Article Text

Abstract
Objectives: To review compliance with our emergency department (ED) guideline on the imaging of ingested non-hazardous metallic foreign bodies in children, investigate adverse outcomes, and make suggestions for improving the guideline.
Methods: Retrospective analysis of patients presenting in a 3 year period to a paediatric ED with a history of possible metallic foreign body (MFB) ingestion, who were managed according to an ED guideline.
Results: We identified 430 episodes of possible MFB ingestion, of which 422 were eligible for inclusion in the study. Compliance with the guideline was 77.8% with no significant adverse events. The exclusion of symptoms as a criterion for x ray results in a reduction in the x ray rate of 56% in the symptomatic group with no increase in adverse events.
Conclusion: A handheld metal detector (HMD) can be safely and reliably used in lieu of plain radiography to investigate children with a history of MFB ingestion, irrespective of symptoms and without incurring any significant adverse events.
- ED, emergency department
- HMD, handheld metal detector
- MFB, metallic foreign body
- children
- foreign body
- metal detector
- radiography
Statistics from Altmetric.com
Possible foreign body ingestion is a common reason for children to present to an emergency department (ED). Metallic foreign bodies (MFBs) are more commonly implicated than non-metallic, with coins being the most common.1–3 Although most ingested MFBs pass spontaneously into the stomach and through the gastrointestinal tract without sequelae, impaction in the oesophagus is a recognised and potentially serious complication with oesophageal ulceration, perforation, fistula formation, mediastinitis, and respiratory compromise (including aspiration) having all been reported.4–7 Standard investigations recommended in otolaryngology and emergency medicine texts and performed in most ED include plain radiography of the neck and chest to identify MFBs lying within the oesophagus.7,8 However, several authors have demonstrated the high sensitivity and specificity of a handheld metal detector (HMD) in identifying oesophageal MFBs.1,2,9,10 It has been noted that HMD as well as replacing plain x rays can identify some radiolucent MFBs, such as aluminium ring pulls.11 Despite these findings, many departments have continued to utilise plain radiography as their primary investigative tool. A guideline for investigating suspected MFB ingestion was introduced at the Sheffield Children’s Hospital in 2000 (fig 1). This paper seeks to review compliance with this guideline, investigate any adverse events, and make recommendations for improvements.
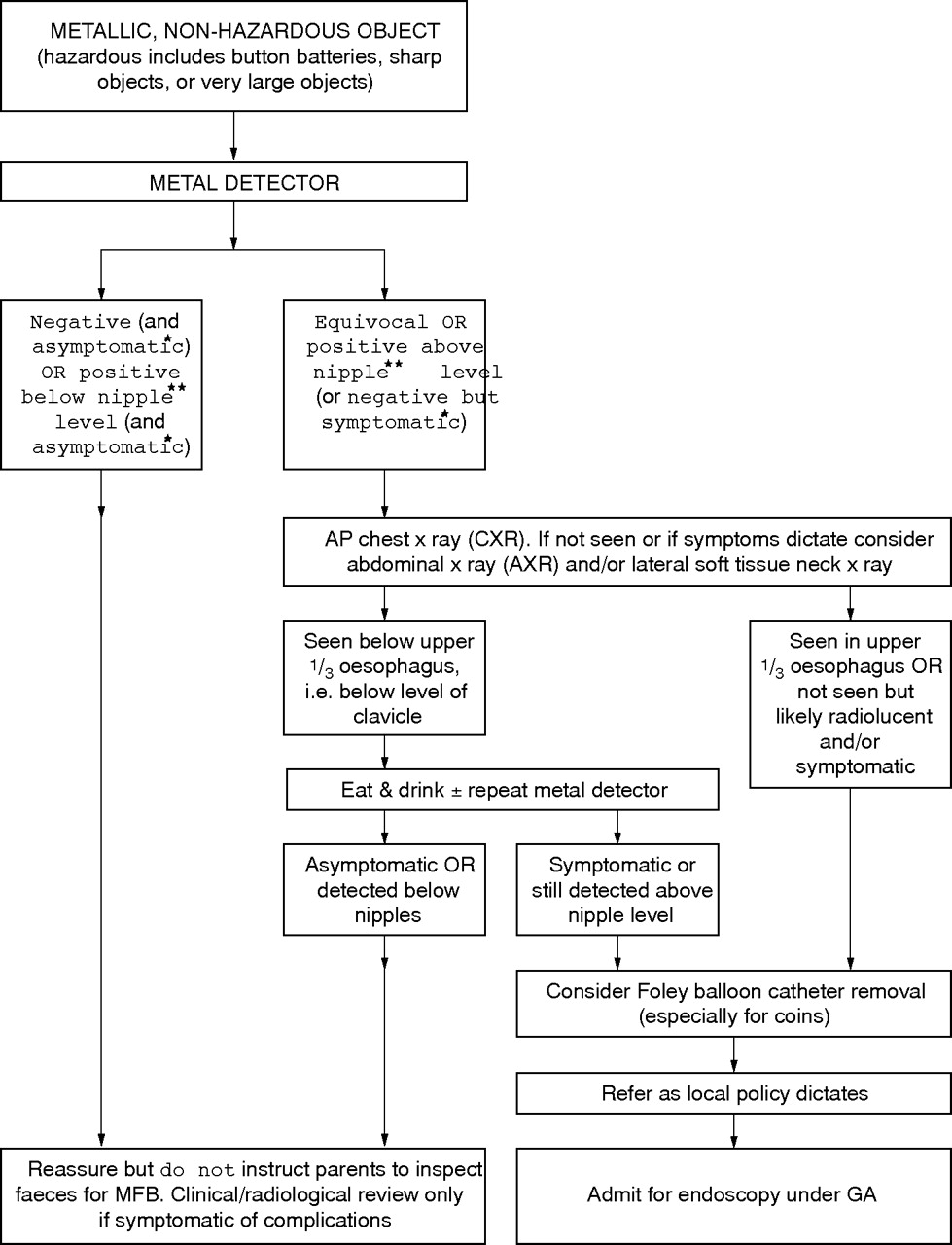
Management of ingested metallic foreign bodies. *Text related to symptoms, which we suggest be removed from the algorithm. **Nipple level should be changed to xiphisternal level.
METHODS
