Article Text

Abstract
Objective: Preclinical actions in the primary assessment of victims of blunt trauma may prolong the time to definitive clinical care. The aim of this study was to examine the duration of performed interventions and to study the effect of on-scene time (OST) and interventions performed before admission to hospital on hospital resuscitation time.
Methods: 147 consecutive patients with high-energy blunt trauma aged ⩾15 years were studied prospectively. Prehospital time intervals and interventions were documented and compared with hospital data collected from continuous digital video registration. Analyses were performed with correction for injury severity and type of prehospital medical assistance (emergency medical services (EMS) versus physician-staffed helicopter emergency medical services (HEMS)).
Results: Primary survey and initial treatment were initiated and completed within 1 h of arrival of the EMS. 83% of this “golden hour” elapsed out of hospital and 81% (n = 224) of all interventions (n = 275) were carried out before admission to hospital. An increase in the number of prehospital interventions was associated with an increased OST (p<0.001). Subanalyses showed no such correlation in the HEMS group. The HEMS group had a longer mean OST than the EMS group (p<0.001) with relatively more prehospital interventions (p<0.001) and a shorter mean in-hospital primary survey time with fewer in-hospital interventions. Overall, OST and the number of prehospital interventions were not related to in-hospital primary survey time and interventions.
Conclusion: For most trauma patients the initial life- and limb-saving care is achieved within the “golden hour”. Prehospital treatment occupies most of the golden hour. More prehospital interventions were performed with HEMS than with EMS only, but the higher number of interventions did not result in a longer OST with HEMS. Although the numbers of subsequent in-hospital interventions may be lower, no reduction in time in hospital may be expected from the interventions performed before hospital admission.
Statistics from Altmetric.com
Efficient time management and adequate acute treatment are considered crucial in the initial care of trauma victims. The period immediately following a trauma during which patients should receive life- and limb-saving care is often referred to as the “golden hour”.1 The chances of survival increase when the time between the actual injury and the definitive care is kept to a minimum.2 3 Thus, trauma care systems are designed to provide rapid coordinated medical care to injured patients.4
In the Netherlands the out-of-hospital trauma care is provided by emergency medical services (EMS). EMS teams are staffed with a highly trained nurse who supplies basic emergency care. In addition to the EMS, physician-staffed helicopter emergency medical services (HEMS) provide advanced trauma life support (ATLS)-based medical care5 and professional overall on-scene management. HEMS are dispatched according to specific criteria. The primary dispatch criteria are based on suspicion of a high-energy trauma or other life-threatening trauma, and secondary dispatch criteria are based on the condition of the patient.6 Because of relatively short distances in the Netherlands, HEMS activation is not related to distance and patient transportation to an appropriate emergency department is predominantly (85–98%) performed by ambulance, escorted by the HEMS physician when indicated.
In the Netherlands the involvement of the HEMS seems to reduce mortality and to enhance survival chances compared with situations were only EMS assistance is provided, especially for patients with severe blunt trauma.7 However, the on-scene presence of a physician and subsequent increase in the number of time-consuming interventions may prolong the prehospital on-scene time (OST).
Primary in-hospital care should continue (H)EMS-initiated treatment following the internationally implemented ATLS guidelines5 and may benefit from the interventions that were already performed on-scene.
Several studies have investigated the effect of the time interval within the “golden hour” on patient outcome.3 7–9 However, to our knowledge, no studies have investigated the actual time frames and actions in this first period following a trauma. In addition, no studies have been published in which the interventions performed on-scene and their duration were correlated with the interventions and the time spent during in-hospital primary trauma care.
The objective of this study was to examine the time management and interventions of the initial (pre)hospital trauma care. In addition, we tested the hypothesis that an increase in the number of interventions performed before admission to hospital would result in a reduction in the time spent in the emergency room.
