Article Text

Abstract
Background Hypothermia at hospital admission has been found to independently predict increased mortality in trauma patients.
Objectives To establish if patients anaesthetised in the prehospital phase of care had a higher rate of hypothermia than non-anaesthetised patients on admission to hospital.
Methods Retrospective review of admission body temperature in 1292 consecutive prehospital trauma patients attended by a physician-led prehospital trauma service admitted to The Royal London Hospital between 1 July 2005 and 31 December 2008.
Results 38% had a temperature recorded on admission. There was a significant difference in body temperature between the anaesthetised group (N=207) and the non-anaesthetised group (N=287): mean (SD) 35.0 (2.1) vs 36.2 (1.0)°C, respectively (p<0.001). No significant seasonal body temperature variation was demonstrated.
Conclusion This study confirmed that patients anaesthetised in the prehospital phase of care had a significantly lower admission body temperature. This has led to a change in the author's prehospital practice. Anaesthetised patients are now actively surface heated and have whole body insulation to prevent further heat loss in an attempt to conserve body temperature and improve outcome. This is an example of best in-hospital anaesthetic practice being carried out in the prehospital phase.
- Hypothermia
- emergency medical services
- body temperature
- injury
- anaesthesia
- clinical assessment
- effectiveness
- environmental medicine
- prehospital care
- trauma
- major trauma management
Statistics from Altmetric.com
- Hypothermia
- emergency medical services
- body temperature
- injury
- anaesthesia
- clinical assessment
- effectiveness
- environmental medicine
- prehospital care
- trauma
- major trauma management
Introduction
Hypothermia is an independent predictor of increased morbidity and mortality in severely injured patients, regardless of injury severity, the presence of shock, and other coexisting factors.1–10 Hypothermia has been defined as a core body temperature <36°C,11–15 both in trauma patients and those undergoing anaesthesia. Induction of general anaesthesia prevents normal homoeostatic control of body temperature and typically results in a 1°C fall in core temperature within 30 min.16 Certain conditions predispose to hypothermia. Those at the extremes of age, receiving certain drugs, or with neurological injury or burns are at particular risk.
Active rewarming using a resistive (electric) heating blanket has been found to increase body temperature in an experimental model of accidental hypothermia17 and during transport18 and to effectively prevent intraoperative heat loss during major abdominal surgery.19 It is therefore a potentially useful technique in the prehospital setting. The application of a systematic prehospital hypothermia prevention strategy has been shown to arrest post-injury hypothermia in rural areas with prolonged evacuation times.20 We suspected that patients with trauma who had prehospital anaesthesia would be at high risk of hypothermia. We were unable to identify any published data on temperature homoeostasis for anaesthetised trauma patients in an urban helicopter emergency medical service (HEMS) setting. Having identified readily available warming techniques, which could be applied in the prehospital phase, we performed an observational study to identify the incidence of hypothermia in our patients. Prevention of hypothermia is a key feature of good in-hospital anaesthetic practice, and recent UK guidelines have stressed that prehospital anaesthesia should, where possible, be carried out to the same standards as in-hospital anaesthesia.21
Aim of study
We set out to determine the incidence of hypothermia in prehospital trauma patients and whether the problem was more common in anaesthetised patients. We identified two groups of trauma patients, those who were anaesthetised before transport and those who were not.
Study setting
The study setting was London HEMS which is a physician-led prehospital care service tasked to major trauma in a mainly urban environment. Just over a third of patients attended by the service require prehospital anaesthesia.
Methods
The project was registered as a clinical service evaluation of patients aged 16 and above. Admission body temperature (Genius infrared tympanic thermometer; Tyco Healthcare, Mansfield, Massachusetts, USA) was obtained from the hospital trauma service registry, and the prehospital clinical details and interventions from the prehospital medical records. The relevant parts of the two datasets were merged, and quality assurance checks performed. Unique hospital numbers, personal data and dates were used to ensure that each individual's records were accurately matched across data sources. The tympanic thermometers were calibrated every 3 months.
Admission body temperature has been recorded in our emergency department since July 2005. The study period was started in the second half of 2005 and ended in 2008. A total of 1292 patients met inclusion criteria in this period.
