Article Text

Abstract
Objective The emergency department assessment of chest pain score accelerated diagnostic pathway (EDACS-ADP) facilitates low-risk ED chest pain patients early to outpatient investigation. We aimed to validate this rule in a North American population.
Methods We performed a retrospective validation of the EDACS-ADP using 763 chest pain patients who presented to St Paul's Hospital, Vancouver, Canada, between June 2000 and January 2003. Patients were classified as low risk if they had an EDACS <16, no new ischaemia on ECG and non-elevated serial 0-hour and 2-hour cardiac troponin concentrations. The primary outcome was the number of patients who had a predetermined major adverse cardiac event (MACE) at 30 days after presentation.
Results Of the 763 patients, 317 (41.6%) were classified as low risk by the EDACS-ADP. The sensitivity, specificity, negative predictive value and positive predictive value of the EDACS-ADP for 30-day MACE were 100% (95% CI 94.2% to 100%), 46.4% (95% CI 42.6% to 50.2%), 100% (95% CI 98.5% to 100.0%) and 17.5% (95% CI 14.1% to 21.3%), respectively.
Conclusions This study validated the EDACS-ADP in a novel context and supports its safe use in a North American population. It confirms that EDACS-ADP can facilitate progression to early outpatient investigation in up to 40% of ED chest pain patients within 2 hours.
- acute coronary syndrome
- effectiveness
- risk management
- statistics
Statistics from Altmetric.com
Key messages
What is already known on this subject?
There has been a rising interest in the development of accelerated diagnostic protocols for low-risk chest pain in the ED, with numerous clinical decision instruments (such as the emergency department assessment of chest pain score accelerated diagnostic pathway (EDACS-ADP)) being published in recent years. These protocols need to be validated in other populations and clinical settings before they can be broadly adopted.
What might this study add?
This study validates the EDACS-ADP in a different population and clinical setting from where it was derived. This provides useful information on how generalisable this protocol is to a new population and will inform clinicians as to whether this protocol may be safely applied in their own clinical setting.
Introduction
ECG and cardiac troponin (cTn) are the principal tests used to assess patients who present to EDs with symptoms of heart disease. However, these tests may not safely rule out acute coronary syndrome (ACS) on their own.1 ,2 Risk stratification tools are typically clinical decision aids that incorporate patient symptoms, clinical history and examination findings into a numerical score that categorises a patient's pre-test likelihood of having a disease. These tools, used in