Article Text

Abstract
Objectives To examine whether the predictive value of the early warning score (EWS) could be improved by including rapid lactate levels, and to compare the modified EWS with the pre-existing risk scoring systems.
Design Retrospective observational study in South Korea.
Setting An urban, academic, tertiary hospital.
Participants Consecutive adult patients who were admitted to the medical intensive care unit via the emergency department (ED).
Outcome measures A newly developed EWS—the VitalPAC EWS (ViEWS), was used in the present study. Lactate level, ViEWS and HOTEL score were obtained from patients at presentation to the ED, and APACHE II, SAPS II and SAPS III scores were obtained after admission. The area under curve of each risk scoring system for in-hospital, 1-week, 2-week and 4-week mortality was compared.
Results 151 patients were enrolled and the mortality was 42.4%. The ViEWS-L score was calculated as follows: ViEWS-L score=ViEWS+lactate (mmol/l) according to the regression coefficient. The mean ViEWS-L score was 11.6±7.3. The ViEWS-L score had a better predictive value than the ViEWS score for hospital mortality (0.802 vs 0.742, p=0.009), 1-week mortality (0.842 vs 0.707, p<0.001), 2-week mortality (0.827 vs 0.729, p<0.001) and 4-week mortality (0.803 vs 0.732, p=0.003). The ViEWS-L score also had a better predictive value than the HOTEL and APACHE II scores. The predictive value of ViEWS-L was comparable with SAPS II and SAPS III.
Conclusions The ViEWS-L score performed as well as or better than the pre-existing risk scoring systems in predicting mortality in critically ill medical patients who were admitted to the medical intensive care unit via the ED.
- Early warning score
- lactic acid
- critically ill patient
- mortality
- emergency care systems
Statistics from Altmetric.com
Introduction
The early warning score (EWS) was introduced to identify adult patients at risk for death early and to predict their clinical outcome.1–3 The EWS comprises only physiological variables and is regarded as a simple and fast bedside tool to assess adult patients. The chosen physiological variables are based on studies associated with physiological abnormalities and mortality,4–6 and the benefits of the EWS are well established.7–9
In critically ill patients, hyperlactatemia is associated with increased risk of mortality.10–12 Additionally, lactate levels can be obtained in a few minutes using commercially available machines. Therefore, incorporating rapid lactate levels into the EWS is supposed to increase the ability of the EWS to identify adult patients at risk for poor clinical outcomes when they present at the emergency department (ED).
Pre-existing risk scoring systems, such as the acute physiology and chronic health evaluation (APACHE II) and the simplified acute physiology score II (SAPS II), contain many parameters that must be measured during the first day after admission to the intensive care unit (ICU), and SAPS III contain parameters that must be measured during the first hour after ICU admission. Therefore, it may be interesting to compare a modified EWS with rapid lactate levels, which is available in a few minutes, to these risk-scoring systems in critically ill medical patients. A recently introduced risk score, Hypotension, Oxygen saturation, low Temperature, ECG change and Loss of independence (HOTEL), was also compared with the modified EWS.13
Objectives
The aim of the present study was to address two main questions. First, can the modified EWS using lactate levels improve mortality predictions in critically ill medical patients admitted via the ED compared with the EWS alone? Second, can the modified EWS predict mortality better than the pre-existing risk-scoring systems?
Methods
Study design and setting
This retrospective, observational study was approved by the institutional review board of the study hospital and the requirement for consent was waived.
The study was conducted in a 1000-bed, urban, academic, tertiary-care hospital in South Korea with an annual ED census of 34 000. The study hospital offers medical, surgical, coronary, neurological and paediatric ICUs. The medical ICU (MICU) in the study hospital has 14 beds, each bed equipped with a monitoring system and a mechanical ventilator. The ratio of patients to nurses is approximately 3:1.
When patients present to the ED, triage nurses assess their vital signs, including systolic blood pressure, diastolic blood pressure, pulse rate, respiratory rate, body temperature, peripheral oxygen saturation and central nervous system status. Central nervous system status was recorded using the alert/verbal/painful/unresponsive scale. A complete history was taken and a full physical examination was performed by the attending physician in the ED. Laboratory tests and radiological evaluations were conducted as necessary. Medical records were computerised after patients were discharged.