METHODS
Study design
A prospective cohort study was performed, documenting and evaluating the interventions performed before and after admission to hospital and the time-related structure of initial trauma care in blunt trauma victims. The study setting was a level 1 trauma centre in the Netherlands (Erasmus MC, Rotterdam) and its related trauma care region with over 2.5 million inhabitants.
Selection of participants
From May to September 2003, all consecutive patients sustaining a high-energy blunt force trauma who were transported directly from the scene of the accident to the emergency department were enrolled in the study. Patients referred to the Erasmus MC from another hospital were not considered eligible for inclusion. Victims of penetrating trauma were excluded because of the specific injury characteristics and subsequent requirement for the “scoop and run” procedure. Patients under the age of 15 years and victims of drowning, strangulation or suffocation were also excluded.
Data collection and processing
The data on all trauma patients were prospectively documented into the Major Trauma Outcome Study (MTOS) compatible trauma registry. Prehospital time intervals, the number and types of interventions performed before and after admission to hospital (intubation, chest tube, first and second intravenous line insertion, extremity splint placement) and patient characteristics were recorded. The prehospital time interval was divided into OST and transport time. OST was defined as the time between arrival of the first EMS unit on the scene and departure of the patient from the trauma scene. Transport time was defined as the time interval between departure from the trauma scene and arrival at the emergency department.
Dispatch centre records, ambulance registration forms and HEMS flight forms were manually collected and used to supplement registry data. The prehospital times were recorded in real time during the dispatch. The Revised Trauma Score (RTS) and Glasgow Coma Scale (GCS) were recorded on arrival of the first EMS unit but before treatment was initiated in order to avoid any bias.
The hospital resuscitation time (HRT) was obtained from continuous digital video registration. This allowed for a highly accurate calculation of the HRT that was blinded to prehospital data.10 The interventions performed and the duration of the time intervals were scored using these videos. This enabled scoring of the number of interventions performed during the different steps of the ATLS principles (A, B, C, D and E) and the time needed.
The HRT was defined as the interval between briefing and the end of the secondary survey. It was subdivided into primary and secondary survey. Primary survey is the interval from briefing until the end of the exposure interval. Secondary survey is the time from the end of the exposure interval until the end of a complete and detailed physical examination including radiographs. In cases where the ATLS principle was not executed to completion, the end point of both the the primary survey and HRT was defined as either the last finished ATLS interval “ABCDE”, departure from the resuscitation room or death.
Two subanalyses were performed. To assess the effect of injury severity, patients with an injury severity score (ISS) <16 were compared with those with an ISS ⩾16.11 In addition, data for patients receiving additional HEMS assistance were compared with data for the EMS group.
Outcome measures
Primary outcome measures were prehospital and in-hospital time intervals. Secondary outcome measures were the number and types of interventions performed before and after admission to hospital.
Data analyses
All analyses were performed using the SPSS Version 11.5. Data on time management are displayed as median time with first and third quartiles. Comparisons between groups were made using the χ2 test for categorical variables and the Mann-Whitney U test for continuous variables. Data were stratified according to ISS (<16 vs ⩾16) and the presence of HEMS (EMS group vs combined EMS-HEMS group) to determine any additional effect of injury severity and HEMS assistance on time management and interventions performed. Linear regression analysis was performed to determine the correlation between prehospital and hospital interventions and the total trauma resuscitation time.
RESULTS
Characteristics of study subjects
During the 4-month study period 192 patients with suspected blunt high-energy trauma were admitted to the emergency department of a level 1 trauma centre. Forty-five of these 192 patients were excluded from the study: 29 were aged <15 years, 4 were referred from surrounding hospitals, 3 sustained penetrating trauma and prehospital data could not be retrieved for 9 patients. Data for the remaining 147 patients were analysed. Of these, 45 were multi-trauma patients with an ISS of ⩾16 and 102 had an ISS of <16. A total of 40 patients were assisted by combined EMS-HEMS. When patients were treated by both an EMS and an HEMS unit, the EMS team always arrived on the scene first.
