Article Text

Abstract
Objectives: To determine the efficacy of the abbreviated Mortality in Emergency Department Sepsis (MEDS) score, the Modified Early Warning (MEW) score and near-patient-test (NPT) lactate levels in predicting 28-day mortality in adult emergency department (ED) patients with sepsis.
Methods: A retrospective cohort study of adult ED patients with sepsis admitted to hospital was conducted in a large urban teaching and a district general hospital. Data were collected during four time periods between 1 January 2006 and 31 January 2007. Inclusion criteria were age ⩾16 years and an ED diagnosis of sepsis. Primary outcome for all patients was 28-day mortality. Patients were preassigned to risk groups according to their abbreviated MEDS score, MEW score and NPT lactate.
Results: 307 ED patients with sepsis were included in the study. Among these there were 72 deaths (23%). Mortality rates for the low-, moderate- and high-risk groups of the abbreviated MEDS score were 1/63 (1.6%), 48/205 (23.4%) and 23/39 (59.0%) patients. The MEDS score for low-risk patients was 98.6% (95% CI 92.5% to 99.9%) sensitive and 26.5% (95% CI 21.0% to 32.6%) specific and for high-risk patients it was 31.9% (95% CI 21.4% to 44.0%) sensitive and 93.2% (95% CI 89.2% to 96.1%) specific for death within 28 days. Mortality rates for the low- and high-risk MEW score were 20/159 (12.6%) and 52/148 (35.1%) patients. The MEW score for high-risk patients was 72.2% (95% CI 60.4% to 82.1%) sensitive and 59.2% (95% CI 52.6% to 65.5%) specific for mortality. An NPT lactate level of ⩾4 mmol/l was 49.1% (95% CI 35.1% to 63.2%) sensitive and 74.3% (95% CI 64.8% to 82.3%) specific for 28-day mortality.
Conclusion: These results demonstrate the efficacy of the abbreviated MEDS score, the MEW score and NPT venous lactate levels in predicting 28-day mortality in ED patients with sepsis. The abbreviated MEDS score was found to be the best performing risk assessment model which, with prospective validation, may aid early clinical decision-making in ED patients with sepsis and might affect the outcome from sepsis.
Statistics from Altmetric.com
Sepsis remains an ongoing challenge in medicine. It is one of the major causes of morbidity and mortality worldwide. Mortality rates in severe sepsis are as high as 28.7–49.7%, equalling the number of deaths caused by acute myocardial infarction.1–4 Advances in medicine had little effect on the outcome of sepsis until “early goal-directed therapy” (EGDT) demonstrated a significant reduction in mortality.4 EGDT is central to the international Surviving Sepsis Campaign Guidelines,5 emphasising the importance of early recognition and haemodynamic optimisation of the patient with sepsis.6
Emergency departments (EDs) are the first point of medical contact for critically ill patients and play an important role in early identification of high-risk septic patients. Recognising those patients at an early stage can be a challenge even for the experienced ED clinician, for it may not be as straightforward as one would expect.
Over the last two decades a number of risk-stratifying physiological scoring systems and biochemical markers have been established. The majority of these were derived from patients in the intensive care unit (ICU) and their applicability to patients in the ED remains questionable.
Methods of risk-stratifying patients in the ED include the Modified Early Warning (MEW) score, the Mortality in Emergency Department Sepsis (MEDS) score7 and serum lactate levels.