Selection of study sample
Consecutive adult patients older than 18 years who were admitted to the MICU via the ED between 1 April 2010 and 31 March 2011 were included in the present study. We excluded patients whose medical records lacked one or more elements needed to establish a modified EWS, HOTEL, APACHE II, SAPS II or SAPS III score.
Main outcome measures and data sources
Demographics, clinical data, physical findings and laboratory results at ED presentation were collected by trained abstractors following the guidelines recommended by Gilbert et al.14 Clinical and laboratory variables required to calculate the APACHE II, SAPS II and SAPS III scores after MICU admission were collected in the same manner. Survival status was determined from discharge records.
The EWS used in this study is shown in table 1. The VitalPAC EWS (ViEWS) was chosen for the present study among many EWSs, which was recently developed and validated from the national database set.15 Urine output was not included in this version. Because the study hospital did not use ViEWS during the study period, ViEWS scores upon presentation to the ED were calculated based on the collected data. HOTEL scores upon presentation to the ED were also calculated in the same manner.
VitalPAC early warning score (ViEWS) used in this study
The main outcomes were hospital mortality, 1-week, 2-week and 4-week mortality.
Lactate levels were primarily measured using arterial blood, but venous blood lactate levels were also used. Lactate levels were measured using a Stat Profile Critical Care Xpress Analyser (Nova Biomedical, Waltham MA, USA). The measuring range for lactate in this machine is 0.3–20 mmol/l. Lactate levels that were reported out of range were excluded from the analysis.
Statistical analysis
Normally distributed data are expressed as the mean±SD. Non-normally distributed data are expressed as the median and IQR. Categorical variables are reported as percentages. Comparison of normally distributed data was performed using an independent-samples t-test. For non-normally distributed data, comparisons were performed using the Mann–Whitney U test. For categorical data, the χ2 test with a Yates correction for 2×2 tables was used. Results were considered significant at a threshold of p<0.05 (two-tailed).
Associations between the presence and absence of outcomes and each potential diagnostic determinant were first quantified using univariate logistic regression analyses. Then, multivariate logistic regression analysis was performed for trend factors (p<0.10) in the univariate analysis. Regression results are expressed as ORs with 95% CIs.
To modify the ViEWS with lactate level we performed logistic regression analysis, setting hospital mortality as the outcome variable and the ViEWS score and lactate levels as predictor variables. In addition, we rounded regression coefficients in this model to the nearest integer. Modified ViEWS with lactate level was named as ‘ViEWS-L’ score.
The predictive values of the ViEWS and ViEWS-L score were tested using the areas under the receiver operating characteristic (ROC) curves analysis. The SEM and p values for the ROC curves, and comparisons between them were calculated following the methods of Hanley and McNeil.16 ,17 The same area under the curve (AUC) method was used to compare ViEWS-L, HOTEL, APACHE II, SAPS II and SAPS III.
Analyses were conducted using SPSS for Windows V.17.0 and SAS V.9.1 .
Results
Patient characteristics
During the study period, 165 patients met the eligibility criteria. Among them, we excluded 14 patients whose medical records were insufficient to determine ViEWS-L score because of missing initial lactate level, while it was possible to determine other risk scores.
A total of 151 patients were enrolled in the study. The mean age was 65.3±17.2 years and 102 (67.5%) patients were men. The mortality rate was 42.4% (64/151). Hypertension was the most frequent comorbidity (43.0%) followed by diabetes mellitus (25.8%), malignancy (20.5%), stroke (13.9%), chronic liver disease (12.6%) and chronic kidney disease (11.9%). There were no significant differences between survivors and non-survivors in most demographic characteristics, although chronic liver disease and malignancy were more frequent in non-survivors. Systolic blood pressure, diastolic blood pressure and peripheral O2 saturation were also significantly lower in non-survivors (table 2).
