Article Text

Abstract
Introduction Fresh frozen cadavers are effective training models for airway management. We hypothesised that residual carbon dioxide (CO2) in cadaveric lung would be detectable using standard clinical monitoring systems, facilitating detection of tracheal tube placement and further enhancing the fidelity of clinical simulation using a cadaveric model.
Methods The tracheas of two fresh frozen unembalmed cadavers were intubated via direct laryngoscopy. Each tracheal tube was connected to a self-inflating bag and a sidestream CO2 detector. The capnograph display was observed and recorded in high-definition video. The cadavers were hand-ventilated with room air until the capnometer reached zero or the waveform approached baseline.
Results A clear capnographic waveform was produced in both cadavers on the first postintubation expiration, simulating the appearances found in the clinical setting. In cadaver one, a consistent capnographic waveform was produced lasting over 100 s. Maximal end-tidal CO2 was 8.5 kPa (65 mm Hg). In cadaver two, a consistent capnographic waveform was produced lasting over 50 s. Maximal end-tidal CO2 was 5.9 kPa (45 mm Hg).
Conclusions We believe this to be the first work to describe and quantify detectable end-tidal capnography in human cadavers. We have demonstrated that tracheal intubation of fresh frozen cadavers can be confirmed by life-like waveform capnography. This requires further validation in a larger sample size.
- Resuscitation, Training
- Airway
Statistics from Altmetric.com
Introduction
Cadaveric models provide effective simulation in airway management1 and facilitate airway research that would be unethical in live patients.2 ,3 The gold standard method of confirming tracheal tube placement in the clinical setting is the detection of expired carbon dioxide (CO2).4 We hypothesised that residual CO2 in cadaveric lung would be detectable using standard clinical monitoring systems, facilitating detection of tracheal tube placement and further enhancing the fidelity of clinical simulation using a cadaveric model.
Methods
After obtaining the appropriate legal and ethical authorisations, two fresh frozen unembalmed cadavers were sourced from a licensed Australian university anatomy facility and used for the purpose of emergency medical training as part of a procedural skills workshop for prehospital and retrieval medicine physicians. Cadaver one was a man in his eighties who had died 15 days previously. The body was frozen 5 days after death and first thawed 4 days prior to study. Cadaver two was a woman in her eighties who had died 11 days previously. The body was frozen 5 days after death and first thawed 4 days prior to study.
Tracheal intubation via direct laryngoscopy was undertaken as the initial procedural intervention on both cadavers. Definitive intratracheal placement was confirmed by direct observation of bilateral lung inflation after clamshell thoracotomy, a scheduled component of the educational workshop conducted subsequent to the intubations. No artificial ventilation was provided prior to intubation.
Cadaver one was intubated on first pass with an 8.0 mm internal diameter cuffed orotracheal tube to a depth of 22 cm at the teeth and cuff inflated with 5 mL air. Cadaver two was intubated on first pass with a 7.0 mm internal diameter cuffed orotracheal tube to a depth of 21 cm at the teeth and cuff inflated with 5 mL air.
Each tracheal tube was connected to a self-inflating bag (Disposable Manual Resuscitator, Mayo Healthcare Pty Ltd, Sydney Australia), with a LIFEPAK 15 (Physio-control, Redmond, Washington USA) sidestream CO2 detector. The capnograph display was observed and recorded in high-definition video using an iPhone 4S (Apple Inc, Cupertino, California USA). The cadavers were hand-ventilated with room air until the capnometer reached zero or the waveform approached baseline.
Results
A clear capnographic waveform was produced in both cadavers. It was visible after the third expiration in cadaver one and the first expiration in cadaver two, approximating the appearances found in the clinical setting.
The waveform from cadaver one had a flat alveolar plateau and normal morphology comparable to that found in a live patient with non-obstructed airways (figure 1). A consistent waveform was produced at least until recording ceased at 106 s postintubation, at which time, the end-tidal carbon dioxide (ETCO2) was measured at 5.5 kPa (42 mm Hg). Maximal ETCO2 was 8.5 kPa (65 mm Hg), recorded 56 s postintubation.

Normal capnographic morphology with flat alveolar plateau comparable to the live patient with non-obstructed airways (cadaver one, 55 s postintubation).
