Article Text

Abstract
Background and aims: Early treatment is critical for successful intervention in acute stroke. The aim of this study was to describe delays in presentation to hospital and in the emergency department (ED) management of patients with acute stroke and to identify factors influencing these delays in an Italian urban hospital.
Methods: The present series includes all patients presenting with acute stroke, in whom arrival delay was ascertainable. To describe delays into the ED, the triage–visit delay, visit–computed tomography (CT) delay and visit–CT report delay were registered. Type of stroke, severity of stroke assessed using the modified National Institute of Health Stroke Scale (mNIHSS) scale, level of consciousness, history of previous stroke or previous hospital admission, use of the emergency medical service (EMS), onset of stroke during day or night and admission during working or non-working day were registered for every patient. Univariate and multivariate analysis were performed to evaluate factors influencing early arrival.
Results: Over a one-year period 537 patients with acute stroke were evaluated; 375 patients in whom arrival delay was ascertainable were included in the study. Median arrival delay was 5.4 h (interquartile range (IQR) 2.7–11.6); 104 patients (28%) arrived within 3 h and 198 (53%) within 6 h. Triage–visit delay was 0.3 h (IQR 0.2–0.7), visit–CT scan delay was 1.2 h (IQR 0.8–1.9), visit–CT report delay was 2.7 h (IQR 1.7–4.5). Triage–visit delay and visit–CT delay were shorter for patients presenting within 3 h. The type of stroke was ischaemic in 240 (64%), haemorrhagic in 61 (16%) and transient ischaemic attack in 74 (20%). The median basal mNIHSS score was 5 (IQR 3–10); 64 patients (17%) had an altered level of consciousness, 103 (27%) had had a previous stroke, 223 (59%) had had a previous hospital admittance. In this series 214 patients (57%) arrived with the EMS, 323 (86%) presented with symptoms during the day, 261 (70%) were admitted during working days. Univariate analysis showed a significantly shorter arrival delay in patients calling the EMS (median 4.2 vs 7.2 h; p<0.001) and in patients with a higher basal mNIHSS score (Spearman ρ = −0.204; p<0.001) or altered level of consciousness (normal 5.8 h, not alert but arousable 3.8, not alert but arousable with strong stimulation 2.5, totally unresponsive 6.0; p = 0.005). Multivariate analysis showed that use of the EMS and higher basal mNIHSS score were independent variables associated with a shorter arrival delay.
Conclusion: A substantial proportion of patients does not arrive at the ED in a suitable time for reperfusion therapy. Patients using the EMS have a shorter arrival delay. Approximately half of the patients with stroke are sufficiently aware of the urgency of this clinical condition to activate the emergency telephone system.
Statistics from Altmetric.com
Stroke is a world leading cause of death and long-term disability and is associated with high costs.1 A recent epidemiological Italian study reported an annual incidence of 153 000 new cases in the elderly population.2 Early hospital presentation is crucial for optimising the benefit of intervention, as well as for the feasibility of effective treatment; in fact, thrombolytic therapy is dependent on rapid intervention.3 Current guidelines from Italian,4 European5 and American associations6 recommend intravenous thrombolysis for patients who can be treated within 3 h from the onset of ischaemic stroke and intra-arterial thrombolysis for patients with stroke caused by large vessel occlusion of less than 6 h duration. Clinical studies suggest that cerebral ischaemia persisting more than 6 h results in permanent neurological damage.7 Early hospital arrival is thus critical for successful stroke treatment. A number of studies have evaluated time delay in stroke care8–21 and some have investigated the causes of the delay. Some of these studies were conducted in north America8–16 and others in Europe.17–21 Only one study was conducted in Italy in the early 1990s;22 since then, the Italian healthcare system and in particular the emergency medical service (EMS) has been reorganised.
The aim of this study was to describe delays in presentation to hospital and in the Emergency Department (ED) management of patients with acute stroke and to identify factors influencing these delays in an Italian urban hospital.
SUBJECTS AND METHODS
Hospital setting and patients
The study was conducted in the ED of the Foundation IRCCS, Ospedale Maggiore Policlinico, Mangiagalli Regina Elena of Milan, Italy, a teaching hospital located in the centre of the city that serves a large surrounding urban area. All patients presenting to the ED with signs and symptoms of acute stroke and admitted to hospital with a diagnosis of acute cerebrovascular event were considered eligible. A major criterion for inclusion was the possibility to establish the time of stroke onset and consequently the arrival delay. Patients with subarachnoid haemorrhage, chronic subdural haematoma and in-hospital stroke were excluded. A brain computed tomography (CT) scan was performed in all cases.
