Article Text

Abstract
Acute opioid intoxication and overdose are common causes of presentation to emergency departments. Although naloxone, a pure opioid antagonist, has been available for many years, there is still confusion over the appropriate dose and route of administration. This article looks at the reasons for this uncertainty and undertakes a literature review from which a treatment algorithm is presented.
- AWS, acute withdrawal symptoms
- naloxone
- opioid
- overdose
- poisoning
Statistics from Altmetric.com
Although naloxone has been used as a specific antidote for opioid poisoning since the 1960s,8 there are variations in the recommended doses with the British National Formulary advising 0.8–2 mg boluses, repeated as necessary up to 10 mg for adults (10 µg/kg followed by 100 µg/kg boluses for children), and Poisindex suggesting 0.4–2 mg boluses. There is also wide variation in the route of administration.
There are a number of reasons for this. First, opioids exert their effect by binding to a series of receptors. Naloxone has antagonist activity at all of the receptor types9 and the amount needed to provide such an effect depends upon the number of receptors occupied. Recent evidence suggests that a dose of 13 µg/kg naloxone (approximately 1 mg in an 80 kg person) produces 50% receptor occupancy;10 however, this is also influenced by the dose of opioid ingested or injected. Unfortunately this is seldom known in clinical practice,11 and instances have been reported where over 20 times the recommended doses of naloxone have been needed to counteract massive opioid overdoses,12,13 and even more in body packers. Numerous case histories have revealed a 13-fold variation in rate of naloxone infusions given for prolonged overdoses.14–22
Second, opioid antagonists can precipitate acute withdrawal symptoms (AWS) in chronic opioid users11,23–28 provoking an often violent reaction. In one early study on the use of naloxone to reverse morphine anaesthesia in non-opioid dependent, general surgical patients, acute withdrawal-like symptoms were observed to occur after the administration of 15 μg/kg naloxone.29 In another study, behavioural changes, sweating, and yawning were observed in 14 healthy volunteers given 2–4 mg/kg naloxone, and these effects often lasted for a number of hours after its administration.30
Third, the pharmacodynamic actions of naloxone last for a briefer period than all but the most short acting opioids;8,24,29,31 although the elimination half life of naloxone is similar to that of morphine (60–90 minutes)9 it is redistributed away from the brain more rapidly.32 Consequently, the patients may become renarcotised and suffer harm if they self discharge from medical care early. Clinicians are clearly walking a tightrope between precipitating AWS and avoiding renarcotisation.
Numerous case reports describing possible adverse effects of naloxone have been published. Pulmonary oedema has been reported but most instances have occurred in the postoperative period33–39 or in the presence of pre-existing cardiorespiratory disease,40 and in many of these reports it can be difficult to differentiate between the effect of naloxone and the effect of the underlying disease process or other drugs that have been ingested or administered. Many episodes of pulmonary oedema secondary to opioid toxicity have been published since it was first noted by William Osler in the 1880s5,41–50 and it has been suggested that naloxone simply reveals the opioid induced pulmonary oedema that had been masked by the respiratory depression.51
Seizures52 and arrhythmias53–57 have also been noted, but could have been caused by hypoxia,54 the opioids themselves,44,55,58 their coingestants (most notably cocaine),57 or pre-existing disease.53,56 Interestingly, a number of episodes of severe hypertensive reactions have been reported following administration of naloxone to patients with pre-existing simple hypertension.59–63 In addition, one report showed a significant rise in serum catecholamine concentrations in a patient with a phaeochromocytoma following administration of naloxone without prior exposure to exogenous opioids.64 Currently, a great deal of research is being undertaken on the interaction of endogenous opioids and the autonomic nervous system and it would seem reasonable to postulate that the antagonistic action of naloxone may have an effect. Canine experiments have indicated that reducing hypoxia and hypercapnia lowers serum catecholamine concentrations. It has been proposed that hyperventilating patients prior to administration of naloxone would reduce the risk of sympathetic mediated adverse effects,58,65 although this has not been verified in human.
In contrast with the above concerns, extremely high doses (up to 5.4 mg/kg boluses and 4 mg/kg/h infusions) of naloxone have been given to non-opioid dependent subjects without any reported adverse effects.66–68
The aim of this review is to find evidence of the optimum dose and route for administration of naloxone and for how long patients need to be observed before it is safe to discharge them.
