Article Text

Abstract
Fractures of the femur are common orthopaedic emergencies presenting to emergency departments (ED). Femoral nerve block (FNB) is a fast, safe and effective means of providing pain relief to these patients. With the aim to analysing the variation in current practice of giving FNB in patients with fractured femur in the UK, we carried out a telephonic national survey. Out of 252 EDs contacted, 230 departments participated in the survey (91% response rate). The survey showed that 74% EDs in the UK had access to ultrasound, but only 10% EDs gave FNB regularly under ultrasound guidance. In total, 46% of EDs gave FNB by blind technique. Therefore, ultrasound-guided FNB is an underutilised method of providing pain relief for fractured femur patients. The main reasons for not using ultrasound for FNB were: lack of training, participants’ confidence in giving an effective and safe FNB block blindly and time constraints. The literature review suggests that ultrasound-guided FNB has a faster onset of action, is more effective and safer than the FNB given with nerve stimulator (NS) or blindly, and probably needs lower local anaesthetic dose. The use of NS for FNB in ED might not be practical because of the likelihood of the pain resulting from the movement of the affected limb due to the contraction of the muscles caused by nerve stimulation and because of additional training needed in using NS. The studies comparing FNB given using ultrasound or NS, or given blindly, have been done in the perioperative settings. To date, there has been no randomised controlled trial in ED setting comparing FNB given blindly or under ultrasound guidance. Such a study might have provided a good evidence for modifying the current practice of blind FNB.
- ultrasound
- musculo-skeletal
- analgesia/pain control
Statistics from Altmetric.com
Introduction
Fractures of the femur are common orthopaedic emergencies presenting to emergency departments (ED). These patients need effective analgesia as part of their initial management. In spite of the guidelines of the College of Emergency Medicine,1 there is sometimes reluctance to give adequate analgesia to these patients especially in elderly, frail patients and patients with concurrent head or chest injury. Options for providing pain relief to patients with fractured femur include parenteral injections, oral analgesics, entonox and nerve blocks. Femoral nerve block (FNB) is a fast, safe and effective means of providing pain relief to patients with fracture of the femur (neck, extracapsular fracture, shaft or distal femur).2–6 After a successful block, the subsequent requirement of opioids is reduced which avoids potential side effects such as nausea, vomiting, sedation, delirium and respiratory depression, especially in elderly patients.5 ,7 ,8
Techniques of femoral nerve block
Blind femoral nerve block
FNB provides good pain relief to patients with diaphyseal and distal femur fractures.4 ,6 ,9 It is performed with the patient supine. After preparing the skin, the needle is inserted 1 cm below the inguinal ligament and 1 cm lateral to the femoral artery at a 90° angle to the skin to a depth of about 3 cm.9 ,10 (figure 1) If paraesthesia occurs, the needle is slightly withdrawn. Local anaesthetic (LA) is infiltrated around the femoral nerve, fanning out the needle laterally to about 3 cm from the artery.10

Schematic representation of the anatomy for the femoral nerve block
Three in One block (TiO block)
About 40 years ago, Winnie et al11 devised an inguinal paravascular approach of blocking the femoral, obturator and lateral cutaneous nerve with a single injection. This approach came to be known as Three in One block.11 This block provides good pain relief to patients with fractured neck of femur.5 ,9 It is similar to FNB given blindly with the same puncture site, except that the needle needs to be directed slightly cephalad.9 ,11 It requires larger LA volume and compression distal to the injection site for about 5 minutes after the injection.9 ,11 It is believed that the distal pressure helps the proximal spread of LA to the level of lumbar plexus along the perineural sheath to block the obturator and lateral femoral cutaneous nerves to provide better analgesia for fractures of the proximal femur.9 ,11 However, this concept of TiO block has been challenged as all three nerves are rarely blocked together, particularly the obturator nerve.12–14
Fascia iliaca block
This is another blind technique to achieve block of the femoral, lateral cutaneous and obturator nerves. A short bevel needle is inserted 1 cm distal to the junction of medial 2/3 and lateral 1/3 of the line joining anterior superior iliac spine with the pubic tubercle.15 A ‘pop’ is felt as the needle goes through the fascia lata, and again as it penetrates the fascia iliaca.15 (figure 1) LA is injected into fascia iliaca compartment to achieve the block.
