Article Text

Abstract
The objective of this study was to evaluate the effects of two different dosage protocols on the outcome of patients with severe neurotoxic snake envenoming, using a retrospective analysis of patients admitted with a diagnosis of severe neurotoxic snake bite over a 4 year period. In the study, 55 snake bite victims requiring ventilatory support for severe neurotoxic envenoming received either 150 ml of polyvalent snake antivenom (SAV) (low dose SAV group, n = 28) or 100 ml of SAV at presentation followed by 100 ml every 6 hours until recovery of neurological manifestations (high dose group, n = 27). The median dose of SAV in the high dose group was 600 ml (range 300 to 1600). The duration of mechanical ventilation in the low dose group (median 47.5 hours; range 14 to 248) was similar to that in the high dose group (median 44 hours; range 6 to 400). The mean (SD) duration of intensive care unit stay was similar in the two groups. There were three deaths in the high dose group; two patients in the low dose group had neurological sequelae. All other patients improved, had no residual neurological deficit, and were discharged. We conclude that there is no difference between a protocol using lower doses of SAV and one with higher doses in the management of patients with severe neurotoxic snake envenoming.
- RICU, respiratory intensive care unit
- SAV, snake antivenom
- neurotoxic snakebite
- snake antivenom dose
- mechanical ventilation
Statistics from Altmetric.com
Snake envenoming is a common medical emergency encountered in the tropics, and an estimated 35 000 to 50 000 people die of snake bite every year in India.1 The bites of elapid snakes (cobras) cause predominantly neurotoxicity, which manifests as paralysis of ocular, bulbar, limb and respiratory muscles.2 The management of these patients includes ventilatory support and administration of snake antivenom (SAV).
The dose of SAV required in the management of severe neurotoxic snake envenoming should be based on measuring serial venom concentrations in patients and determining when free venom concentrations are undetectable3; however, this is rarely clinically feasible. In the absence of any definite data,4 most recommendations are based on mouse assays, where the lethal dose is estimated to be around 120 mg of cobra venom and 60 mg of krait venom.5 The amount of venom neutralised by 1 ml of SAV is approximately 0.6 mg and 0.45 mg for cobra and krait respectively. Thus, empirically, the total SAV requirement for otherwise fatal cobra and krait bites is 200 and 134 ml respectively. However, this may not be true for human bites, as the exact total amount of venom injected by the snake at the time of bite is variable depending on the species and size of the snake, the mechanical efficiency of the bite, whether one or two fangs penetrated the skin, and whether there were repeated strikes. There is no consensus on the dose of SAV required in the management of snake bite, and selection of a particular dose of SAV is a controversial issue.
The aim of this study was to assess the effects of two different dosage protocols on the outcomes of patients with severe neurotoxic snake envenoming.
MATERIALS AND METHODS
The study was a retrospective analysis of patients treated at the respiratory intensive care unit (RICU) of this institute over the last 4 years. Patients with severe neurotoxic envenoming (defined as requirement of mechanical ventilation for ventilatory failure) were included in the study. Snake envenoming was diagnosed based on the history of snakebite and neurotoxic manifestations, presence of fang marks, presence of local manifestations such as swelling, cellulitis, and blister formation, or if the dead snake was brought in for identification.
Detailed history, findings of physical examination including site of bite, local reaction at the bite site and systemic features, and records of investigations including arterial blood gases, serum biochemistry, complete blood count, and coagulation profile were noted. Details of the dosage and schedules of SAV were recorded. Based on the prevalent practice in the RICU at different times, the patients could be divided into two groups. Group I (high dose group; before June 2002) received 100 ml of polyvalent SAV (Haffkine Institute, Mumbai, India) at presentation followed by 100 ml every 6 hours (no upper limit) until recovery of neurological manifestations. Group II (low dose group; July 2002–July 2004) received 100 ml of SAV at presentation followed by 50 ml 6 hours later. Neostigmine or other cholinesterase inhibitors were not administered to any victim.
The primary outcome measures were the duration of mechanical ventilation (time in hours from the onset of intubation to extubation) and the duration of RICU stay. Mortality and other complications during the RICU stay were also recorded.
Continuous variables were compared using unpaired Student’s t test and categorical variables using χ2 test. Survival curves were constructed to compare the duration of mechanical ventilation in the two groups using Kaplan-Meier analysis and log rank test.