METHODS
The Medline and Embase databases were searched using the following terms:
“naloxone or naloxone” and “narcotics or opioid or opiate” or “morphine or buprenorphine or codeine or dextromoramide or diphenoxylate or dipipanone or dextropropoxyphene or diamorphine or dihydrocodeine or alfentenil or fentanyl or remifentanil or meptazinol or methadone or nalbuphine or oxycodone or pentazocine or pethidine or phenazocine or tramadol” and “overdose” or “overdos$” or “poisons” or “poison$” or “acute intoxic$” or “acute toxic$” and limited to human studies.
Studies were deemed to be relevant if they compared doses and routes of administration of naloxone or if they produced evidence about rates and timing of complications. Case histories were reviewed but were included only if they could be reasonably grouped together for comparison.
All papers, including review articles and case histories, had their references scrutinised for further articles that were in turn retrieved and reviewed; this process was repeated until no further articles were found (a total of five rounds).
SEARCH RESULTS
The initial search produced 185 papers; the subsequent series of reference reviews produced 10 relevant articles.65,69–77 These papers are summarised in tables 1 and 2, which can be found on the electronic version of this article.
DISCUSSION
Effect of dose on AWS
AWS include agitation, nausea, vomiting, piloerection, diarrhoea, lacrimation, yawning, and rhinorrhoea; these are generally not life threatening.78 Reported rates of AWS related complications vary widely from 7–46% with 2–4 mg boluses70,72,73,76 to 47% with a median of 0.9 mg;71 however, the actual outcome measures were not directly comparable. Only one study records AWS (12%),72 with one US paper quoting the number of patients (7%) who required restraint (presumably the most severely affected patients)76 and the other studies describing the proportion of patients who discharged against medical advice (18–47%).70,71,73 Patients self discharge for many reasons—for example, fear of police involvement—so that the numbers who do abscond do not necessarily equate to those who experience AWS, although clearly they are no longer narcotised in order to be able to leave the emergency department.
Another potential problem in interpreting the data is the lack of information comparing absolute doses given and rates of administration with AWS, and state of drug dependency/tolerance prior to AWS. Wanger’s study77 stated that the paramedics had the impression that patients who were given naloxone subcutaneously had a smoother emergence than those given it intravenously in spite of a larger dose. It is likely that this is because of a slower increase in concentrations at the receptors, but further research would be needed to confirm this; it may also reflect paramedics’ preference for an easier route of administration.
Effect of dose on recurrence of toxicity
Four papers quote the percentage of patients who require a second dose of naloxone,72,74,76,77 again with marked variation across the world and between centres in the same country. Watson’s72 and Sporer’s76 patients were given 2 mg boluses, and 14% and 35%, respectively, were given a second dose. In Christenson’s74 and Wanger’s77 studies, patients were given either 0.4 mg intravenously or 0.8 mg subcutaneously, with 55% overall having further naloxone in the former study compared with 15% (subcutaneously) and 35% (intravenously) in the latter paper. This marked variation may be explained by the studies having different thresholds for giving further doses of naloxone as opposed to treating the patients conservatively, as well as very different half lives of opioids taken—heroin versus methadone.
Watson72 found that recurrence of toxicity was significantly more likely when long acting opioids were ingested, although route of opioid administration and use of coingestants surprisingly did not have any noticeable effect.
Route of administration of naloxone
Only two papers compared routes of administration.76,77 Both studies used different criteria to define opioid intoxication (in terms of history and clinical findings) and naloxone was given in the prehospital setting; therefore, it is difficult to generalise the findings to other patient populations. In spite of these concerns, Sporer76 showed that 2 mg naloxone intramuscularly works as well as 2 mg intravenously (94% and 90% response rates, respectively); this is perhaps not surprising considering the relatively large dose given and it was not possible to distinguish differences in complication rate between the study groups.
Wanger’s study77 revealed that 0.8 mg naloxone subcutaneously worked as rapidly as 0.4 mg intravenously from time of arrival at the patient’s side to time of clinical effect, because the slower time of effect from administration was offset by not having to gain intravenous access first.
Neither of these studies settles concerns about unpredictable and erratic absorption from the intramuscular/subcutaneous injection sites in those patients who are hypotensive, but they may be useful alternative routes when intravenous access is difficult to obtain. No studies have evaluated the absorption kinetics of intramuscular administration of naloxone. It is likely that variables—including depth of injection, dose given, muscle blood flow, site, and so forth—would all alter the kinetics of absorption by the intramuscular route, particularly in the opioid poisoned patient with hypotension.