FNB using nerve stimulator
Stand on the side of the patient on which the FNB is to be given. Mark the needle insertion site which is immediately lateral to the femoral artery at the level of the femoral crease. Under all-aseptic conditions, infiltrate LA subcutaneously at the site of insulated needle insertion while palpating the femoral artery. Insert the insulated needle immediately lateral to the artery and advance it in the sagittal and slightly cephalad plane. Initially, set the nerve stimulator (NS) to deliver 1.0 mA (2 Hz, 100 µs). With proper needle position, advancement of the needle should not result in any local twitches; the first response is usually that of the femoral nerve, in the form of movements of the patella due to contraction of quadriceps femoris. After the initial stimulation of the femoral nerve is obtained, gradually decrease the stimulating current until twitches are still seen or felt at 0.2–0.4 mA current. This typically occurs at a depth of 2–3 cms.16 If twitches are seen with <0.2 mA, slightly withdraw the needle as the needle tip might have penetrated the femoral nerve. After negative aspiration for blood, slowly inject about 20 ml of LA, in 5 ml aliquots aspirating repeatedly, and constantly monitoring the patient for any symptoms/signs of LA toxicity.
FNB under ultrasound guidance
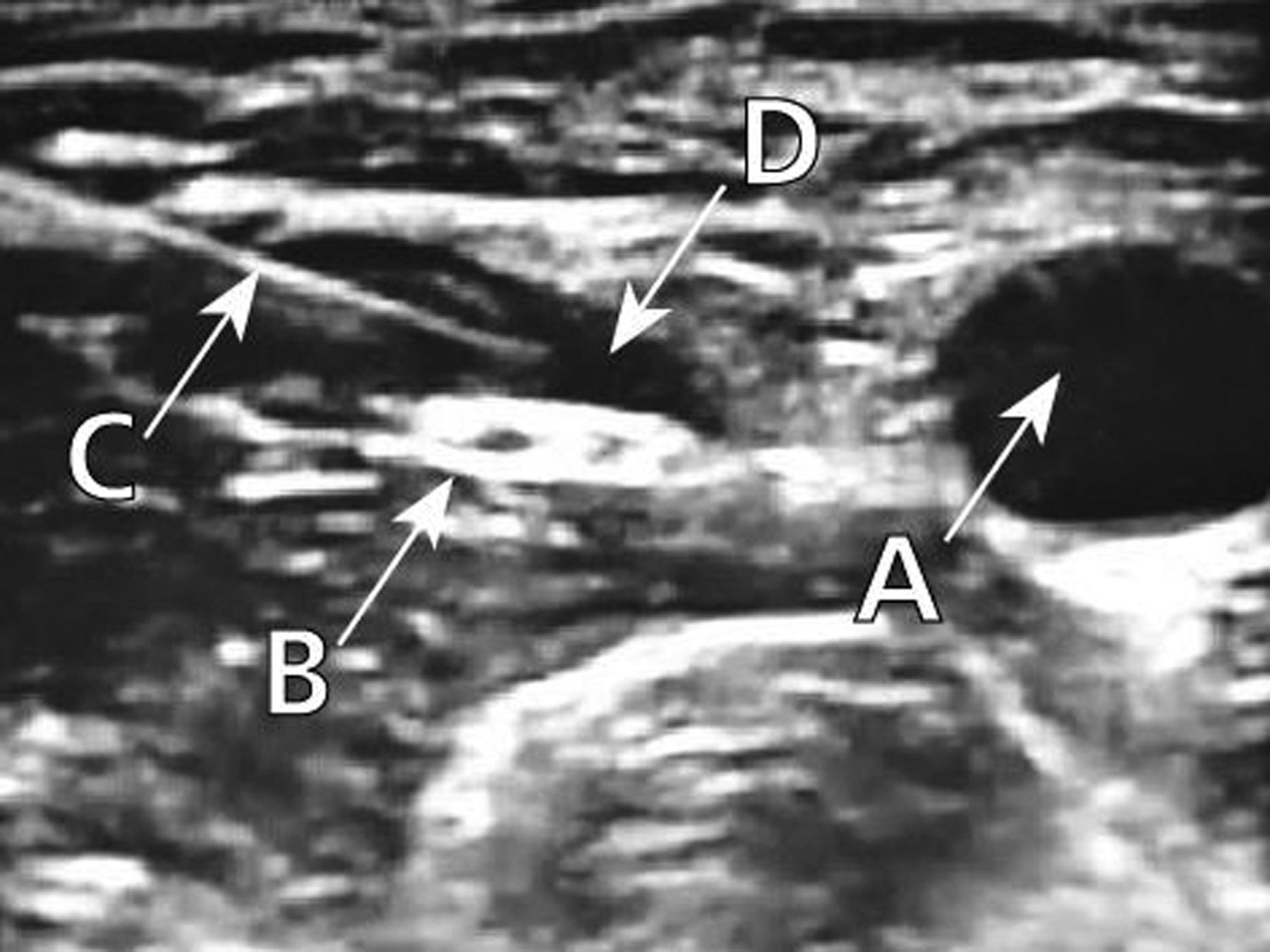
A high-frequency (≥10 MHz) linear probe is required because of relatively superficial location of the femoral nerve.17 The probe is placed transversely across the inguinal crease to view the neurovascular bundle, the iliacus muscle and the fascia iliaca. The puncture is performed lateral to the ultrasound probe in the ‘in-plane’ approach, or below the probe in the ‘out-of-plane’ approach, using a 22 gauge short bevel 4 cm needle.17–20 The needle tip is placed under the fascia iliaca and above the ilacus muscle lateral to the femoral artery. The femoral nerve is often better visualised as the injected LA encircles it (figure 2).

Ultrasonographic view after injection of local anaesthetic around the femoral nerve using ‘in-plane’ approach. A: femoral artery; B: femoral nerve; C: needle; D: local anaesthetic around the femoral nerve
UK national survey