RESULTS
During the study period, 55 patients were admitted, 27 in the high dose and 28 in the low dose group (table 1). Snake bite was confirmed by patient report, correlation between clinical manifestations, and recognition of snakes by patients and bystanders. Only three dead snakes were brought for identification: two kraits and one cobra. The exact species was not identified because of the non-availability of venom specific enzyme immunoassay.
Baseline characteristics and outcome of patients in low dose and high dose snake antivenom group
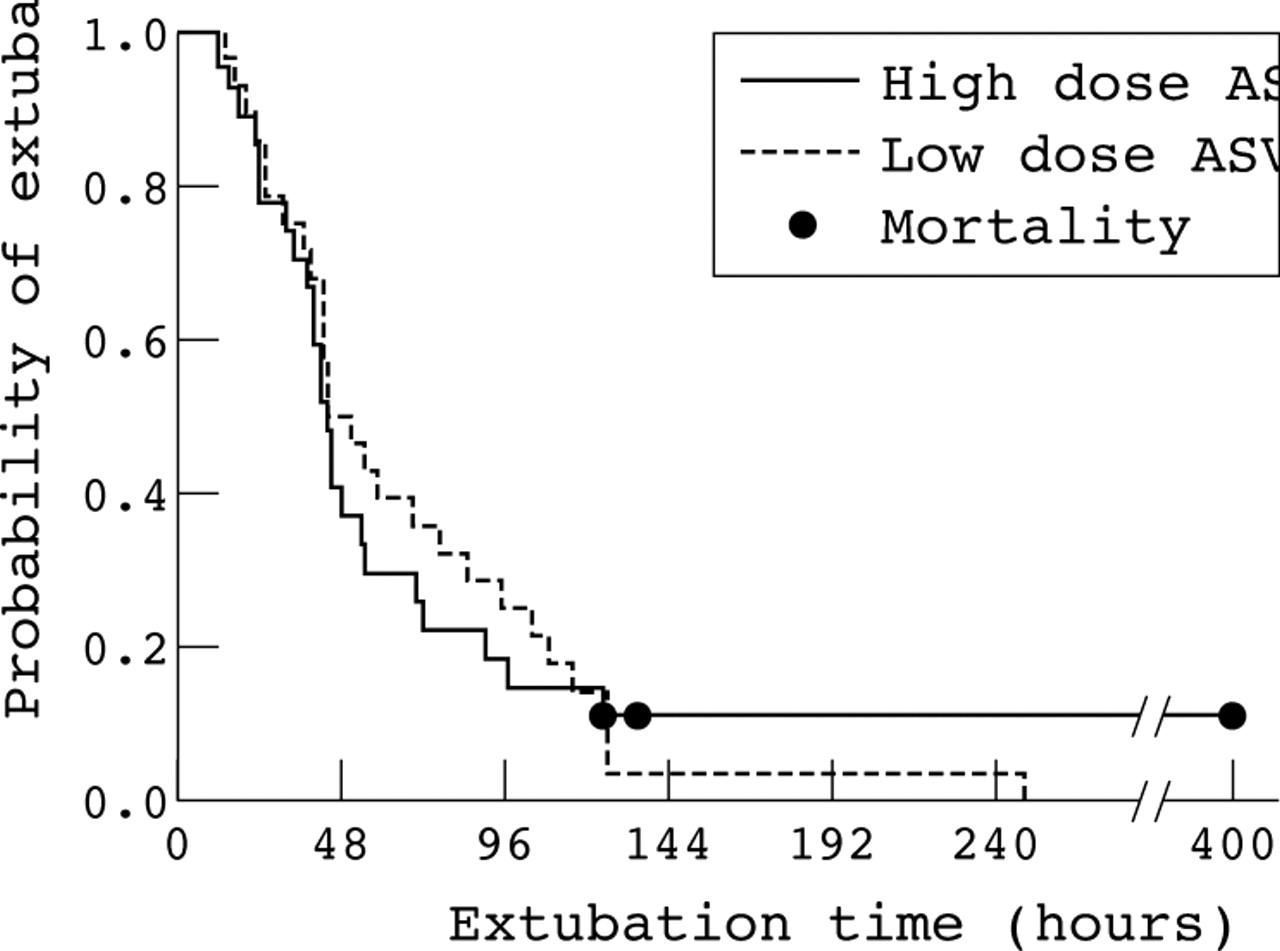
At admission, all patients had ptosis, dysphagia, diplopia, dysphonia, and evidence of hypercapnic respiratory failure (PaO2 <60 mmHg and PaCO2 >45 mmHg). None of the patients had any evidence of coagulopathy or renal failure at admission. The median dose of SAV in the high dose group was 600 ml (range 300 to 1600); all patients in the low dose group received 150 ml (table 1). Four patients in the low dose group and three in the high dose group showed hypersensitivity reactions to SAV, and were treated with promethazine and hydrocortisone. There was no episode of anaphylaxis. The mean duration of RICU stay was similar in the two groups (table 1). The median time to extubation in the high dose and low dose SAV groups was 44 and 47.5 hours respectively, and was not significantly different in the two groups using log rank test (fig 1). Two patients in the low dose group had ventilator associated pneumonia and one patient each in both groups had stress related minor gastrointestinal bleeding. There were three deaths in the high dose group. These three patients had probably sustained irreversible neurological damage before reaching the hospital and succumbed to complications related to ventilator associated pneumonia and sepsis. Two patients in the low dose group had residual neurological deficit in the form of extrapyramidal symptoms and myoclonic seizures at the time of discharge from hospital. All other patients improved and were discharged.