The MEW score, a scoring system based solely on physiological parameters, is widely used in the UK. Two recent studies in surgical and medical inpatients found the MEW score to be useful in identifying patients at risk of deterioration.8 9 These findings were not supported by a study in patients in an ED.10
The MEDS score, designed to predict mortality in ED patients with sepsis, was derived and validated in patients from a single urban teaching hospital in the USA.7 The score has also been externally validated in non-surgical ICU patients with severe sepsis admitted via an ED in Taiwan11 and in ED patients with sepsis in the USA.12 However, an external validation of the MEDS score in unselected ED patients with sepsis in the UK has not been performed. A drawback for its implementation in UK practice could be the fact that one of the MEDS score variables—neutrophil bands >5%—is not routinely measured in many UK hospitals. However, excluding a single variable from a complex score may only have a small effect on the predictive accuracy.13
Lactate is one of a number of biochemical markers that have been proposed to aid risk stratification in patients with sepsis. A raised blood lactate level has been shown to be predictive of an adverse outcome in critically ill patients and to be associated with an increased mortality in patients with a suspected infection.14 15 Hyperlactataemia in septic patients is one of the criteria for commencing EGDT.4 6 16 For lactate levels to aid early identification of high-risk septic patients, a short turnaround time is important. This can easily be accomplished using a near-patient-test (NPT) device during the initial assessment in the ED.17 To our knowledge, the diagnostic performance of NPT lactate in predicting mortality in ED patients with sepsis has not been assessed.
This study aimed to determine the efficacy of the abbreviated MEDS score (without neutrophil bands), the MEW score and NPT lactate in predicting 28-day mortality in adult ED patients with sepsis.
METHODS
Design and study population
A retrospective cohort study of adult ED patients (>16 years) with sepsis admitted to hospital was performed in the EDs of the Leicester Royal Infirmary (LRI), a large urban teaching hospital, and the Kettering General Hospital (KGH), a district general hospital. Data were collected over four time periods between 1 January 2006 and 31 January 2007. Owing to differences in the availability of the computerised data in the two participating hospitals, two methods of identifying suitable ED patients were used. At the LRI, patients were identified from the computerised ED database (EDIS). They were included if they had an ED diagnosis of sepsis, two or more systemic inflammatory response syndrome (SIRS) criteria and a working diagnosis of infection documented in their ED notes. Patients at the KGH were included if they had blood cultures taken in the ED, had two or more SIRS criteria and a working diagnosis of infection documented in their ED notes. Patients were excluded if parameters to calculate the MEW or MEDS score were missing. The primary outcome was 28-day mortality.
We consulted a COREC information officer and the Kettering R&D Department who advised that formal ethics committee approval was not required for this study owing to its observational nature.
Data collection
Members of the research team, blinded to the primary outcome, collected physiological variables, blood results and information about the patient required to calculate the MEW and abbreviated MEDS score from the ED notes and the laboratory records of all included patients. All of these parameters are routinely obtained as part of standard practice in both participating EDs. Where available, NPT lactate results (Roche OMNI S) were collected from the patient’s ED notes.
Definition of MEDS score variables and risk groups
The original MEDS score comprises nine independent predictors of mortality resulting in a maximum score of 27. For this study, an abbreviated MEDS score without neutrophil bands was used as this reflects common UK practice (table 1). Five previously validated risk groups describe the risk of death according to the MEDS score as very low (0–4), low (5–7), moderate (8–12), high (12–15) and very high (>15).7 We used three risk groups in our study—low, moderate and high—as this is more in keeping with clinical decision-making.
Definition of MEW score variables and risk groups
The MEW score contains five physiological parameters: heart rate, respiratory rate, systolic blood pressure, temperature and level of consciousness. Each parameter is given points of 0–3 (maximum of 2 for temperature) according to their deviation from the normal range. A score of ⩾5 was found to be associated with admission to the intensive care/high dependency unit and an increased mortality.9
Outcome evaluation and statistical analysis
Enrolled patients were preassigned to risk groups according to their MEW score, abbreviated MEDS score and NPT lactate level, based on previously published thresholds.7 9 15 For the abbreviated MEDS score, patients were stratified into low (0–4), moderate (5–12) and high (>12) risk. For the MEW score, patients were classified as low risk (<5) or high risk (⩾5). For lactate, patients were stratified into low (<4 mmol/l) and high risk (⩾4 mmol/l).
Separate and combined analysis of the data retrieved from both hospitals was performed. Descriptive variables were presented as means and 95% confidence intervals (CI). The t test for independent samples was used to compare continuous variables (assuming normal distribution) and the χ2 test for categorical data. Sensitivity, specificity and odds ratios (ORs) were calculated. Kaplan-Meier survival analysis was performed. Receiver operating characteristics (ROC) area under the curve (AUC) was calculated for each predictor model. ROC curves plot the true positive rate (sensitivity) of a test (model) against its false positive rate (1−specificity). The AUC is a measure of the accuracy of the prediction model. All analyses were performed using MedCalc. Statistical significance level was set at p<0.05.