With the aim of analysing the variation in current practice of giving FNB in patients with fractured femur in the UK, we carried out a national telephonic survey. The UK national survey was conducted by both the authors. The list of all the EDs was obtained from The College of Emergency Medicine. The phone numbers of the EDs were obtained from the internet by both EV and RM. After piloting the survey in the Mersey region, RM carried out a telephonic national survey in May 2009. The questions asked in the survey have been enlisted in the box 1.
Survey questionnaire
Question 1. Do you have an ultrasound machine in your department?
Answer: Yes or No.
Question 2. Do you give femoral nerve lock (FNB) to patients with fractured femur (neck, extracapsular, shaft, distal femur)?
Answer: No, occasionally or regularly.
Question 3. If you give FNB, do you give the FNB under ultrasound guidance?
Answer: Yes or No.
Question 4. If you do not give the FNB under ultrasound guidance, what are the reasons for giving the FNB without ultrasound guidance?
Answer: Training issue, time issue or any other reason.
Out of 252 EDs contacted, 230 departments participated in the survey (91% response rate). All the questionnaires were answered by middle grade doctors (83%), consultants (14%) or associate specialists (3%). While conducting the survey, the authors made sure that the information was collected from one of the regular senior doctors who had a good knowledge about his department.
UK distribution of EDs surveyed
England had the maximum participation in the survey, probably because there are more hospitals in England compared with other constituent countries of the UK. The UK distribution of the EDs which participated in the survey has been shown in figure 3 and table 1.
UK distribution of EDs surveyed, frequency of giving femoral nerve blocks, and availability of ultrasound machines

{kind=link}
{kind=link}
{kind=link}
UK distribution of emergency departments which participated in the survey
Key findings of the survey
-
Although 74% EDs in the UK had ultrasound, only 10% of these departments gave FNB under ultrasound guidance regularly, and 20% occasionally (table 1).
-
Totally, 32% of the EDs preferred to give FNB by blind technique, in spite of having ultrasound in their departments.
-
In total, 46% of EDs in the UK gave the FNB by blind technique regularly.
-
The main reasons for not using ultrasound for FNB were: lack of training (24%), participants’ confidence in giving an effective and safe FNB block blindly (11%) and time constraints (2%) (table 2).