conjunction with ECG and cTn, such as the thrombolysis in myocardial infarction (TIMI) score incorporated into the accelerated diagnostic protocol using troponin as the only biomarker (ADAPT) pathway,2 can provide safe discharge for a small proportion of patients identified as low risk.1–6 New risk stratification tools are needed that will safely identify a larger subset of chest pain patients who may be discharged earlier from the ED. The broad adoption of such a tool could reduce ED overcrowding and improve the efficiency of ACS diagnostic processes. However, while many tools have been created, few tools have been incorporated into clinical practice, with many having limited applicability because of unsatisfactory performance, poor usability or a reluctance of health professionals to use them.3 ,4
The Vancouver Chest Pain Rule was derived using risk factors, pain characteristics, ECG findings and cardiac biomarkers to assist clinicians with this task.5 The recently derived emergency department assessment of chest pain score accelerated diagnostic protocol (EDACS-ADP)6 uses similar clinical features with ECG and cTn as the only biomarker. In the Australasian derivation and validation cohorts, the EDACS-ADP classified more patients at low risk of major adverse cardiac events (MACEs) with higher sensitivity and specificity than the Vancouver Chest Pain Rule.5
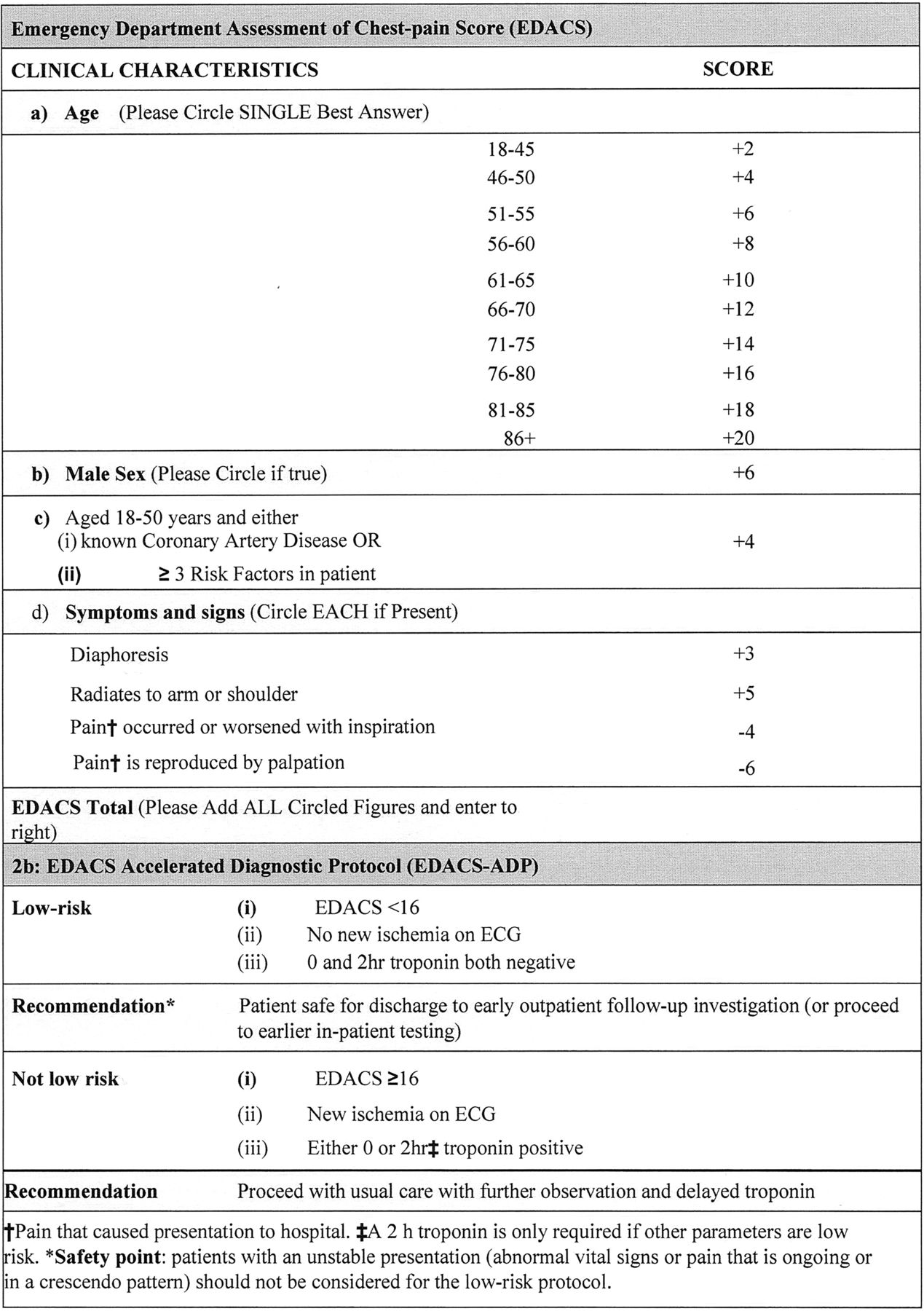
The EDACS-ADP6 generates a score from clinical features to identify a subgroup of ED chest pain patients who are at low risk of MACEs (figure 1). The score ranges from −10 to 34, with higher values representing higher risk. When combined with ECG and cTn results, this score forms part of an accelerated diagnostic protocol (EDACS-ADP).6 The EDACS-ADP classifies chest pain patients as low risk of 30-day MACE if they are stable on arrival, have EDACS<16, have ECGs without new ischaemia on arrival and have negative cTn concentrations at 0 and 2 hours after arrival. The rule was shown to identify up to 50% of patients who presented with suspected cardiac chest pain as low risk with the potential to be safely discharged from the ED within 2 hours with a negative predictive value (NPV) of 99.7%.6 However, the validation cohort was recruited in the same Australasian centres as the derivation cohort, which potentially limits its general applicability.

Emergency department assessment of chest pain score (EDACS).5
There is a need to validate accelerated diagnostic protocols in a variety of patient groups and clinical settings before broad adoption.7 This study assessed the performance of EDACS-ADP in the Canadian Vancouver Chest Pain Rule cohort with the aim of gaining further insight into the applicability of the decision aid in different clinical settings.