RESULTS
A total of 308 ED patients with sepsis were eligible for inclusion, of which 307 had complete records and were included in the study (fig 1). Among these were 72 deaths (23%). The mean age of the cohort studied was 69.7 years (95% CI 67.5 to 71.8), of which 158 (51%) were men. The abbreviated MEDS score could be calculated for all included patients and the MEW score for all but one patient. Blood lactate was only routinely measured in the ED at the LRI and was available in 90% of cases (n = 158).

Flow diagram of patients included in the study.
Patients enrolled at the LRI were generally older, had a significantly higher mortality rate and far higher mean MEW and mean abbreviated MEDS scores (table 2). Non-survivors were significantly older than survivors and had a significantly higher mean abbreviated MEDS score, mean MEW score and mean blood lactate level (table 3).
The 28-day mortality rates for the low-, moderate- and high-risk groups of the abbreviated MEDS score were 1/63 (1.6%), 48/205 (23.4%) and 23/39 (59.0%) patients. The Kaplan-Meier survival curves illustrate the significant differences between the three risk groups (fig 2). An abbreviated MEDS score of ⩾5 was 98.6% (95% CI 92.5% to 99.9%) sensitive and 26.5% (95% CI 21.0% to 32.6%) specific and a score of >12 was 31.9% (95% CI 21.4% to 44.0%) sensitive and 93.2% (95% CI 89.2% to 96.1%) specific for death within 28 days. Patients with an abbreviated MEDS score of >12 were significantly more likely to die within 28 days (OR 6.4; 95% CI 3.2 to13.1).