Baseline characteristics of enrolled patients
Sepsis caused greater mortality (65.6%) than non-septic conditions (34.4%). Pneumonia was the most frequent discharge diagnosis (53.0%), followed by acute renal failure (7.9%) and gastrointestinal bleeding (6.6%). In non-survivors, pneumonia was also the most frequent discharge diagnosis (54.7%), followed by gastrointestinal bleeding (9.4%), acute renal failure (6.2%), alcoholic ketoacidosis (4.7%) and portosystemic encephalopathy (4.7%). The details of patient diagnoses are displayed in table 3.
Discharge diagnosis of enrolled patients
The mean lactate level for the entire sample was 4.7±4.6 mmol/l, ranging from 0.3 to 19.8 mmol/l. The lactate level was significantly higher in non-survivors (7.1±5.4 mmol/l vs 3.0±2.9 mmol/l, p<0.01). There were also significant differences in white blood cell count, platelet levels, prothrombin time, activated partial thromboplastin time, total bilirubin, HCO3 and albumin levels between survivors and non-survivors (table 3).
The mean ViEWS for all patients was 6.9±4.1. The mean HOTEL score was 1.9±1.1, mean APACHE II score was 25.0±9.4, mean SAPS II score was 60.7±22.5 and mean SAPS III score was 66.9±15.9. All scores were significantly higher in non-survivors than in survivors (p<0.01; table 1).
The lactate level and ViEWS were significant predictors for hospital mortality by univariate logistic regression analysis. Lactate remained significant by multivariate logistic regression after controlling for cormorbid diseases, vital signs, laboratory markers and ViEWS (adjusted OR: 1.22, 95% CI 1.03 to 1.45, p=0.021). Additionally, history of malignancy (adjusted OR: 10.19, 95% CI 3.25 to 31.96, p<0.000) and white blood cell count (adjusted OR: 0.93, 95% CI 0.87 to 0.99, p=0.034) were significant predictive factors for hospital mortality by multivariate logistic regression (table 4).
Logistic regression analysis for hospital mortality
Modification of ViEWS with lactate levels: ViEWS-L score
We designed the ViEWS-L score to improve the predictive value of the ViEWS by including lactate levels. On a logistic regression analysis with hospital mortality as the outcome variable and ViEWS and lactate levels as the predictor variables, the coefficient of ViEWS was 0.169 and that of lactate was 0.208. We rounded these coefficients up and ViEWS-L score was determined using the following formula: ViEWS-L score = ViEWS + lactate (mmol/l). The mean ViEWS-L score for all patients was 11.6±7.3. Figure 1 displays the number of patients and mortality in each of the four groups classified by cut-off scores of 5, 10 or 15. The group with a score below five contained 30 patients with a mortality rate of 13.3%. The group with a score between 5 and 10 contained 47 patients with a mortality rate of 23.4%. The group with a score between 10 and 15 contained 33 patients with a mortality rate of 48.5%. The group with a score above 15 contained 41 patients with a mortality rate of 80.5%.

The distribution of ViEWS-L score and associated hospital mortality of enrolled patients.ViEWS-L, vitalPAC early warning score-lactate.