Reasons for not giving femoral nerve block under ultrasound guidance
Review of literature
The literature search was performed using the PICO21 technique:
Patient: In patients with fractured femur
Intervention: Is ultrasound guided femoral nerve block
Comparison: Femoral nerve block given blindly OR with nerve stimulator
Outcome: Safer and more effective (measures: block onset time, complete/incomplete block, duration for which block lasted, dose of local anaesthetic required and complications rate)
The databases and websites which were searched were: Medline (1950–present), EMBASE (1980–present), Cochrane, European Society for Regional Anaesthesia, Regional Anesthesia and Pain Medicine journal, CINAHL (1981–present), TRIP DATABASE, Google and Google Scholar, Bandolier, King's Fund, Current Contents Search, National Institute for Health and Clinical Excellence (NICE), Controlled trial.com, UpTodate and Best Bets. Both RM and EV independently went through the titles ± abstracts of 210 articles which came up during literature search on MEDLINE and EMBASE to look for relevant articles. Any discrepancy was resolved by discussion between the two authors. The references of all the relevant articles were searched manually for cross-references. Professor Peter Marhofer from Vienna, one of the pioneers in the field of ultrasound-guided nerve blocks was also contacted for any unpublished data.
Nerve blocks by blind technique
The first nerve block was performed by William Halsted and Richard Hall.22 Ever since Kulenkampf's original publication,23 eliciting paraesthesia has been an integral part of performing a nerve block by blind technique. This practice was reinforced and perpetuated by the often quoted maxim of Moore, ‘no paresthaesia, no anaesthesia’.24 In 1979, Selander et al, in their study, found that postanaesthetic nerve lesions were more common in patients in whom paraesthesia was elicited.25 They suggested that whenever possible, nerve blocks should be performed without eliciting paraesthesia.25
Nerve blocks using nerve stimulator
An alternative to eliciting paraesthesia is to use a nerve stimulator (NS). In 1962, Greenblatt and Denson published a study on 87 NS guided nerve blocks which had a 100% success rate.26 Doty et al, in their single, blind, randomised, controlled trial (RCT) on 135 patients, demonstrated that nerve blocks given with NSs are more frequently successful as compared with blocks given by direct infiltration without NSs.27 Results of other prospective observational studies also suggest that blocks given with NSs have good success rates.28–31 All these studies were done in perioperative settings.
Both paraesthesia and NS-guided techniques aim to get close to the intended nerve, but without penetrating it. Both these methods, elicitation of paraesthesia or nerve stimulation have modest sensitivity for detection of needle to nerve contact.32 Moreover, the use of NS can cause muscle contraction that can worsen pain and may displace the fracture.33 Therefore, neither method is ideal in ED setting.
Ultrasound-guided nerve blocks
The use of ultrasound for nerve block was first reported in 1978 by La Grange and colleagues who performed supraclavicular brachial plexus blocks using a doppler ultrasound for detection of blood flow to identify blood vessels and inject local anaesthetic in their vicinity aiming to block the accompanying nerves.34 The popularity of use of ultrasound for peripheral nerve blocks has gained momentum in the last 10 years partly because of the improvement in ultrasound technology.17
Potential advantages
Ultrasound has revolutionised regional anaesthesia by allowing the operator to visualise all steps of a block in real time.35 In 1997, Marhofer et al, in their RCT on 40 patients, compared the ultrasound-guided TiO block with the TiO block with a NS. They concluded that ultrasound guidance reduced the block onset time and improved the quality of sensory block. Femoral artery puncture was observed in three cases, all in NS group.36 In 1998, Marhofer et al, in their RCT on 60 patients, again concluded that ultrasound reduced the block onset time and improved the quality of sensory block. In this study, femoral artery puncture was observed in two cases in each of the two NS study groups.37 In both these studies, Marhofer et al did not provide a power calculation, and did not describe the method of randomisation.36 ,37 So, these RCTs raise the possibility of bias or error in methodology.