Kaplan-Meier survival estimates for low-risk (0–4), moderate-risk (5–12) and high-risk (>12) groups according to the abbreviated Mortality in Emergency Department Sepsis (MEDS) score (log rank test χ2 = 49.4; p<0.001).
Patients with a MEW score ⩾5 had a significantly higher 28-day mortality rate (35.1% (95% CI 27.5% to 43.4%) vs 12.6% (95% CI 7.9% to 18.8%), p<0.001). A MEW score of ⩾5 was 72.2% (95% CI 60.4% to 82.1%) sensitive and 59.2% (95% CI 52.6% to 65.5%) specific for mortality and a significant predictor for non-survival (OR 3.76; 95% CI 2.11 to 6.71).
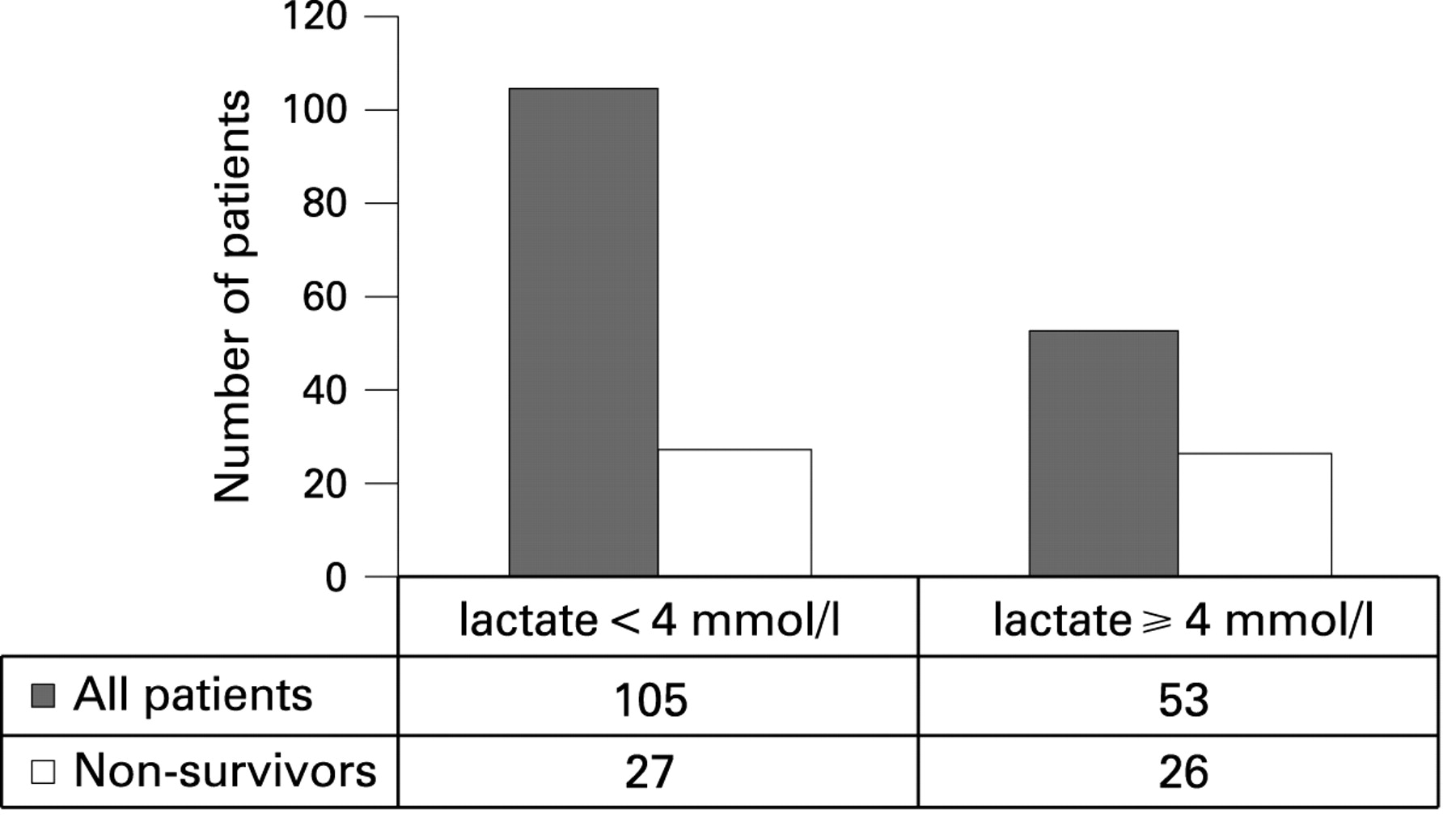
Patients with a lactate level of ⩾4 mmol/l had a significantly higher mortality rate (49.1% vs 25.7%; p = 0.006) (fig 3) and were more likely to die (OR 2.8; 95% CI 1.39 to 5.57). A blood lactate level of ⩾4 mmol/l was 49.1% (95% CI 35.1% to 63.2%) sensitive and 74.3% (95% CI 64.8% to 82.3%) specific for 28-day mortality.

Association between lactate level and 28-day mortality in emergency department patients with sepsis.
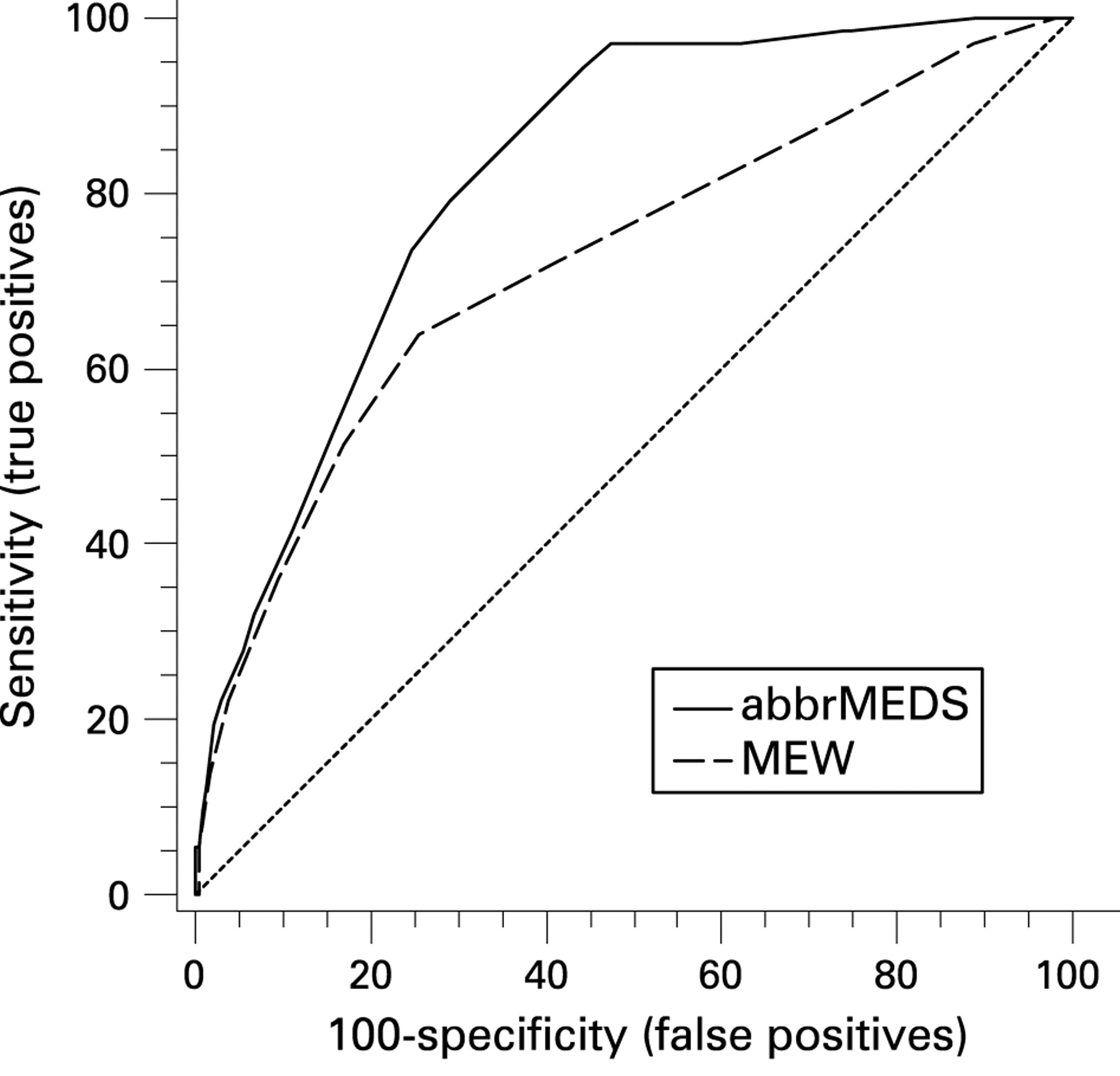
ROC analysis including data on all patients showed the abbreviated MEDS score to be a good predictor of 28-day mortality, the MEW score to be an acceptable predictor and NPT lactate levels to be a poor predictor of 28-day mortality (table 4). The abbreviated MEDS score was found to be a significantly better discriminator than the MEW score (p = 0.016, fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operator characteristic (ROC) curves: comparison of abbreviated Mortality in Emergency Department Sepsis (abbrMEDS) score and Modified Early Warning (MEW) score as predictor of 28-day mortality.
DISCUSSION