In the ED at Sheffield Children’s NHS Trust, children with a history of possible ingestion of an MFB are investigated according to a standard guideline (fig 1). The HMD examination is performed using the C.Scope HHB handheld locator (C.Scope International, Ashford, Kent, UK) by radiographers trained in its use but with variable experience. All new radiographers undergo in-house training in the use of the HMD, according to the manufacturer’s instructions, and observe demonstration of its use before being deemed competent. This training does not last more than 1 h initially, but is supplemented by radiology department guidelines and readily available assistance from more experienced practitioners if necessary. Similar accuracies in identifying MFBs by practitioners of varying experience has been demonstrated in earlier studies.2,10
All metallic objects, for example jewellery, is removed and non-removable metal, for example fillings and sternal wires, are noted. Children stand upright or are held by their parents with their trunk extended (fig 2). The HMD is checked on a metallic object such as the examiner’s watch, and then passed from the level of the nasopharynx, moving caudally across the chest and upper abdomen to the symphysis pubis. Radiographers examine the back and perineum at their discretion. A positive signal gives a visual and auditory alarm. An oesophageal MFB is indicated by a positive signal when any part of the HMD is above the nipple line, with a positive signal below this level considered indicative of location in or distal to the stomach. An equivocal signal is reported where the examiner is unable to definitely allocate the positive signal as above or below this level.

{kind=link}
{kind=link}
A child being examined. (Photograph is reproduced with consent.)
As the ED at Sheffield Children’s Hospital is the only department seeing children under the age of 15 in Sheffield, we assumed that any unplanned returns with complications would have presented to this department (cross boundary flow 2% with neighbouring departments12).
We retrospectively identified all children presenting to the ED with a history of possible MFB ingestion for the period April 2000 to March 2003. This was achieved by extraction of computerised ED discharge coding and radiology department coding of foreign body ingestion or HMD examination. Case notes for all attendances including and subsequent to the initial presentation with a possible MFB ingestion were examined, and freehand data extracted. To minimise the chance of missing data, this database was cross referenced with the main hospital attendance database and with the radiology department database of radiographs performed. Microsoft Excel 2000 was used to enter and analyse data. Ethics approval was deemed unnecessary as this was an observational study and no identifiable patient characteristics were used.
RESULTS
We identified 430 episodes of attendances by children with a history of possible ingestion of an MFB during the 3 year study period. One child’s notes were missing and seven children had no HMD report available. These eight cases were excluded from analysis leaving 422 cases for review. None of these children had any adverse outcome, and none had an oesophageal MFB. The male to female ratio was 1.1:1 (221:201) and mean age at presentation was 4.2 years (range 2 months–15 years). Table 1 gives a breakdown of the frequency distribution of objects ingested. Coins were the most commonly ingested objects (67.5%, n = 285).