Recent case series and reports have suggested that both intranasal79,80 and nebulised81 naloxone may be effective, although they are subject to similar unanswered pharmacokinetic concerns. Also, there is no evidence about the rates of renarcotisation and AWS.
Goldfrank’s study75 provides a good practical dosing guide for patients who require prolonged opioid antagonism. It was a small study where the end point measured plasma naloxone levels and not clinical effect; however, it claimed only to be an initial guide to treatment, and stressed the importance of close observation of the patient and titration of dose as necessary. This makes sense because of individual tolerance and susceptibility to opioids—for example, clinical observation has shown that corpulent patients will absorb opioids into fatty tissues from which it is expected to redistribute out more slowly and such patients tend to need more prolonged naloxone infusions. Further research is required to validate formally and prospectively the Goldfrank protocol.
Timing of complications
Christenson et al74 suggested that if patients fulfilled certain criteria 1 hour after administration of naloxone then they could be discharged safely. However, one of their patients who had taken heroin needed further naloxone after 2 hours and Watson et al72 similarly noted that patients who had taken long acting opioids developed renarcosis up to 2 hours after their initial treatment. Since the half life of naloxone is 60–90 minutes, it would seem logical to observe patients for signs of recurrent toxicity for at least 2 hours, although further studies are needed to validate this.
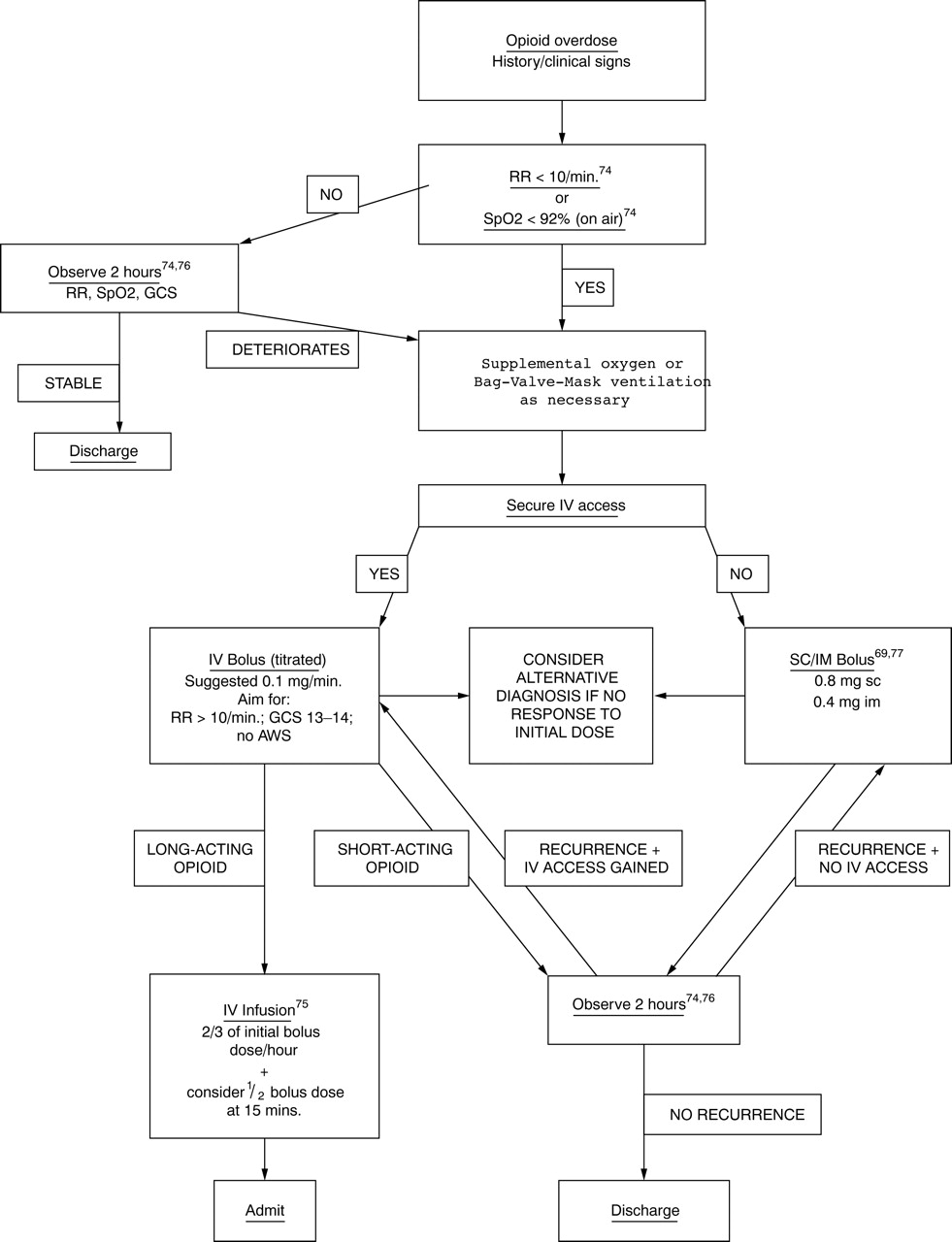
{kind=link}
Flowchart of treatment of opioid overdose.