A standard anaesthetic technique is performed on prehospital trauma patients. Etomidate (0.3 mg/kg if normotensive, 0.2 mg/kg if hypotensive) (B Braun, Melsungen AG, Germany) is used as an induction agent, and suxamethonium (Anectine; GSK, Uxbridge, UK) followed by pancuronium (Hospital UK Ltd, Warwickshire, UK) 0.1 mg/kg are administered for muscle relaxation. Post-induction analgesia and sedation are provided with titrated intravenous morphine and midazolam (Hameln Pharmaceuticals, Gloucester, UK) in 1–2 mg aliquots. Indications for a rapid sequence induction (RSI) are actual or impending airway compromise, ventilatory failure, unconsciousness, humanitarian reasons, and in patients who are unmanageable or severely agitated after head injury. Our service is dispatched specifically to major trauma within a catchment area of 2826 km2, with a resident or commuting population of approximately 10 million. A doctor and paramedic team are dispatched by helicopter during daylight hours and by rapid response car at other times.
As part of London HEMS Standard Operating Procedures (SOP), patients with serious injuries are packaged after removal of clothing and placed, skin to metal, on an aluminium orthopaedic scoop stretcher (model 265; Ferno, Cleckheaton, UK). Patients are then covered with a standard cotton or fire-retardant polyester ambulance blanket (Thomas Kneale Co Ltd, Manchester, UK) and moved as soon as possible to an ambulance or helicopter for transport to hospital. Patients attended outside buildings are therefore directly exposed to ambient temperature; in London, the mean (SD) minimum temperature is 2.2 (1.9)°C in January and February.22
We recorded the following variables: age, gender, severity of injury, the presence of central nervous system (CNS) injury and burns, on-scene time, mortality, admission temperature, and variation of admission body temperature with time of year. Hypothermia was defined as body temperature below 36°C as currently recommended for trauma and anaesthetised patients.11–13 16 Grading of specific injuries was determined by the 1990 Abbreviated Injury Scale (AIS). Patients were designated as having a head injury only if the AIS score for ‘head’ was 3 or more and the remaining body area scores were 1, consistent with previous work.2 Burn injuries were considered severe if AIS for ‘external’ was equal to or above 3. ‘Elderly’ was defined as aged 60 years and above.
Statistical analysis was performed using SPSS V16.0. Assuming normal distribution, Student unpaired t test or one-way analysis of variance, as appropriate, was used for comparison of numerical data, and χ2 test for evaluation of proportions between groups. Statistical significance was defined as p<0.05.
Results
Of the 1292 patients admitted, 497 (38.5%) had a prehospital RSI. Temperature was recorded on admission for 494 patients (38%), 47% of which had hypothermia on arrival in the emergency department, with the mean (SD) temperature being 34.6 (1.7)°C. There was a trend for more frequent temperature acquisition in the RSI group than in the non-RSI group (207/497 (41.6%) vs 287/795 (36.1%), p=0.053) (table 1).
Patients admitted to the emergency department at Royal London Hospital by London Helicopter Emergency Service from July 2005 up to and including 2008
The two comparison groups were not matched for age, proportion of elderly people, and on-scene time as described in table 1. No significant difference in gender was found, male (%) being 80.7 (RSI) vs 84.7 (non-RSI) (p=0.3).
For patients with a temperature recorded, a higher percentage of patients with CNS injury (AIS for head ≥3) was found for the RSI group than for the non-RSI group (13 vs 4, respectively, p<0.001) (Table 1). Of the seven patients with severe burn injuries, temperature was recorded for only three on arrival in the emergency department: two in the non-RSI group (36.1°C (75% burns) and 36.9°C (25% burns)—both later transferred to the burns unit) and one RSI patient with 80% burns had a temperature of 33.3°C (died) (not tabulated).
The percentage of patients with ISS >15 was higher for the RSI group than for the non-RSI group (62 vs 29, respectively, p<0.001). Likewise, the mean (SD) ISS was higher for the RSI group than for the non-RSI group (21 (14) vs 12 (10), respectively, p<0.001).
A significantly higher mortality was found for the RSI group than for the non-RSI group (17% vs 2%, respectively, p<0.001).