Types of objects ingested
A total of 268 children (63.5%) had a time of ingestion recorded, and from this a time to presentation could be calculated. Mean time to presentation was 607 min (range 10 min to 14 days) with 180 children (67%) presenting within 2 h and 213 (79.4%) within 4 h.
Table 2 summarises the data. Of the 422 patients eligible for inclusion in the study, 61 (14.5%) with symptoms and HMD indicating a foreign body below the nipple could not be mapped to any of the categories in the algorithm
Summary of data
Table 3 summaries the x ray outcome for the 361 patients who were mapped to categories in the algorithm.
Radiography performed
Overall, the care of 281/361 (77.8%) patients complied with the algorithm.
We next investigated whether any adverse events occurred. An adverse outcome was defined as any unplanned re-attendance with symptoms or complications relating to the original episode, including any clinically important missed MFBs.
Of the 61 patients who did not map to the guideline (symptomatic patients with HMD indication of foreign body below the nipples), 56 had no x ray with no adverse outcome. Of the remaining five (who had an x ray), three were defined as having an adverse outcome: one was found to have ingested a screw and was referred to the surgeons for follow up, one had an x ray before HMD because of an episode of cyanosis at the time of ingestion, and the third had a foreign body in the lower oesophagus. None required intervention and all foreign bodies passed without event, as confirmed by repeat HMD examinations.
Of the 64 patients with no indication for an x ray who had an x ray (group B in table 3), 51 were negative for a foreign body and 13 had a foreign body in or distal to the stomach.
Eighty four children with a negative HMD examination still had radiography performed. Twelve (14%) of these were reportedly positive for an MFB. Five of these radiographs were performed for technical reasons (difficult HMD, uncertainty about metallic nature of foreign body). One child’s x ray was initially interpreted by an ED doctor as possibly projecting an MFB over the larynx, as the child reported swallowing a small watch. He had negative endoscopy with an uneventful clinical course, and the x ray was subsequently reported as being normal. There were no other adverse events in any of these children.
There were no adverse outcomes in the 16 individuals with an indication for x ray on the guideline who did not receive an x ray (group C in table 3). Two of these children had HMD indication of a foreign body above the nipples, followed by a patient report of MFB movement and subsequent repeat HMD examination clearly confirming a position below the nipple line.
There were no adverse outcomes in the 226 patients with no indication for an x ray who were not x rayed (group D in table 3). There were two unplanned returns, one with an unrelated diarrhoeal illness and a second because the parents had been sifting through the stool for 2 weeks to look for the foreign body (DON’T!). It should be emphasised that it is clearly documented in the guideline to advise parents NOT to do this.
Twenty three children (5.4%) were referred. There were seven successful balloon catheter removals in the ED, four failed catheters proceeding to endoscopy, six endoscopies, and the remainder were observed and subsequently discharged without intervention.
Overall there were no significant adverse outcomes for any of the patients in the study for a minimum of 9 months after the last presentation used in the data collection.
Calculation of sensitivity and specificity was performed using data from patients who had radiological in addition to HMD examination (n = 124). Overall sensitivity was 78% (95% CI: 64% to 88.5%) and specificity 98.6% (95% CI: 92.7% to 100%). For coin-like objects only (n = 57), calculated sensitivity was 88.9% (95% CI: 70.8% to 97.6%) and specificity 96.7% (95% CI: 82.8% to 99.9%).
DISCUSSION
The use of an HMD was first described to track a foreign body through the gastrointestinal tract in 1980 by Lewis.13 Studies with various other HMDs carried out over the subsequent 20 years demonstrated sensitivities of 95–100% and specificities of 82–93%.1,2,9,10 As there are no published sensitivity or specificity data for the particular HMD used in our study, we cannot exclude the chance of some variability in the quoted figures. There are industry standards for this type of equipment, however, so we do not expect significant variation in sensitivities. There has continued to be reluctance in using the HMD as the main investigative tool for MFB ingestion. This may be because of availability, unfamiliarity with the device, lack of training, lack of evidence regarding safety, and parental and even physician scepticism.
The advantages of the HMD over plain radiography include avoiding radiation exposure, speed, ease of use with minimal training, low cost, and the ability to detect radiolucent materials such as aluminium. The HMD can also be used to avoid serial “exploratory” radiographs by defining the general anatomical location of MFBs which require mandatory radiography to plan definitive management.