The demographic characteristics of the patients are shown in table 1. HEMS assistance was provided relatively more frequently in the multi-trauma group (21/43). Patients in the EMS-HEMS group were more severely injured, as represented by lower GCS and RTS values and higher ISS values. In addition, patients in this group experienced physical entrapment relatively more often than patients in the EMS group. Unadjusted mortality was higher for multi-trauma patients and for patients receiving additional HEMS assistance.
Main results
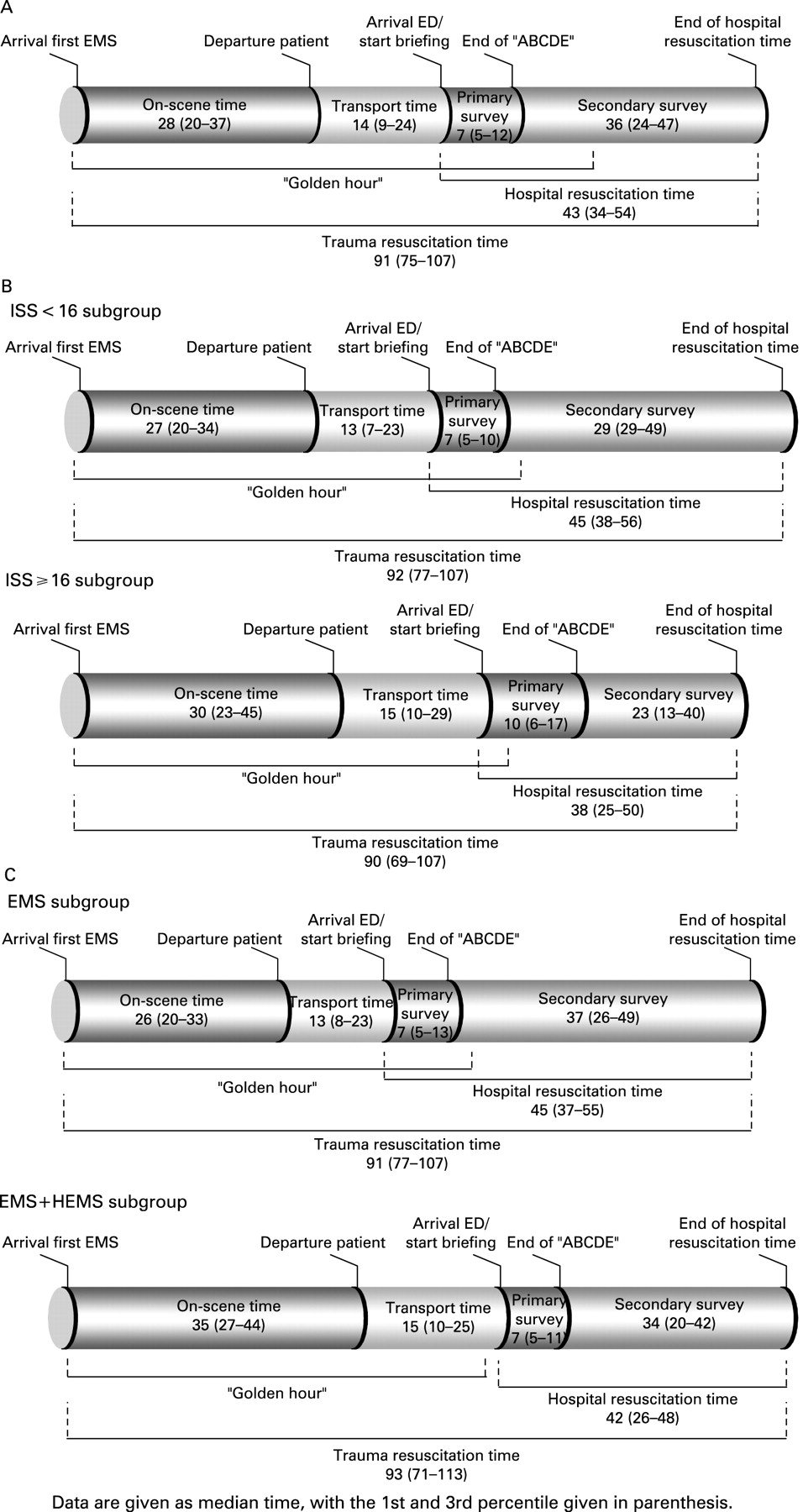
The distribution of the various time intervals is shown in fig 1A. The median trauma resuscitation time (TRT) was 91 min, subdivided into a median OST of 28 min, transport time of 14 min, primary survey time of 7 min and secondary survey time of 36 min. On average and within all subgroups, the initial assessment and treatment including the primary survey were completed within the first hour after arrival of the first EMS unit at the trauma scene. When stratified according to injury severity (fig 1B), the multi-trauma group had no difference in prehospital time intervals but did have a longer in-hospital primary survey interval (p = 0.001) and a shorter in-hospital secondary survey interval (p<0.001). The HEMS-assisted group (fig 1C) had a longer mean OST (p<0.001) and a shorter mean in-hospital primary survey time than the group treated by EMS only.
{kind=link}
The prehospital and in-hospital interventions performed during the “golden hour” are shown in table 2. A total of 275 interventions were performed in the 147 patients included in the study. Of these, 81.5% were performed before admission to hospital and 18.5% were performed in the emergency department. Most of the prehospital interventions were intravenous line insertions and most of the in-hospital interventions consisted of insertion of a second intravenous line and extremity splint immobilisation. The numbers of prehospital and in-hospital interventions were higher in the multi-trauma patients (ISS ⩾16) than in the group with an ISS <16. The number of prehospital interventions was higher in the HEMS-EMS group than in the EMS group (p<0.001) and the number of in-hospital interventions was lower. Relatively more prehospital intubations, chest tube placements and second intravenous line insertions were performed in the HEMS group.