ViEWS versus ViEWS-L score
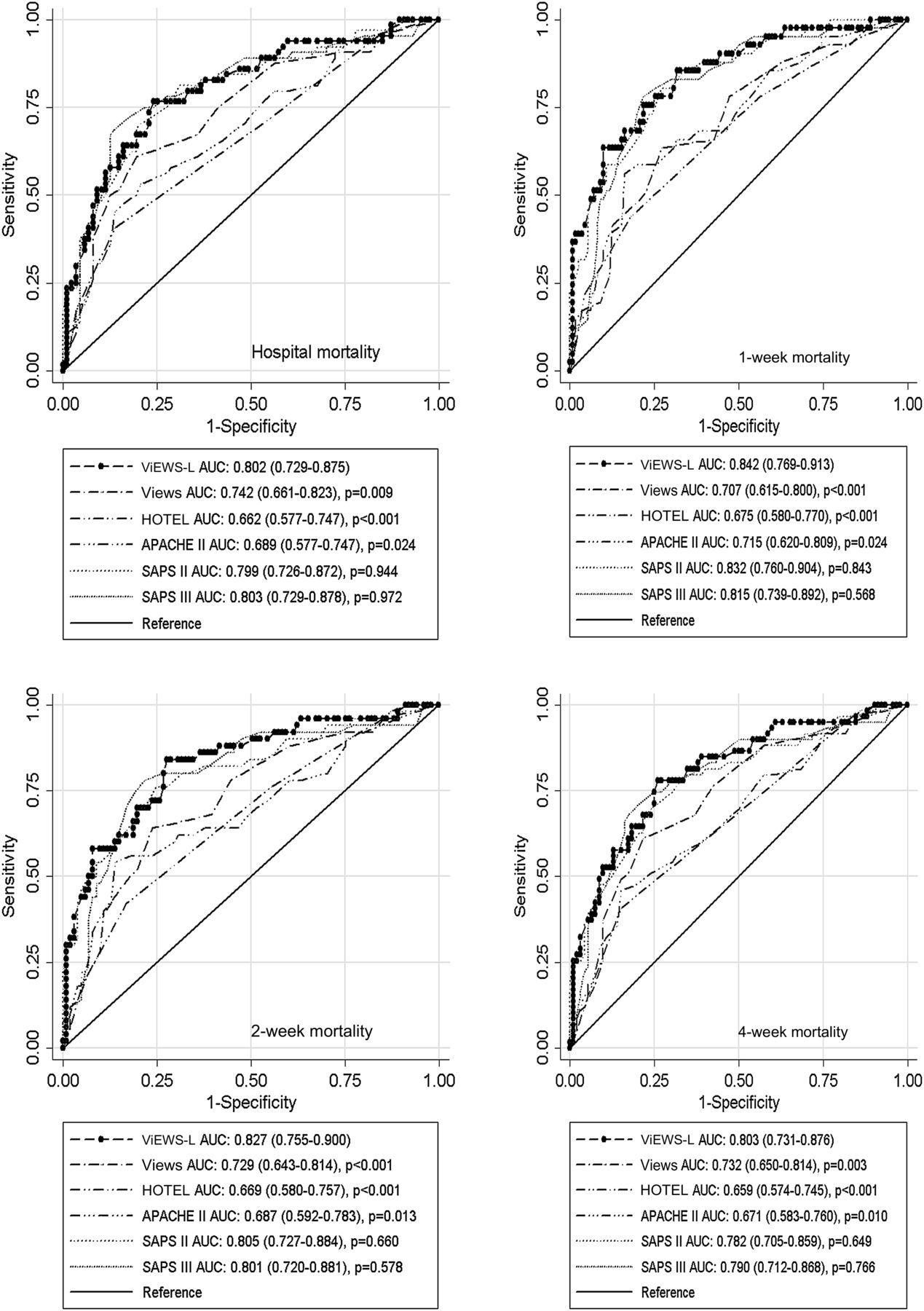
The predictive values of the ViEWS and ViEWS-L score for hospital mortality, 1-week mortality, 2-week mortality and 4-week mortality were compared. The ViEWS-L score was superior to the ViEWS for all outcomes (figure 2). The AUCs of the ViEWS and ViEWS-L score for hospital mortality were 0.742 and 0.802 (p=0.009), 0.707 and 0.842 (p<0.001) for 1-week mortality, 0.729 versus 0.827 (p<0.001) for 2-week mortality and 0.732 versus 0.803 (p=0.003) for 4-week mortality, respectively.

{kind=link}
{kind=link}
Comparison of area of under the receiver operating characteristic curve of risk scoring systems for each mortality outcome. Data was presented with 95% CIs and p value was noted compared with the ViEWS-L score. APACHE, acute physiology and chronic health evaluation; AUC, area under curve; HOTEL, Hypotension, Oxygen saturation, low Temperature, ECG change and Loss of independence; SAPS, simplified acute physiology score; ViEWS-L, vitalPAC early warning score-lactate.