As we did not confirm HMD findings with plain radiography in all patients, an accurate calculation of sensitivity and specificity for the entire study population was not possible. From the subset of patients who had both HMD and x rays, the calculated sensitivities suggest that the HMD is not as accurate in identifying non-coin-like MFBs. This is also suggested by other authors.14 Sensitivity calculations have been performed on very small numbers of non-coin-like MFBs, both in this and in prior studies.14 Coupled with the huge variation in type, size, and metal content of the non-coin MFBs, we believe that the actual sensitivity for selected non-coin-like MFBs may actually be similar to that reported for coin-like MFBs. In our study, the nature of the MFB did not appear to predict adverse outcomes (including clinically significant missed MFBs).
Previous studies have shown that symptoms alone are poor predictors of oesophageal MFBs.1,5,6 Our study confirms this finding with only 13.9% of symptomatic children having an oesophageal foreign body. We believe that ability to eat (swallow) may be a better discriminator than general symptoms in identifying possible oesophageal MFBs.
In the asymptomatic group of patients, only 11/301 (3.7%) met the criteria for having an x ray, leaving little scope to review the guideline for a further reduction in x ray rates. In the symptomatic group, all 121 patients met the criteria for x ray by virtue of having symptoms. We reviewed, in light of the study, the symptom criteria included in the guideline.
If symptoms were excluded from the criteria for an x ray, then in the symptomatic group only 19/121 (15.7%) would meet the anatomical criteria for x ray (above the nipple or equivocal), and 102/121 (84.3%) would not meet the anatomical criteria (below the nipple or no foreign body detected). Of these 102, none had an adverse outcome and therefore could have safely been managed on the HMD result alone. Exclusion of symptoms from the x ray criteria would have reduced the number of symptomatic patients x rayed by 27/60 (45%). See fig 1 for the suggested new guideline.
It may also be reasonable, in equivocal cases, to allow the child to eat and then repeat the HMD exam, therefore x raying only if the result is still equivocal. This may further reduce the x ray rate.
There may appear to be a discrepancy between studies as to the reference point for an oesophageal foreign body. Our original guideline suggests that a positive HMD above the nipple line indicates an oesophageal foreign body, while others suggest a positive HMD above the xiphisternum indicates an oesophageal foreign body.14 We believe this discrepancy is a function of the design of the HMD and definition of the reference point relative to the HMD. Our HMD is 8 cm wide and detects foreign bodies across the whole width. When we define a positive signal below the nipple line, the upper edge of the HMD is placed at the nipple line. In reviewing a number of both adult and child patients, we feel that the reference to “below the nipple line” could mean that the lower edge of the HMD lies at the level of the xiphisternum and could be interpreted as being above the xiphisternum. Our current reference to the internipple line may account for our one lower oesophageal foreign body which was reported as below the nipple line. It may be best to define the reference point in terms of the entire HMD lying either above or below the given reference level. There may also be more variability in the level of the nipple line as a surface landmark corresponding to the lower gastro-oesophageal junction or diaphragm. To avoid potential confusion, we suggest that the level of the xiphisternum may be a simpler and more constant landmark to use.
It should be stressed that ingestion of a potentially hazardous foreign body mandates radiography. The HMD is useful in identifying the region of the body for imaging but should not preclude x ray confirmation, even if negative for a signal. Potentially hazardous foreign bodies include sharp objects, very large objects, button batteries, and filled balloons.
Any retrospective study risks cases being missed. We have attempted to minimise the chances of this occurring as outlined in our methods. Unfortunately, there is still a chance of multiple coding errors, undocumented HMD use, and of children with complications presenting elsewhere.
This study demonstrates that the HMD can be safely and reliably used in lieu of plain radiography to investigate children with a history of metallic non-hazardous foreign body ingestion, provided a clear guideline is followed. Use of the algorithm in conjunction with trained HMD operators has resulted in a substantial reduction in the number of radiographs taken in a children’s hospital over a 3 year period. No adverse events have been identified in that time. We have suggested additional refinements to the guideline, which would make it clearer and allow for further reduction in radiography.
Acknowledgments
We thank Mr S Marven, Dr P Broadley for the initial guideline, and Dr I Seymour for assisting with data collection.
REFERENCES
Footnotes
-
Funding: none
-
Competing interests: none declared