With one exception, all other serious complications became apparent within 20 minutes of arrival and treatment in the emergency department.65,70,71 The one exception was a case of fatal pulmonary oedema, where the patient was found dead 7 hours after discharge (9 hours after ingestion of opioid). In this case, further opioid ingestion cannot be ruled out, and in any case it would seem that genuinely delayed adverse events are rare. Because it would be difficult to persuade opioid addicts to stay for 8 hours after they have had naloxone, it would be reasonable to discharge them if they fulfil Christenson’s criteria 2 hours after naloxone.
Research difficulties
The reasons for the dearth of randomised controlled clinical trials have been summarised recently by Whyte et al.82
Legal, political, and ethical difficulties, particularly in the context of obtaining consent, often hinder the recruitment of adequate numbers of patients. In addition, trials would have to be prohibitively large to achieve sufficient power when measuring outcomes that are rare.
It is difficult to eliminate confounding factors, such as the wide range of different opioids, co-ingestants, and adulterants that can be taken, the variety of routes by which they can be taken (orally, intravenously, subcutaneously, nasally, or by smoking), and the complex treatment regimes that are given. It is often difficult to determine what individual patients have taken because usually they do not know.
The external validity of the studies can be questioned because many are undertaken in regional poisons centres whereas most patients are treated in general hospitals where there is limited access to specialised toxochemical laboratory facilities. Similarly, it can be argued that patients who agree to participate in research are not representative of the whole population of opioid overdose patients.
Blinding of treatments is extremely difficult because patients are often in the emergency department for such a short period before they are discharged that the clinician who administers the treatment is usually the one who has to review the response to that treatment.
The research undertaken so far has relied heavily on observational studies, which have a number of well recognised limitations, such as difficulty in minimising confounding factors and retrospective data collection. Studies have often used different inclusion criteria in terms of degrees of sedation and respiratory rate as well as different thresholds for giving further doses of naloxone, which makes direct comparison of studies difficult.
Follow up of patients is difficult; Smith et al70 managed to contact only 32% of the patients who had been discharged. Other studies compared the lists of patients discharged with ambulance service records and death certificates issued by the local coroners. They may have been lost to follow up if they had given misleading demographical details and after discharge were taken to another healthcare facility by private transport, or if they had died later and been given an alternative cause of death.
In spite of these difficulties, a number of conclusions can be drawn but further trials are needed to validate them clinically in the emergency department and thus help clinicians walk the tightrope between over and under treating these patients. Clinical judgement and meticulous observation are required to successfully manage opioid intoxicated patients.
CONCLUSIONS
Although the evidence base is sparse at present, the following algorithm has been devised to summarise the research in a way that is clinically useful. References have been included where relevant otherwise the recommendations are based on consensus derived from the clinical experience of Medical Toxicology Units in Europe, the USA, and Australia. Although recent studies have suggested that intranasal and nebulised naloxone may be useful alternatives to parenteral administration, the authors think that the evidence is not strong enough yet to add them to the algorithm; however, they could be easily included in the flowchart as further evidence becomes available.
Opioid overdose is a challenging condition that requires a difficult balancing act between over and under treatment with naloxone.
REFERENCES
Footnotes
-
Competing interests: none declared