ViEWS-L score versus HOTEL, APACHE II, SAPS II and SAPS III score
The predictive value of the ViEWS-L score was compared with other pre-existing risk scores (figure 2). The predictive value of the ViEWS-L score was superior to the HOTEL score for all four outcomes (0.802 and 0.662, p<0.001 for hospital mortality; 0.842 and 0.675, p<0.001 for 1-week mortality; 0.827 and 0.669, p<0.001 for 2-week mortality; 0.803 and 0.659, p=0.003 for 4-week mortality, respectively). The predictive value of the ViEWS-L score was also superior to the APACHE II score for all four outcomes (0.802 and 0.689, p=0.024 for hospital mortality; 0.842 and 0.715, p=0.024 for 1-week mortality; 0.827 and 0.687, p=0.013 for 2-week mortality; 0.803 and 0.671, p=0.010 for 4-week mortality, respectively). The SAPS II score was comparable with ViEWS-L score in predicting mortality for all four outcomes (0.802 and 0.799, p=0.944 for hospital mortality; 0.842 and 0.832, p=0.843 for 1-week mortality; 0.827 and 0.805, p=0.660 for 2-week mortality; 0.803 and 0.782, p=0.649 for 4-week mortality). The SAPS III score was also comparable with ViEWS-L score in predicting mortality for all four outcomes (0.802 and 0.803, p=0.972 for hospital mortality; 0.842 and 0.815, p=0.568 for 1-week mortality; 0.827 and 0.801, p=0.578 for 2-week mortality; 0.803 and 0.790, p=0.766 for 4-week mortality, respectively).
Discussion
We demonstrated that modified ViEWS with rapid lactate levels (ViEWS-L) exhibited improved ability to predict mortality in (unselected or mixed) critically ill medical patients compared with ViEWS alone. Furthermore, the performance of the ViEWS-L score was comparable with or better than several pre-existing, validated risk scoring systems, such as the HOTEL, APACHE II, SAPS II and SAPS III scores.
Researchers have developed risk-scoring tools for patients presenting to the ED. Previous studies have shown that physiological data collected at presentation can be used to predict mortality without requiring laboratory data.5 ,8 ,18 However, one review reported that scores based on physiological data were not adequate (AUC ≥0.800) in consecutive patients in medical assessment unit).19 Scoring systems based on combined physiological and laboratory data have also been introduced.20 ,21 However, these scoring systems may be too time complex and time consuming to rapidly identify patients at risk in the ED. Recently, Kellett et al introduced the HOTEL score showing AUC of 86.5% for the derivation group and 85.4% for the validation group for early mortality between 15 min and 24 h after admission in the mixed medical emergent cohort.13
Otherwise, the usefulness of pre-existing risk-scoring systems such as the SAPS II or APACHE II has been evaluated.22–24 These scoring systems are moderately to highly accurate for predicting hospital mortality in patients presenting to the ED, with ROC values ranging from 0.72 to 0.91. However, these scoring systems may not be useful in a broad clinical setting, particularly because they require the inclusion of many variables that are not available instantly.
In the UK, EWSs and the recently developed version, ViEWS, are widely used to identify patients at risk in clinical settings.15 ,25 ViEWS includes only six physiological variables, all of which can be measured within a few minutes, allowing for rapid recognition of patients at risk. An additional parameter, lactate levels can also be assessed within a few minutes from as little as 60 μl of whole blood using commercially available machines. Therefore, the ViEWS-L score can also be determined in a few minutes. Simplicity, speed and ease-of-use of the ViEWS-L score are substantial merits over other scoring systems. Because the ViEWS-L score performed better than or similar to pre-existing risk scoring systems, ViEWS-L may be promising as a reliable and rapid risk scoring system for critically ill medical adult patients upon presentation to the ED. We suggest that the ViEWS-L may be used to modify ED treatment and to assess treatment response; however, more data is required to verify this use.