Our results demonstrate the efficacy of the abbreviated MEDS score, the MEW score and NPT venous lactate levels in predicting 28-day mortality in ED patients with sepsis. Although all three assessment models demonstrated the potential of an early risk-stratifying tool for patients with sepsis, the abbreviated MEDS score was found to be the best overall discriminator for identifying high-risk patients.
MEDS score
This is the first evaluation of the MEDS score in patients with sepsis in UK emergency care. We used an abbreviated version of the score (without neutrophil bands), reflecting common practice in UK EDs. We found that the performance of the abbreviated MEDS score is comparable to the original MEDS score (AUC 0.82)7 and an external validation among ICU patients with sepsis in Taiwan (AUC 0.75).11
As for any scoring systems, its utility in clinical practice will depend on the ease with which the score can be applied. Parameters for the abbreviated MEDS score are readily available as part of the standard clinical assessment and baseline blood tests that are obtained in all unwell patients in the ED. As well as identifying high-risk patients in need of EGDT, the abbreviated MEDS score may also have the potential to be used as a “rule-out” tool since patients with an abbreviated MEDS score of ⩽5 have a very low mortality of 1.6% (sensitivity 98.6%). Conversely, the abbreviated MEDS score may also have the potential to be used as a tool to identify a group of patients where aggressive therapy is futile, since an abbreviated MEDS score of >16 in our cohort had a 98.7% specificity for 28-day mortality.