Data collection
Since 2003 in our ED the management of patients with possible cerebrovascular disease has been standardised; a trained nurse at triage applies the Cincinnati Stroke Scale and all patients with focal neurological signs follow a diagnostic protocol. The present series refers to data collected during a one-year period, from 1 September 2003 to 31 August 2004. Data were collected before the hospital authorisation for thrombolytic treatment in the SITS–MOST study. All data were reviewed by the authors on medical records. All the data were anonymised before analysis to ensure confidentiality.
Arrival delay was defined as the time from the clinical onset of stroke, reported by the patient or an attending relative to the ED physician and recorded in a computer-based manner. When the precise hour of onset was not reported, additional information about the timing found in the medical records was used to approximate the time of stroke onset and arrival delay. Onset defined as “in the morning” was registered at 07:00 hours, “before lunch” at 12:00 hours, “after lunch” or “this afternoon” at 14:00 hours, “this evening” or “before dinner” at 18:00 hours, “after dinner” at 19:00 hours. When symptoms were first noted on awakening, the previous midnight was recorded as the time of onset. Patients for whom the time of onset was not documented or could not be approximated reasonably were excluded.
To describe the evaluation process inside the ED, we registered the delay from triage to the ED physician visit (triage–visit delay), from the ED visit to CT scan execution (visit–CT delay) and from the ED visit to the radiologist report of the CT scan (visit–CT report delay). Door to needle delay was not registered in the overall series; it was reported in only a small proportion of patients enrolled in the SETIS study, an ongoing treatment trial (randomised, double blind treatment with tirofiban versus acetylsalicylic acid) coordinated by our hospital.23
Among factors possibly influencing arrival delay we considered: age; sex; history of arterial hypertension; diabetes or atrial fibrillation; previous stroke; previous hospital admission for any cause; type of stroke; stroke severity; level of consciousness; use of the EMS (telephone number 118); onset of stroke during day or night; admission during working or non-working day.
Type of stroke was classified as ischaemic, haemorrhagic or transient ischaemic attack (TIA). Ischaemic stroke was defined as the persistence of clinical signs for more than 24 h or the development of an ischaemic lesion at the 48–72 h brain CT scan. Haemorrhagic stroke was defined as the presence of intracerebral haemorrhage. TIA was defined as a brief episode of neurological dysfunction caused by focal brain or retina ischaemia, with clinical symptoms typically lasting less than a few hours and without subsequent evidence of acute infarction.24
Stroke severity was assessed by the modified National Institute of Health Stroke Scale (mNIHSS) score. The mNIHSS score, when not obtained on admission, was deduced by the neurological examination as validated in a previous study;25 this scale ranks from 0 to 31 points the severity of neurological impairment. The level of consciousness was graded according to item 1a of the mNIHSS scale: patient alert (item 1a = 0), not alert but arousable (item 1a = 1), not alert but arousable with strong stimulation (item 1a = 2), totally unresponsive (item 1a = 3). Use of the EMS for transport to hospital was recorded. In Italy the EMS is organised on a provincial basis with a single call centre that answers all patients’ phone calls to 118. Day or night onset was defined when symptoms began from 07:00 to 22:59 hours and from 23:00 to 06:59 hours or at awakening, respectively. Working days were the week days from Monday to Friday, non-working days were Saturday, Sunday and national holidays.
Statistical analysis
Arrival delays were not normally distributed, therefore for descriptive statistics the median and interquartile range (IQR) are given. Comparison of delays within the ED in relation to time from onset (<3, between 3 and 6 and >6 h) was made with the Kruskal–Wallis test.
At univariate analysis arrival delay was considered the dependent variable and the variables reported below were tested against it. Nominal variables (gender, history of arterial hypertension, diabetes or atrial fibrillation, previous stroke, previous hospital admission, use of the EMS, onset of stroke during day or night, admission during working or non-working day) were dichotomised (0 = no, 1 = yes); mNIHSS was analyzed as an ordinal variable, as well as a categorical variable (0 < 12, 1 ⩾ 12); level of consciousness was graded in four classes according to item 1a of the mNIHSS. Comparison of arrival delays between two groups was performed using the Mann–Whitney test and between more than two groups with the Kruskal–Wallis test. The Spearman test was used for correlations between arrival delays and age and the mNIHSS score.
Among the above-mentioned variables, those associated with the arrival delay with a p value less than 0.2 were included in the multivariate analysis. Multivariate analysis of the arrival delay was performed by multiple linear regression and for this analysis the arrival delays were transformed into logarithms in order to obtain a normal distribution. The final model was determined by the stepwise method.