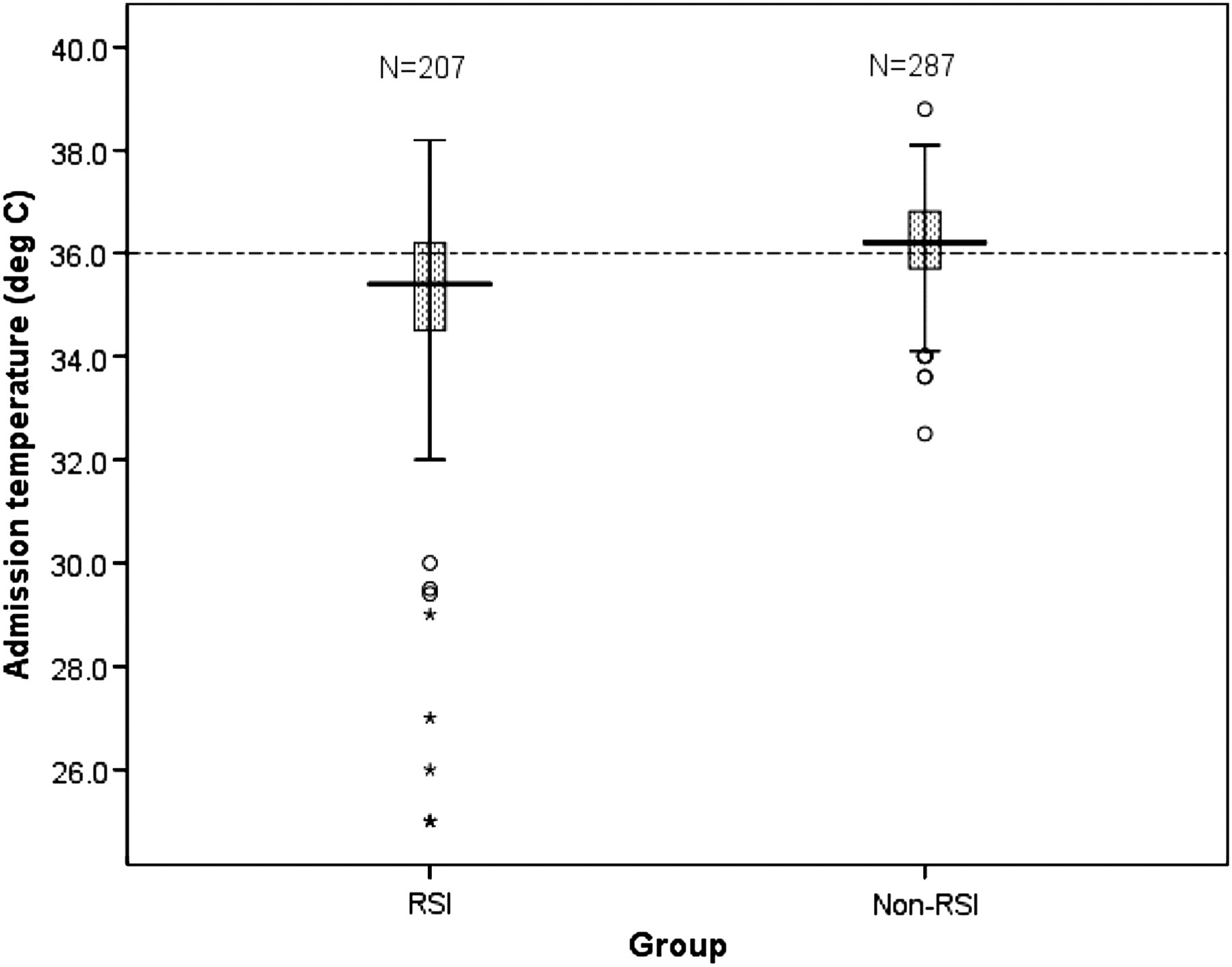
There was a significant difference in body temperature on admission between the RSI group (N=207) and the non-RSI group (N=287), the mean (SD) temperature being 35.0 (2.1) vs 36.2 (1.0)°C, respectively (p<0.001) (95% CI for the mean difference 0.9 to 1.5) (table 1, figure 1). A significant number of the anaesthetised patients had a temperature below 35°C (figure 2).

Box plot of the two study groups showing the median line, IQR, and the boundaries (maximum and minimum) of the temperature observations. The dotted line represents the hypothermia cut-off point. Asterisks indicate extreme values (more than 3 IQRs from the end of the box). Open circles indicate outliers (more than 1.5 IQRs but less than 3 IQRs from the end of the box). p<0.001 (Mann–Whitney U test). RSI, rapid sequence induction.

Admission body temperatures. Scatter diagram of individual points for anaesthetised patients. Solid lines show mean temperature with 95% CIs. The dotted line represents the hypothermia cut-off point.
Using the months of the year as an independent grouping variable for the RSI patients showed that the mean body temperatures within the 12 groups were not identical (p=0.001; Kruskal–Wallis test), indicating that population differences exist. However, there was significant heterogeneity of variance within the groups (Levene's test), and conservative post hoc tests adjusted for unequal variances and sample sizes revealed no solid findings (Tamhane T2, Dunett's T3) (figure 3). Using liberal criteria, a tentative difference in temperature between August and November was found: median temperature (IQR) (°C) 36.3 (3.9) and 35.0 (2.9), respectively, p=0.047 (Games-Howell).