The abbreviated MEDS score performed well in both cohorts of patients, despite the fact that patients in the LRI were older and had a significantly higher mortality rate than the KGH cohort. Furthermore, applying the abbreviated MEDS score to the derivation and validation data sets (combined) of Shapiro7 resulted in an AUC of 0.80 compared with an AUC of 0.808 with the original MEDS score (Dr N Shapiro, personal communication). Such a difference is unlikely to be clinically significant.
MEW score
The MEW score was originally developed to allow early identification of critically ill patients on general wards; it was not specifically designed to identify the presence of sepsis. When applying the score to our cohorts of ED patients with sepsis, its overall performance in predicting 28-day mortality was acceptable. However, its discriminatory power among the older and more sick LRI cohort of patients was rather poor (AUC 0.63). Using a cut-off MEW score of ⩾5 to stratify patients into low and high risk, as previously suggested,9 was not found to be effective in our patients. Taking everything into consideration, we found the MEW score to be a less suitable risk assessment tool for ED patients with sepsis.
NPT lactate levels
This study investigated the prognostic usefulness of NPT lactate levels in ED patients with sepsis and demonstrated an association of raised lactate and mortality in patients with sepsis. Not only had non-survivors a significantly higher NPT lactate level than survivors, patients in the high-risk lactate group (⩾4 mmol/l) had a significantly higher mortality rate (p = 0.006). These findings are compatible with results from previous studies using conventional laboratory lactate analysis,6 14 15 18 19 and would make NPT lactate a useful tool in early risk assessment of patients with sepsis. Despite this, we found that NPT lactate was less discriminative in predicting mortality in ED patients with sepsis than the other two risk models. It may be that there are patients with a normal lactate level who die by mechanisms other than tissue hypoxia (eg, multiple organ failure), or that raised lactate levels in survivors might be the result of metabolic processes other than anaerobic glycolysis.20
Study limitations
As with any retrospective study, the data included and their accuracy are dependent on the original ED note-keeping, thus creating a potential for bias. There is the possibility that patients with sepsis were missed during the study period if they were given the wrong ED discharge code or did not have blood cultures obtained in the ED. We chose 28-day mortality as the primary end point for assessing predictability of each risk model, but deaths unrelated to sepsis may have occurred. However, when assessing the prognostic ability of each risk model for early death (⩽3 days), their performances were consistent (abbreviated MEDS score: AUC 0.80; MEW score: AUC 0.69; lactate: AUC 0.63). Lactate was only available for half the patients (those with a coded ED diagnosis of sepsis) and may thus not be generalisable to all ED patients with a clinically suspected infection. Finally, the patient selection criteria in this study were broadly defined, creating a rather heterogeneous cohort. Although this was not intentional, it is reflective of real-life clinical practice and may be more in keeping with the way risk assessment tools should be used.
CONCLUSION
The data from our study suggest that the abbreviated MEDS score, MEW score and NPT lactate levels provide considerable prognostic information about 28-day mortality in ED patients with sepsis. The abbreviated MEDS score was found to be the best performing risk assessment model, a promising tool for early identification of high-risk patients with sepsis in the ED. With prospective validation, the abbreviated MEDS score may aid early clinical decision-making in ED patients with sepsis, which may substantially improve the outcome from sepsis.
We consulted a COREC information officer and the Kettering R&D Department who advised that formal ethics committee approval was not required for this study owing to its observational nature.
Acknowledgments
The authors thank Jenny Tiisler, Mike Silverstone and Vivek Pillai for their assistance in this study.
REFERENCES
Footnotes
Funding: None.
Competing interests: None.
Linked Articles
- Primary survey