In a second model we also considered use of the EMS as the dependent variable (0 = no, 1 = yes). Selection of the independent variables was made with the same criteria as above. For this analysis we used binary logistic regression.
A probability value less than 0.05 was considered statistically significant. All probability values were two-sided. For statistical analysis we used SPSS version 12.
RESULTS
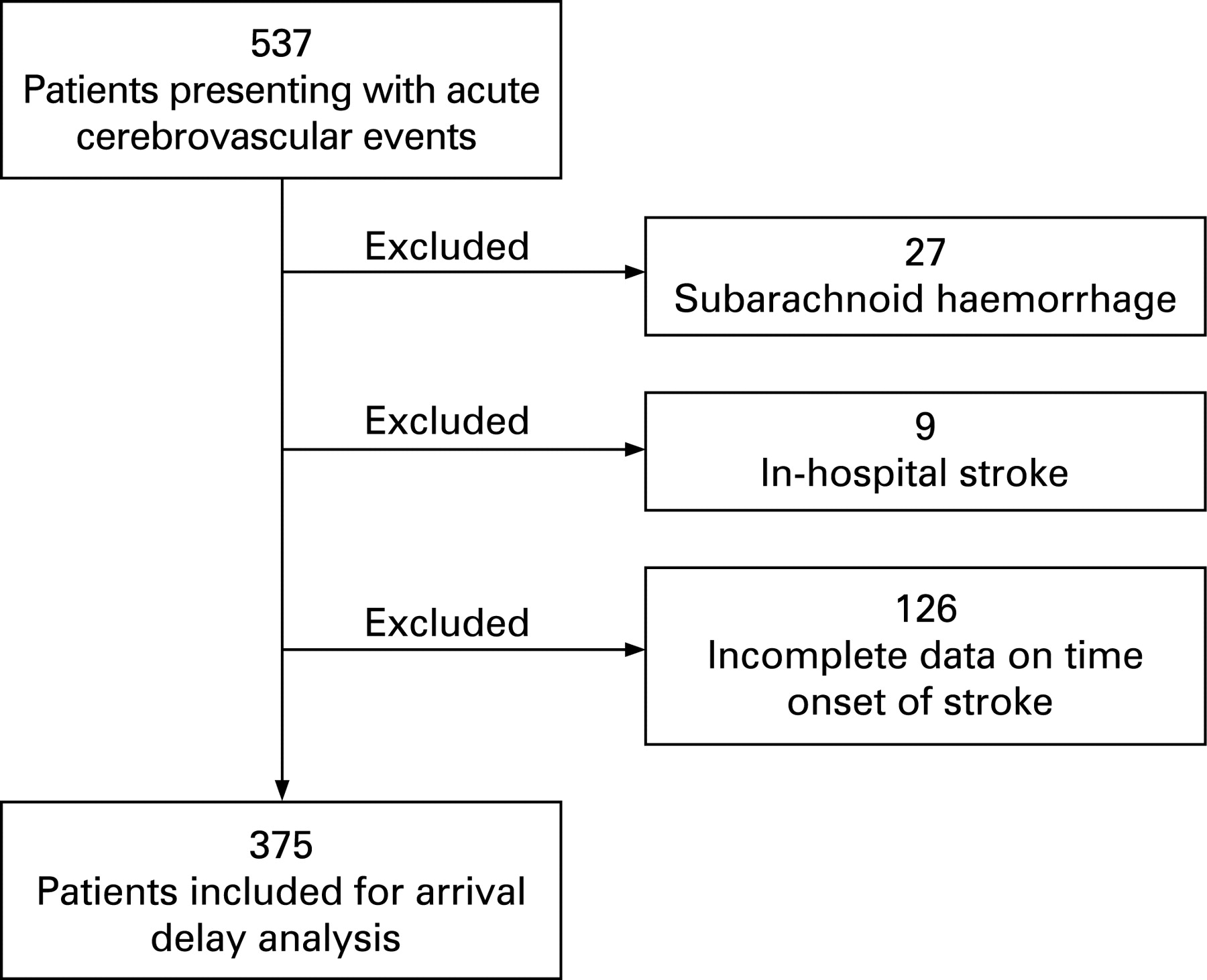
A total of 537 patients presenting with acute cerebrovascular events were evaluated in the ED during a one-year period. Among the whole series, the following patients were excluded: 27 patients with subarachnoid haemorrhage or chronic subdural haematoma; nine with stroke occurring during hospitalisation; 126 with incomplete data regarding time of stroke onset (figure 1). The number of patients included was 375.