Materials and methods
Study design and setting
This study retrospectively applied the EDACS-ADP to a prospectively recruited cohort of patients from Vancouver, Canada. The cohort was primarily recruited in 2000–2003 to derive the Vancouver Chest Pain Rule.5 It was selected to validate the EDACS-ADP because the data were collected specifically for the purpose of identifying a low-risk group of chest pain presentations in an ED, with all the data points necessary to calculate the EDACS. As such, while this is a retrospective analysis, all data were collected prospectively. Full details of the methods of data collection, participant recruitment and follow-up of that study have previously been published,5 but are summarised below. That study was approved by The Providence Health Care Research Ethics Board.5 Funding organisations and sponsors of the current project had no role in data interpretation and reporting.
Study population
Consecutive adult participants were prospectively recruited from St. Paul's Hospital (an urban, tertiary centre in British Columbia, Canada) between June 2000 and January 2003. During the study period, the ED received 45 000 patients annually and the hospital had a full cardiology service, including a coronary care unit, 24-hour cardiac catheterisation laboratory and cardiac surgery with transplant capabilities. To be eligible for the study, participants had to present with anterior or lateral chest pain. Research assistants obtained consent from eligible patients between 07:00 and 22:00, 7 days per week. Patients were excluded if they were younger than 25 years, had clear traumatic or radiologically evident non-cardiac aetiology for their symptoms, had a terminal non-cardiac illness, had difficulty in communication, did not have a fixed address or telephone number in British Columbia for follow-up or had already been enrolled in the study in the past 30 days.
Study protocol
Data were collected by research assistants on standardised study forms and entered into a database.5 Patients were managed according to local guidelines, and treating clinicians were blinded to all study data.8 Clinical data, including chest pain characteristics, cardiac risk factors and medical history, were documented, and ECGs and blood for cardiac troponin T (cTnT) (Roche Elecsys 3rd generation Troponin T assay, Hoffman LaRoche, Laval, Quebec, Canada) analysis were taken 0 and 2 hours from presentation. A serum cTnT ≥0.04 µg/L was reported as abnormal (internal document—St Paul's Hospital Laboratory Medicine Bulletin regarding ‘change to troponin method’—26 March 2002). Research assistants were blinded to patient outcomes. ECGs were interpreted by staff emergency physicians according to prespecified criteria, described in the ‘Data analysis’ section. These staff physicians were blinded to all other predictor variables and blinded to 30-day outcomes as well. The information documented by research assistants was not used in patient management.
The data5 used in the current study were collected before the EDACS-ADP was derived. Consequently, family history of coronary artery disease was recorded or interpreted differently to the derivation study. This was recorded as ‘parent or sibling <65 years of age with heart attack’ compared with ‘parent sibling or child who suffered angina heart attack or death at <50 years of age’ in the original study.
MACEs were determined by emergency physician researchers who were blinded to all predictor variables, according to key outcome measures described below. After discharge, research assistants telephoned patients to identify any further hospital visits. Details of all investigations that occurred within 30 days of presentation were noted. Clinicians who had treated patients in the follow-up period were contacted to fill out a structured sheet containing all predictor variables. Study nurses contacted family physicians to ensure all presentations, and investigations performed over the 30-day follow-up period were included in the final diagnosis.
Data analysis
In 2013, data were extracted and analysed to categorise patients using the EDACS-ADP. The EDACS (score) was calculated by researchers who had not been involved in data collection or patient management. Patients were classified as low risk if they had all of the following: (i) an EDACS <16, (ii) troponin results ≤0.04 µg/L at 0 and 2 hours and (iii) an ECG with no evidence of new ischaemia. Cardiac ischaemia not known to be old on the ECG was considered present if there were any of the following changes that were not pre-existing from any available previous ECG(s):9 (i) ST-segment depression of at least 0.5 mm (0.05 mV) in two or more contiguous leads (includes reciprocal changes); (ii) T-wave inversion of at least 1 mm (0.1 mV) including inverted T-waves that are not indicative of acute myocardial infarction (AMI); or (iii) Q-waves >30 ms in duration or (iv) new, or presumed new, ST-segment elevation at the J-point in two or more contiguous leads, with the cut-off points ≥0.2 mV in leads V1, V2 or V3, or ≥0.1 mV in other leads; or (v) new left bundle branch block.8 If no previous ECG(s) were available, any abnormalities were considered to be new. Additionally, sentinel findings indicative of potential clinical instability were described as ‘red flags’. These were either (i) chest discomfort (thought to be possibly cardiac in origin), which was ongoing or in a crescendo pattern, or (ii) the presence of abnormal vital signs (such as systolic BP <100 or heart rate <50 or >100, RR >20, oxygen saturation <95% of room air). The presence of a ‘red flag’ meant that patients were classified as not low risk irrespective of the other EDACS parameters.