The five prehospital interventions (intubation, tube thoracotomy, first and second intravenous line insertions and extremity splint placement) were analysed in relation to the OST. There was a significant association between prehospital intubation (p = 0.05), chest tube placement (p = 0.005) and second intravenous line insertion (p = 0.001) and an increase in OST.
Table 3 shows the relation between the number of prehospital interventions (range 0–4) and the prehospital and in-hospital time intervals. An increased number of prehospital interventions was associated with an increased OST (p<0.001). Subanalyses for the EMS and HEMS groups showed no such association for the HEMS group.
No relation was found between the number of prehospital interventions and the duration of the in-hospital primary survey. An increase in transport time was correlated with an increased number of on-scene interventions. Each single prehospital intervention and the duration of the corresponding hospital ATLS interval was given in seconds (table 4). In-hospital time intervals were fairly constant despite performance of on-scene interventions.
DISCUSSION
This study has objectively assessed the time intervals and interventions performed in the initial care of 147 patients with blunt trauma. The effect of prehospital interventions and subsequent time spent at the trauma scene on resuscitation time in the emergency department has been studied for the first time. The median time interval from the arrival of an EMS unit at the trauma scene until the end of the primary survey was 49 min, delivering life- and limb-saving treatment within the first hour after arrival of medical assistance. This finding is in line with the worldwide assumption that definitive care must be established preferably within the “golden hour” to improve patient outcome.5
As expected, the number of prehospital interventions was associated with an increase in the OST in both EMS- and HEMS-assisted patients. However, the concept that an increased OST should result in a decrease in hospital primary survey time was not supported. The results indicated a short primary survey time in the emergency department which was fairly constant and not affected by interventions performed before admission to hospital. A more detailed analysis dividing the hospital primary survey into time frames for the single ATLS intervals (ABCDE) showed exact time intervals with far greater accuracy than the existing literature. Although some differences were statistically significant, the clinical relevance is limited.