In 2005, Marhofer et al described the potential advantages of use of ultrasound during nerve blocks like direct visualisation of nerves, vessels and other tissues, real-time control of needle advancement, assessment of LA spread around the nerves and avoidance of muscle twitches.17 In 2007, Casati et al demonstrated that under ultrasound guidance, there was reduction by 42% in the mean effective anaesthetic volume of local anaesthetic for FNB.38 In 2008, Dolan et al, in their study on 80 patients, compared ultrasound-guided fascia iliaca block to loss of resistance technique for fascia iliaca block. They concluded that under ultrasound guidance, there was significant increase in complete sensory loss on thigh and significant increase in incidence of femoral and obturator nerve motor block.15 The limitation of this study was the use of opaque envelops to randomise which is not considered an authentic method of randomisation.15
In 2008, Koscielniak–Nielsen, in a review article, conveyed that ultrasound guidance significantly shortened the block performance time, block onset time and reduced the number of needle passes. He also suggested that ultrasound-guided blocks might be performed using lower LA doses.39 The use of smaller doses of LA is especially useful while managing patients with cardiovascular compromise in whom the dose of LA should be kept to a minimum to prevent unwarranted cardiovascular side effects.36 ,37 In 2009, Abrahams et al, in their meta-analysis, concluded that blocks performed under ultrasound guidance had higher success rate, had faster onset time, lasted longer and had lower risk of vascular puncture (all clinically significant); also took less time to perform, but this result was clinically not significant. Also, there was no statistically significant difference between the ultrasound and NS groups in the incidence of paraesthesia during the block placement or persistent neurological symptoms after the block resolution.40 ultrasound-guided technique is of use especially in patients in whom the anatomical landmarks are difficult to identify, such as in morbid obesity, previous surgery in the area or patients with anatomical anomalies.36 The NICE also supports the use of ultrasound for regional blocks.41
Potential complications
Intraneural injection and vascular injury have been reported during nerve blocks given even under ultrasound guidance.42 ,43 ultrasound imaging technology is expensive, subjective and operator-dependent.17 ,39 ,44 ,45 The incidence of permanent neurological damage after peripheral nerve block, a most feared complication of regional anaesthesia, has been quoted to be in the order of 1 : 5000–1 : 10 000.46 ,47 So, to show a significant difference in terms of nerve safety of ultrasound-guided nerve blocks, a very large study would be required.48
Hopkins has suggested that it is time to change practice and start giving regional blocks under ultrasound guidance.49 With appropriate training, experience and performance, ultrasound techniques have the potential to produce successful nerve blocks with no complications secondary to needle placement.49 Besides good training, a thorough understanding of the anatomy is vital for effective ultrasound-guided nerve blocks.17 ultrasound skills can be rapidly learnt.50
The studies comparing FNB given using ultrasound, or NS, or given blindly, have been done in the perioperative settings. To date, there has been no RCT in ED setting comparing FNB given blindly or under ultrasound guidance. Such a study might have provided a good evidence for modifying the current practice of giving femoral nerve block blindly. Do we really need to wait for such a study which will have resource implications due to need for a large and possible multicentric study; taking into consideration that incidence of permanent neurological damage complication is very low? Should we not extrapolate the results of the perioperative studies, which have proved the superiority of ultrasound-guided FNB over blind FNB, and change our practice to ultrasound-guided FNB? The ability to do the block in real time, following adequate training, also makes it intuitively successful and safer.
Conclusion
The UK national survey has shown that 74% EDs in the UK had access to ultrasound, but only 10% gave FNB regularly under ultrasound guidance. In total, 46% of EDs gave FNB by blind technique. ultrasound-guided FNB is an underutilised method of providing pain relief for fractured femur patients. The main reasons for not using ultrasound for FNB were: lack of training, participants’ confidence in giving an effective and safe FNB block blindly, and time constraints.
The literature suggests that ultrasound-guided FNB has a faster onset time, is safer and more effective than the FNB given with NS or blindly, and needs a lower local anaesthetic dose. It lessens the potential complications, including vascular puncture and reduces the subsequent need for opioids. The technique is operator-dependent and requires training.
The use of NS for FNB in ED might not be practical because of the likelihood of the pain resulting from the movement of the affected limb due to the contraction of the muscles caused by nerve stimulation, and because of additional training needed in using NS.
Based on the current evidence, FNB under ultrasound guidance seems to be a promising technique which should be used in EDs more often for the provision of analgesia to patients with femoral fractures. ED doctors require good basic ultrasound skills and appropriate training in the technique.
Acknowledgments
Mr Patrick Nee, Consultant, Department of Emergency Medicine and Intensive Care, Whiston Hospital, Prescot, for his valuable suggestions and for reviewing the manuscript; Ms Jenni Collins, Medical Photographer and Illustrator, Countess of Chester Hospital, for improving the figures and Sonosite for granting permission to use the ultrasonography image.
References
Footnotes
-
Collaborators RM: Conceived the idea, planned the UK survey, did the survey, analysed the data, did literature search, reviewed the literature and wrote the manuscript. EV: Helped with the UK survey, analysis of data, literature search, literature review and writing of the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.