In keeping with the methodology used in the derivation of the EDACS-ADP,6 if a variable was missing it was considered normal or negative. In this way, the sensitivity was the lowest that could be yielded from the data, which helped ensure the safety of the rule. If any missing variables were abnormal or positive, it would increase the sensitivity and decrease the specificity of the ADP.
Patient characteristics were presented as categorical (with numbers and percentages) or continuous data (with means with SDs or medians with IQRs). The performance of the EDACS-ADP to predict MACEs was assessed by calculating sensitivity, specificity, positive predictive value (PPV) and NPV. Positive and negative likelihood ratios were also calculated. The software package used was Medcalc (Medcalc Software V.11.1.1.0, member of the American Statistical Association. http://www.medcalc.com).
Key outcome measures
The primary outcome was a MACE occurring either on initial hospital attendance or within 30 days of presentation.9 Prespecified MACEs were defined according to predefined criteria9 ,10 and included any of the following: non-ST-elevation myocardial infarction, ST-elevation myocardial infarction, emergency revascularisation, cardiovascular death, cardiac arrest, cardiogenic shock or high atrioventricular block.9 As the third definition of AMI had not yet been published in 2003, AMI was assigned by blinded investigators, according to a predefined criteria, which has since been published in the Annals of Emergency Medicine11 (see online supplementary data 1). In circumstances where the diagnosis was unclear, the case was independently adjudicated by a cardiologist blinded to predictor variables, according to the same criteria. The participant list was cross-referenced against the British Columbia Death Registry to check for deaths. Detailed descriptions of how these end points were defined have been previously published.9
Supplemental material
Results
Characteristics of patients
From the original patient cohort, 819 patients were included. Of these, 37 patients were excluded from analysis and 19 lost to follow-up (figure 2). None of the patients lost to follow-up were recorded in the death registry or re-presented to a regional ED within the next 30 days. The remaining 763 participants were predominantly male, many with a history of smoking, hypertension or dyslipidemia (table 1). Almost half the participants who were ADP positive had hypertension and/or had a past myocardial infarction. There were 76 (10.0%) AMIs during the index admission. Within 30 days of discharge from the ED, a further three (0.4%) patients had a MACE. Overall, 79 participants (10.4%) had a MACE (table 1).
Characteristic of patients

{kind=link}
{kind=link}
Study flow diagram. ADP, accelerated diagnostic pathway; AMI, acute myocardial infarction; MACE, major adverse cardiac event.
Outcome of EDACS-ADP
Of the 763 participants, the EDACS-ADP classified 317 participants (41.6%) as negative for AMI during the incident admission (table 2), with an optimum sensitivity of 100.0% (95% CI 94.0 to 100.0) and NPV of 100.0% (95% CI 98.5 to 100.0) (table 3). Of the patients who did not have an incident AMI, a total of 438 (57.4%) had EDACS <16 (table 4). Of the 317 classified as low risk during the index admission, none experienced a new MACE within 30 days (table 4) demonstrating optimum sensitivity of 100.0% (95% CI 38.0 to 100.0) and NPV of 100.0% (95% CI 98.5 to 100.0) (table 5). The EDACS for the composite outcome of 30-day MACE including incident AMI was similar to that for the incident AMI group (415 vs 416) and the numbers predicted as low risk using the ADP remained the same (table 6) with high diagnostic performance criteria yielding a sensitivity of 100.0% (95% CI 94.22 to 100.0) and NPV of 100.0% (95.51 to 100.0) (table 7).
