.6%), viral meningitis (n = 1, 0.3%), and SAH (n = 1, 0.3%).
Clinical features predictive of secondary headache
All clinical and demographic features were assessed for their ability to predict secondary headache. The prior probability of a secondary headache in this sample was 18.8%. The posterior odds of the 15 most predictive features are outlined in table 3.
Clinical features predicting secondary headache (prior odds of secondary headache = 18.8%)
Four features were selected on the basis of their predictive ability, probable independence, and ease of measurement. These were age greater than 65 years, temperature greater than 38.0 °C, systolic blood pressure greater than 160 mm Hg, and the presence of neck stiffness. Applied to all patients in the study, the presence of at least one of these features predicted secondary headache with a specificity of 82.1% and a sensitivity of 37.8%. Applying this to the “indeterminate” group gives a specificity of 86.2% and a sensitivity of 21.2%. The diagnostic performance of multiple features in predicting secondary headache in both the total sample and in the indeterminate group is summarised in table 4.
Sensitivity and specificity of the selected four clinical features in combination
DISCUSSION
The small proportion of ED patients attending with acute headache reflects the fact that, although a common symptom, it rarely requires urgent attention. Something out of the ordinary must have happened for patients to present to hospital, and we must assume (until proved otherwise) this is a reflection of an underlying pathological process. We have shown that while patients presenting with headache and GCS of greater than 14 represent only 0.5% of all new patient episodes, over 18% of these have significant abnormality. This is in keeping with published data but is a probable underestimate of the true incidence, given the poor quality of history and examination and the lack of appropriate investigation that we have identified.2
History and examination
Both history and examination in the ED were found to be inadequate when compared with published standards.5,11,12 It is these areas where perhaps greatest improvement could be made for minimal cost. As stated elsewhere,13 improvement in training of ED doctors and an increased awareness of the variety of ways in which serious disease may manifest would lead to more detailed and accurate clinical assessment. The introduction of structured forms to record history and examination findings may enhance the quality of information recorded for each patient and facilitate improved diagnostic accuracy. In addition, it would simplify audit processes, permitting easier recognition of improvements in management. Guidelines on the recommended points of history and examination that should be recorded may assist inexperienced ED doctors when dealing with these patients. Furthermore, improvements in clinical assessment may reduce the number of patient assigned to the “indeterminate group”, facilitating clinical decision making processes particularly in relation to investigation or admission.
Investigation
It is clear from the data we have presented that CT is underused. All patients in the “abnormal neurology” or “first or worst headache” groups should have required CT according to published recommendations,3 producing a minimum of 86 (24.4%) head scans. If this is expanded to include the “indeterminate” group, then a maximum of 316 (89.5%) scans should have been performed. Neither of these targets was met, with only 77 (21.8%) scans performed. Lumbar puncture was also underused in this study. Again, the value of this investigation, particularly in suspected cases of meningitis or SAH, is widely accepted.5,14 Only 11.1% (4 of 36) of those patients presenting with a “first or worst” headache, and therefore, possible SAH, underwent lumbar puncture.
Why are these investigations not being used more frequently? It is possible that the frequent occurrence of headache in the general population, combined with a lack of knowledge of the potentially serious underlying causes and the ways in which they present, leads to the failure to thoroughly investigate these patients. The ongoing limited availability of CT to many EDs may play a part in this finding and it is vital that this issue is addressed.15
Predictors of secondary headache
A number of features have been identified that are predictive of the presence of secondary headache. Many of these findings would be expected, such as abnormal plantar reflexes or neck stiffness, which are recognised as signs of neurological abnormality. Most interesting, however, are other factors such as abnormal respiratory examination, pain that was stabbing in character, and pain situated in the orbit. These have been shown to considerably increase the probability of the presence of a secondary headache. Assessment of the predictive value of certain features has been hampered by the low frequency with which the presence or absence of that feature was recorded. The four features selected for use in combination (age >65, temperature >38°C, systolic blood pressure >160 mm Hg, and the presence of neck stiffness) while having inadequate sensitivity to rule out secondary headache, may prove useful in determining which patients may require investigation, particularly if more than one of the four features is present. Clinical predictors such as these will prove most useful in those patients in whom the correct management strategy is unclear, such as those assigned to the indeterminate group.
Improving management
A number of areas have been highlighted where there are inadequacies in patient management. Teaching programmes for ED doctors must include training on the issues we have raised. Improved training should be backed up by clinical guidelines regarding the assessment and management of these patients. This may be further improved by the use of standardised forms for recording history and examination findings, which have been shown to improve documentation in other areas of emergency medicine.16 Groups of patients who definitely require investigation can easily be identified in the ED, for example, “first or worst headache” or “abnormal neurology”. Protocols, agreed in conjunction with inpatient teams, should be in place so that these patients are investigated and managed appropriately and expeditiously. We have identified a large group of patients, the “indeterminate group”, in whom the correct management strategy is unclear. This group may be best served by development of a clinical prediction rule based upon specific points in the history and examination. This would aim to stratify patients into high and low risk groups, enabling focused investigation. The development of such a rule has to be methodologically sound for it to be safe and widely applicable. The standards to which such prediction rules should conform have been reported elsewhere.17,18 The main points include: determining the need for a clinical prediction rule, defining the predictive findings and outcome, and prospectively validating the clinical prediction rule. From the data presented here it is clear that there is a need for such a clinical prediction rule. A prospective study is needed to validate the predictive variables we have outlined and develop such a rule.
In a number of areas the ideal management of patients presenting with headache remains unclear. This has been highlighted in a recent literature review and policy statement by the American College of Emergency Physicians Clinical Policies Sub-committee on Acute Headache. The authors of this policy statement were unable to make any recommendations that consisted of “Generally accepted principles for patient management that reflect a high degree of certainty” based on currently available evidence.19 Further work is needed to provide high quality evidence to determine the optimum management of this important patient group.
Study limitations
This study has a number of important limitations. Being retrospective, we must assume that some patients eligible for inclusion have been missed, as identification was dependent upon data recorded in the ED database. We have demonstrated that the recorded history, examination, and investigation were inadequate in most of the patients. This may have significant impact upon not only upon the groups to which patients were assigned for data analysis, but also upon the accuracy of the final diagnosis recorded for most of the patients and therefore the validity of the predictive variables. It is clear that further prospective work is required to accurately delineate the performance of EDs in the assessment of patients presenting with headache and to investigate the issues we have raised. A prospective study examining the role of a clinical prediction rule and an ED rule out strategy is starting shortly in Sheffield.
Contributors
Thomas Locker participated in the design of the study, data collection, and analysis and in the writing of the paper. Suzanne Mason participated in the in the design of the study and writing the paper. Alan Rigby participated in the data analysis and in writing the paper. Thomas Locker acts as guarantor of the paper.
REFERENCES
Footnotes
-
Funding: none.
-
Conflicts of interest: none declared.