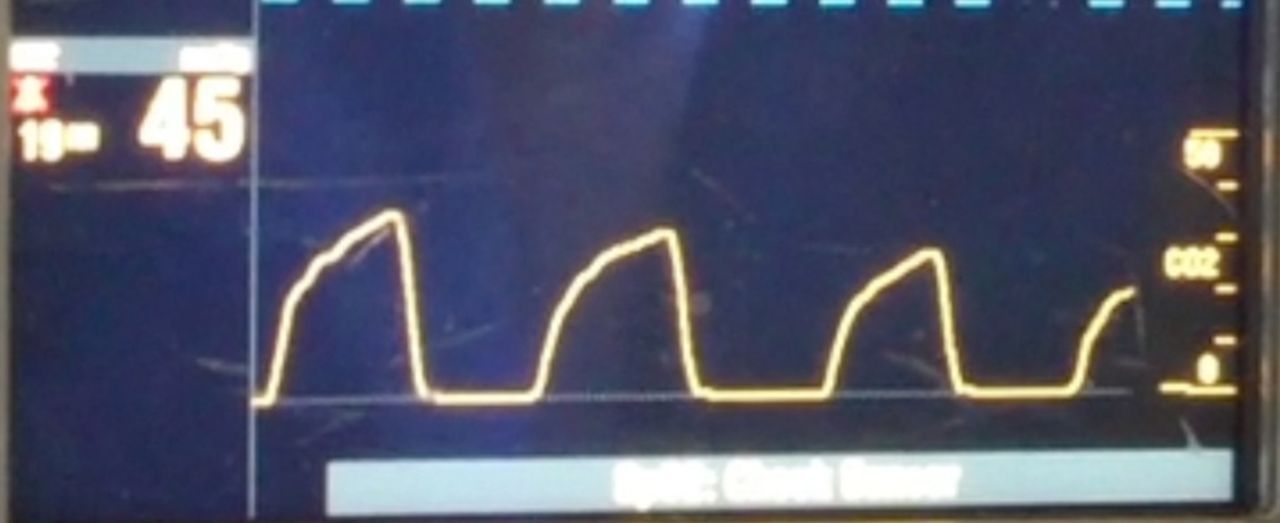
The waveform from cadaver two had an upsloping expiratory phase, similar to that found in patients with airways obstruction (figure 2). This persisted until recording ceased at 56 s postintubation, when ETCO2 was measured at 1.9 kPa (13 mm Hg). Maximal ETCO2 was 5.9 kPa (45 mm Hg), which was the initial postintubation ETCO2.
{kind=link}
{kind=link}
Upsloping capnographic morphology comparable typical of an obstructive pattern (cadaver two, 16 s postintubation).
The partial pressures of carbon dioxide and duration of detectable capnography until cessation of recording are detailed in table 1.
Partial pressures of expired carbon dioxide in fresh frozen cadavers extracted from video recording of waveform after tracheal intubation
Discussion
We believe this to be the first work to describe and quantify expiratory CO2 in ventilated human cadavers. Recently deceased unembalmed and fresh frozen cadavers provide high anatomical fidelity for airway training; the ability to apply the gold standard physiological monitor for tracheal tube placement might further enhance the use of cadavers in simulation training. Prior to its adoption, further research should confirm the absence of a sustained capnograph trace resulting from cadaveric oesophageal intubation. It is unknown whether ETCO2 would be detectable following intubation of cadavers that have been preserved using alternative methods. The source of CO2 in cadaveric lung remains to be elucidated: it is unclear whether it is physiologically produced during life and trapped within and by collapsed airway tissue, or whether it is released as a result of a postmortem process.
Conclusion
We have demonstrated that tracheal intubation of fresh frozen cadavers could be confirmed by life-like waveform capnography. This requires further validation in a larger sample size.
Footnotes
-
Contributors CR conceived and designed the study and drafted the initial manuscript. All other authors conducted the study and assisted with data collection, preparation and approval of the manuscript. All authors fulfil the criteria of authorship. There is no one else who fulfils the criteria who has not been included as an author.
-
Competing interests None.
-
Ethics approval University of Adelaide’s School of Medical Sciences.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Videos of the capnographic waveforms are available for viewing by contacting reidcg@me.com.