{kind=link}
{kind=link}
{kind=link}
Error bars for the rapid sequence induction patients showing mean admission body temperature with 95% CIs during the year.
Discussion
In this retrospective 3.5 year chart review, anaesthetised adult trauma patients had a significantly lower mean body temperature on hospital admission than non-anaesthetised patients (35.0 vs 36.2°C, respectively). The mean difference of 1.2°C (95% CI 0.9 to 1.5) may seem small, but is potentially clinically significant and may influence outcome in critically injured patients.
There are many factors that could have influenced the temperature, including external temperature, severity of the injury, scene time, and impairment of homoeostasis due to anaesthetic agents. Age discrepancy among the groups may also be an explanation, as elderly people are more prone to hypothermia because of reduced heat-generating capacity, thinner skin, and thermoregulatory failure.16 23 CNS trauma due to severe head injury may prevent conservation of body heat and is another potential reason for temperature mismatch. The degree of isolated head injury (AIS ≥3) and ISS >15 were both higher in the RSI group.
Temperature triggering vasoconstriction and sweating differ between men and women, thresholds for both being 0.4°C higher in women.16 24 This could potentially contribute to a temperature bias. However, no significant gender difference was found in the groups studied.
Our data do not allow comparisons to be made between different causes.
In general, medical classification of hypothermia due to environmental exposure only is defined as core temperature below 35°C in humans. With concomitant injury, a separate classification is developed defining hypothermia as a core temperature below 36°C.25 26 This trauma classification is recommended by current advanced trauma life support guidelines13 and for patients undergoing anaesthesia.14 Despite this, the literature is somewhat inconsistent regarding numerical values used to describe hypothermia.
Admission hypothermia (body temperature ≤35°C) has been found to correlate independently with increased mortality among injured patients.5–8 A significant number of the anaesthetised patients in our series had a temperature below 35°C. Luna et al2 defined hypothermia as oesophageal temperature ≤36°C when they prospectively studied 94 severely injured patients intubated prehospital or in the emergency room, and found that the initial temperature correlated with survival. There is no apparent protective effect of hypothermia in trauma patients,8 with the possible exception of short-term improvement for a subgroup of isolated head-injured patients with Glasgow Coma Scale 5–7 subjected to moderate therapeutic hypothermia for 24 h.27 However, a meta-analysis has suggested that hypothermia is not beneficial in the treatment of severe head injuries.28
Preventing and managing the common finding of accidental hypothermia in trauma patients is a potentially critical step in reducing poor outcome. Appropriate measures for correction and avoidance of hypothermia should be vigorously instituted in the field without delay and continue through all phases of care.29 Ideally, prehospital temperature conservation and rewarming should be a priority and pursued as vigorously as temperature conservation in the operating theatre.25
For our data, no robust seasonal body temperature variation was found, which is in accordance with previous observations.2 23
These findings led to the adoption of a proactive heat conservation and active rewarming policy in our service. We reformulated our prehospital packaging and hypothermia SOP, focusing more aggressively on ‘E’ (Exposure) in the ABCDE of resuscitation (appendix 1; online only).
The limitations of this study are those inherent in retrospective medical record reviews where data have been collected in a clinical context. Firstly, a substantial portion of data was missing. Well over 60% of the patients did not have temperature data recorded on admission. However, there is no a priori reason for more or less under-reporting in one of the two groups, although a skew in temperature recording was found favouring the RSI group. Secondly, the site of temperature assessment was not recorded. It is local policy to measure temperature tympanically with few exceptions. Thirdly, the differences in coding and reporting across the two data sources posed a challenge in linkage and potentially a risk of missing data. To eliminate this error, a quality assurance check was performed before the datasets were combined.
Conclusion
Accidental hypothermia is shown to be an independent factor for a poor outcome for trauma patients. Historical data show a high rate of hypothermia in trauma patients and a particularly high rate in those who undergo prehospital anaesthesia. On the basis of this, London HEMS introduced a proactive temperature management policy for this patient group. For our service in an urban air ambulance environment, an active warming blanket in combination with bubble wrap has been shown to be a feasible and practical solution for the seriously injured anaesthetised patient. The next stage of this process will be to assess the success of the warming policy, and, if it is successful, ultimately to determine changes in outcome.
Acknowledgments
We are indebted to RLH Trauma Nurse Coordinator Anita West and HEMS Research Sister Elizabeth Foster for their assistance with the data collection.
References
Supplementary materials
Web Only Data emj.2009.086967
Files in this Data Supplement:
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.