{kind=link}
Arrival delay and delays within the ED
The median arrival delay was 5.4 h (IQR 2.7–11.6 h). In 125 (33%) of the patients included the time of stroke onset was obtained precisely and in 250 (66%) it was approximated, as described in the methods section.
The arrival delay and delays within the ED are reported in table 1. The study population was subdivided according to the arrival delay: 104 (28%) patients arrived within 3 h; 198 (53%) within 6 h and 177 (47%) after 6 h and delays within the ED were evaluated according to the time of presentation (table 2). Triage–visit delay and visit–CT delay were significantly shorter for patients presenting within 3 h, whereas there was no difference in visit–report delay in the three groups.
Factors influencing arrival delay
Table 3 reports the general characteristics of the study population and frequencies of factors considered as explanatory variables of arrival delay.
Univariate analysis (table 4) showed that arrival delay was significantly shorter in patients who used the EMS (p<0.001) and with an altered level of consciousness (p = 0.005). Furthermore, arrival delay was negatively associated with the baseline mNIHSS score (p<0.001 at Spearman correlation test). Among 104 patients presenting within 3 h, 69 (66%) used the EMS; whereas among the 177 patients presenting later than 6 h only 85 (48%) used it. Age was not correlated with the arrival delay (p = 0.26 at Spearman test). Gender, history of hypertension and/or diabetes and/or atrial fibrillation, previous hospital admission and previous stroke, type of stroke, onset of stroke during day or night and presentation on working or non-working day had no measurable effect on arrival delay.
Multivariate analysis showed that major contributors to early arrival delay were use of the EMS and high basal mNIHSS score (table 5). Other variables included in the regression model were not significantly associated with arrival delay.
Factors influencing use of the EMS
The study population was dichotomised in patients who used or did not use the EMS (table 6). Univariate analysis showed that use of the EMS was significantly associated with older age, higher basal mNIHSS score and with an altered level of consciousness (p<0.001 for all three). All these three variables remained significantly associated with the use of the EMS in the multivariate analysis.
DISCUSSION
In our study 28% of the patients arrived within 3 h and 53% within 6 h from the onset of symptoms. The proportion of patients presenting to the ED in the time window suitable for thrombolytic therapy is similar to that reported in previous European studies: a French group reported in 2001 that 29% of patients with acute stroke arrived in the stroke unit within 3 h and 75% within 6 h;19 a British multicentre study reported figures of 37% and 50%, respectively,18 similar to those reported in a previous Italian study published in 1997.22 Although comparisons among studies are difficult because of the use of different methods, the proportion of patients presenting in a suitable time for reperfusion therapy seems nearly homogeneous in different European countries.
As regards the delays in evaluation inside the ED, the crucial point in our hospital was the time from arrival to CT scan. In fact, the median visit–CT scan delay was 1.2 h, which is rather longer than the 25 minutes recommended by the American Heart Association6 for patients eligible for recombinant tissue plasminogen activator treatment. As in other hospitals, however, delays for patients with early presentation were shorter. A longer delay was observed to require CT interpretation by the neuroradiologist, but immediate interpretation was required by the ED physician in the case of urgent clinical decisions.
Our study shows that early ED presentation was associated with activation of the EMS and ambulance transportation also after adjusting for the influence of other variables, such as severity of symptoms, age, presence of risk factors, previous stroke or hospital admission, all factors that could increase the awareness of illness by the patients and their relatives. The median arrival delay in our patients presenting with the EMS was approximately 4 h, whereas self-presenting patients showed a median arrival delay of nearly 7 h. These figures are longer than those reported in a previous north American study9 but the difference could be due to different EMS organisation or geographical differences.
Although the percentage of patients who called the EMS (57%) was higher than reported in other series9 19 a relatively small proportion arrived within 3 h (32%) or within 6 h (60%). An increase in these proportions could be beneficial to patients with stroke, increasing the possibility of effective treatment and lowering the risk of developing large infarcts and subsequent disability. Efforts should be made to inform risk populations about the disease, the symptoms of presentation and the need to reach the hospital as soon as possible. This information could easily be given by family doctors or other physicians who treat patients at risk of stroke. It is hoped that in the future all health professional care will sensitise to the early recognition and treatment of stroke patients, as well as to the early presentation to the ED.
In conclusion, a substantial proportion of patients does not arrive at the ED in a suitable time for reperfusion therapy. Patients transported by the EMS have a shorter arrival delay. Approximately half of the patients with stroke are sufficiently aware of the urgency of this clinical condition to activate the emergency telephone system. Effort should be made to inform at-risk populations about the symptoms of presentation and to encourage the use of the EMS.
REFERENCES
Footnotes
Competing interests: None declared.