Elevated blood lactate is common in critically ill patients and is associated with adverse outcomes. In a study performed by Khosravani et al hyperlactatemia defined by a lactate level >2 mmol/l was an independent factor associated with mortality in 12 000 critically ill adult patients, admitted to the ICUs of a regional healthcare system.10 Although subgroup analyses based on diagnosis or ICU category are not performed in this study, what is important is that hyperlactatemia is associated with increased mortality in a large mixed cohort of medical and surgical patients. Recent studies suggest that hyperlactatemia is a sensitive indicator of mortality in critically ill patients suffering from multiple diseases including sepsis, coronary or cerebral vascular disease and trauma.26 ,27 Using lactate as a parameter to determine the patient's general status may be feasible for multiple disease states.
Previously validated risk scoring systems in critically ill patients such as APACHE II, SAPS II and SAPS III score, were comparable or inferior in performance with the ViEWS-L score in this study, even though they contain more variables, possibly because of treatment during the ED stay. Nowadays, EDs play a major role in treating critically ill patients because they contain laboratory and radiological facilities. Additionally, hospital occupancy, including ICU occupancy, is increasing. Therefore, treating critically ill patients during an ED stay becomes substantial. Consequently, in many cases the severity of an illness may change from the time the patients present to the ED to the time they are admitted to the ICU. If appropriate treatment is provided in the ED, the severity of critically ill patients would improve by the time they are admitted to the ICU. Thus, the APACHE II, SAPS II and SAPS III scores, which are calculated at ICU admission, may be less sensitive in predicting hospital mortality than the ViEWS-L score.
Limitations
The results of this study must be interpreted considering some limitations. First, the number of enrolled patients was small. However, despite the small sample size, there were statistical differences in each measure of mortality, suggesting that a similar larger multicentre study including a broader range of patients is warranted. Second, some patients were excluded from the study because their initial lactate levels on presentation to the ED were unavailable. Excluding these patients may have biased the results of our analyses.
Originally, ViEWS and other EWSs were designed for use in the general ward, where abnormal scores resulted in escalation of care. The present study is based on data from critically ill medical patients already admitted to the ICU. The lack of a comparison group of patients who were not admitted to the ICU is a major limitation to using ViEWS-L score to determine whether to admit patients to the ICU from the ED. Therefore, we cannot suggest any ViEWS-L score cut-off for ICU admission. Our next study, which will enrol all critically ill patients who visited the ED, may be able to provide this information.
Additionally, the result of this study must be interpreted carefully because outcome of this study is mortality, not necessity of some critical intervention or triage accuracy. While the APACHE II or SAPS II scores were devised for quality assurance, the ViEWS and HOTEL scores were developed for triage purposes. The result of this study does not mean that the ViEWS-L score is better than the ViEWS or HOTEL scores to identify patients for immediate intervention or to triage patients presenting to the ED.
Conclusion
A modified ViEWS with rapid lactate level (ViEWS-L) was better able to predict values for hospital, 1-, 2- and 4-week mortality than the ViEWS alone in critically ill medical patients. Furthermore, the ViEWS-L score was a better predictor of mortality than the HOTEL and APACHE II scores, and was comparable with the SAPS II and SAPS III scores.
What is known on this topic
-
The VitalPAC Early Warning Score (ViEWS) is used at the bedside to stratify risk in some countries.
-
Previous risk scoring systems, such as acute physiology and chronic health evaluation II (APACHE II), simplified acute physiology score II (SAPS II) and SAPS III scores, have limitations to apply rapidly for critically ill medical patients presenting to the emergency department.
-
Rapid assessment of lactate levels are supposed to enhance the predictive value of the ViEWS.
What this study adds
-
We designed the ViEWS-L score by modifying the ViEWS to include rapid lactate level.
-
The ViEWS-L score performed as well as or better than previous risk scoring systems for predicting mortality in critically ill medical patients.
References
Footnotes
-
Competing interests None.
-
Patient consent This is a retrospective chart review study and waiver of patient consent was given by the institutional review board of the study hospital.
-
Ethics approval The study was approved by the institutional review board of Chonbuk National University Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.