An explanation for both findings concerning the primary survey time could be a more efficient, systematic and simultaneous ATLS approach of the emergency department trauma team. This might minimise the time required for ABCDE, even when more interventions are needed. The number of prehospital interventions prolonged the OST, but no such association was found when HEMS had been involved. On average, the presence of the HEMS crew was related to an increased OST (fig 1C). This may be due to the relatively higher number of time-consuming physical entrapments in the HEMS-assisted group, the reassessment time by the HEMS team and an overall more extensive treatment in addition to the five interventions documented in this study. The higher number of more severely injured patients in the HEMS group requiring more interventions did not increase the prehospital time intervals.
In agreement with the findings of the present study, both van Olden et al8 and a meta-analysis by Carr et al12 of 49 studies on prehospital times in 20 states in the USA showed an average prolonged OST when HEMS had been involved. Furthermore, a study by Sampalis et al13 and a meta-analysis by Liberman et al14 showed that prehospital advanced life support resulted in increased OST. However, no study or meta-analysis has investigated blunt trauma victims separately.
As reported by Hedges et al,15 the present study showed a relation between longer patient transport times and number of interventions, suggesting that longer distances to the hospital result in more interventions being performed on scene. This infers that (para)medics tailor their on-scene intervention strategy to transport distance. The finding by Petri et al16 of a shorter OST in severely injured patients suggests that this may be another factor guiding the actions of (para)medics during on-scene management.
Limitations of study
No precise definition of the “golden hour” was found in the literature, suggesting that it is a concept rather than a stringent period of time. The measurement starting point chosen for this study was the arrival of the first EMS unit. This was chosen primarily because this point could be determined objectively and also because, from this time point, the prehospital medical interventions are supposed to affect the in-hospital resuscitation times and interventions. For logistical reasons the actual time at which the trauma occurred could not be retrieved reliably in about 30% of cases. For cases in which the trauma time and the EMS response time were documented accurately, a median time interval of 6 min passed between the emergency call to the dispatch centre and the arrival of the first EMS at the accident scene. The prehospital time intervals recorded in this study would thus increase overall by 6 min. Still, the “golden hour” would have expired after the initial treatment including the primary survey at the emergency department.
Because of the aforementioned unreliable documentation and the focus of the investigations on the influence of OST and prehospital interventions on the HRT rather than on the clinical outcome, the currently used starting point seems justified.
If emergency surgery was needed or when a patient died, not all ATLS steps were completed. A moderate effect of this early termination on the HRT in the group of severely injured patients cannot be ruled out.
Likewise, these patients were more likely to need more (radio)diagnostic modalities resulting in a longer HRT. This could result in bias towards in-hospital times in sicker patients, although the number of cases with unfinished ATLS steps was limited (n = 17).
This study did not report on clinical outcome. The only objective outcome parameter obtained was 30-day mortality. Since the number of deaths was low owing to the heterogeneity of the injuries, this parameter could not be used for further analyses or for interpretation of the results.
CONCLUSION
(H)EMS achieve life- and limb-saving care within the “golden hour” but this occupies 83% of the first hour after a traumatic injury. A number of factors appear to affect the decisions concerning the medical treatment and subsequent time spent on the initial treatment. Clearly, the time necessary for treatment is predominantly determined by the number of interventions that need to be performed before admission to hospital, combined with the level of prehospital care. The number of prehospital interventions is increased when HEMS are involved compared with EMS only, but the higher number of interventions does not result in longer OST in the HEMS group. However, although the numbers of subsequent interventions performed in hospital may be lower, performance of interventions before admission to hospital does not seem to result in a reduction in the time in hospital.
This study of the time frames in initial trauma care might serve as a basis for further research into the consequences of interventions and time management on patient outcome.
REFERENCES
Footnotes
Funding: None.
Competing interests: None.