{kind=link}
Extubation times in the low dose and high dose snake antivenom (SAV) groups. The duration of mechanical ventilation was similar in the two groups (log rank test).
DISCUSSION
Neurotoxic snake envenoming is one of the most important causes of snake bite fatality1 and is mainly due to the Elapidae family, which includes the Naja and Bungarus species, commonly referred to as the cobras and kraits respectively. Neuromuscular paralysis in snake bite occurs as a result of blockade of neuromuscular transmission. Toxins from cobra venom predominantly act post-synaptically, whereas those of krait venom mainly act pre-synaptically; however, most snake venoms contain both pre-synaptic and post-synaptic neurotoxins.2,6 SAV is a specific antidote to snake venom actions, and is the only effective treatment for neutralisation of venom that has entered the circulation.
Although SAV has been used for many years, there is no universal consensus in many countries on the optimal dose and protocol of its administration. Theoretically, it would appear that patients with more severe envenoming need higher doses of SAV for effective neutralisation of circulating snake venom. In the absence of any recommendations for management of patients with severe neurotoxic envenoming, higher doses have been previously used in the hope of early recovery.4,7 However, because of the high cost and limited availability of SAV, and reports of patients with severe envenoming recovering without the use of SAV,8 there was a change in dosage protocols from high to low. Moreover, large doses of SAV may not cause any improvement in patients with presynaptic neurotoxicity, which is probably due to the irreversible effects of these toxins (although the clinical significance of pre-synaptic inhibition is difficult to assess6). The antivenom is effective only if given early enough to neutralise the venom in the circulation, prior to the neurotoxins reaching their target site, and thus prevent further development of neurotoxicity. Therefore, the use of large doses late in the course of envenoming is unlikely to be effective.
A few studies have addressed the issue of SAV dosage, but did not specifically include patients with severe neurotoxic envenoming, and outcome measures, especially the details on the duration of mechanical ventilation, were not particularly investigated.9–11 The present analysis was specifically conducted to evaluate if usage of a higher dosage of SAV offered any significant clinical advantage over a lower dose in patients with severe neurotoxic envenomation. We found no significant difference in the outcome between the two groups.
What are the advantages of using a lower dose of SAV? The economic significance of using low doses of SAV is obvious. Each 10 ml vial of SAV in India costs 400 rupees (approximately $9), and use of lower dosages could translate into huge savings to the patient and the community. In addition, there is an increasing shortage of SAV in several developing countries,12 and an important incentive for a regulated dosing protocol would be to prevent crisis of SAV availability and supply. Finally, the incidence of early anaphylaxis and late serum sickness-type reactions, which is related to the dose of SAV,4,13 can be decreased.
Our study has certain limitations. Firstly, the exact characterisation of the specific species was not performed by venom specific enzyme immunoassay, as this test is not routinely available. Secondly, the results of our study do not suggest that it should be applied to all snake bites. However, it definitely does suggest that lower doses of SAV may be as efficacious as higher doses in severe neurotoxic snake envenoming. Finally, laboratory assessments of SAV potency14 should serve as a guide to the use of antivenom dose in a particular region, and the onus thus rests on the clinicians to involve their patients in clinical trials to confirm the dose of SAV needed in their region.15
In conclusion, within the limitations of the present study, there is no difference between a protocol employing lower doses of SAV to higher dose in the management of patients with “unselected” severe neurotoxic snake envenoming.
Acknowledgments
The authors thank Dr Balamugesh, Dr C Reddy, and Dr A Nath for their help while carrying out the study.
Footnotes
-
Competing interests: none declared
Linked Articles
- Primary Survey