Performance of emergency department assessment of chest pain score accelerated diagnostic pathway (EDACS-ADP) components for diagnosis of incident acute myocardial infarction (AMI) during initial hospital attendance
Test characteristics of emergency department assessment of chest pain score accelerated diagnostic pathway (EDACS-ADP) components for diagnosis of incident acute myocardial infarction (AMI) during initial hospital attendance
Performance of emergency department assessment of chest pain score accelerated diagnostic pathway (EDACS-ADP) components to predict 30-day major adverse cardiac event (MACE) in patients (excluding incident acute myocardial infarction (AMI) during initial hospital attendance)
Test characteristics of emergency department assessment of chest pain score accelerated diagnostic pathway (EDACS-ADP) components to predict 30-day major adverse cardiac event (MACE) in patients (excluding incident acute myocardial infarction (AMI) during initial hospital attendance)
Performance of emergency department assessment of chest pain score accelerated diagnostic (EDACS-ADP) components for composite outcome of overall 30-day major adverse cardiac event (MACE) including incident acute myocardial infarction (AMI) (during initial hospital attendance)
Test characteristics of emergency department assessment of chest pain score accelerated diagnostic pathway (EDACS-ADP) components for composite outcome of overall 30-day major adverse cardiac event (MACE) including incident acute myocardial infarction (AMI) (during initial hospital attendance)
Discussion
This study determined that the EDACS-ADP can be safely and effectively applied in a population distinct from where it was derived. The EDACS-ADP had higher sensitivity and NPV in this Canadian population than the Australasian validation study. The ADP has an appropriate safety level for the identification of low-risk patients presenting to the ED with symptoms of possible ACS, which is in keeping with reported ED physicians' acceptable risk thresholds for such events.12 Our findings should assist clinicians by confirming that low-risk chest pain patients may be safely discharged from EDs for further outpatient management within 2 hours. The patients in this study were recruited before the EDACS-ADP was derived, in a different demographic setting, with a different prevalence of 30-day MACE (∼10% in North America5 vs ∼15% in Australasia6) and in different healthcare systems. The similarity in the performance of the EDACS-ADP in both populations implies a robustness of the score and ADP, and supports the assertion that the EDACS-ADP may be applied to other ED populations internationally to assist clinicians in risk-stratifying chest pain presentations.
The proportion of ED patients classified as low risk by the EDACS-ADP in this study (41.5%) and the derivation cohort (45%)6 is similar to that found by the ADAPT rule using a highly sensitive troponin I assay13 and significantly higher than other reported risk stratification tools (9.8% and 25.7%).1 ,2 ,5 ,13–15 The EDACS-ADP has therefore been verified to identify a large population eligible for decision-making for early rule out of MACE without compromising safety and may reduce hospital and ED overcrowding.
This study provided an opportunity for a closer comparison of the EDACS-ADP and the Vancouver Chest Pain Rule. However, the Vancouver Chest Pain Rule aims to identify patients without ACS who require no further investigation,5 whereas the EDACS-ADP aims to identify patients at low risk of MACE who can return for outpatient investigations. These two rules cannot therefore be subjected to direct comparison, but the potential impact on patient flow and overcrowding can be considered. The Vancouver Chest Pain Rule was 98.8% sensitive and 32.5% specific for ACS,5 allowing 25.7% of patients with chest pain to be discharged at 2 hours without any follow-up, and it has been postulated that if the Vancouver Chest Pain Rule identifies one-fifth of the cohort as safe for early discharge, this would permit the safe early discharge of 120 000 chest pain presentations across Canada annually.16 In comparison, the EDACS-ADP categorised 41.5% of chest pain presentations into a low-risk group, eligible for outpatient testing. Extrapolating on the figures from Scheuermeyer et al,16 the EDACS-ADP could facilitate the early discharge of 252 000 patients across Canada annually, but would require these patients to return to the hospital for further investigations.
There is concern that the analytical performance of different generation troponin assays may affect the performance of risk stratification processes.17 In particular, introducing high-sensitivity cTn assays might alter the diagnostic accuracy of existing rules.13 However, prior research has shown that the diagnostic performance of the EDACS-ADP is unlikely to be affected by using a different sensitive troponin assay than that used in the original derivation and validation study.2 ,13 Both Australasian and Canadian validation studies of the ADAPT-ADP reported similar diagnostic accuracy for high-sensitivity TnI and sensitive TnI results.2 ,13 Since the EDACS-ADP's performance was not affected by the use of another sensitive troponin assay, it can be assumed that the EDACS-ADP may perform equally well with different assays.
The EDACS-ADP is one of the approaches recommended by the New Zealand Ministry of Health for the assessment of chest pain in EDs and has now been adopted in 23/26 district health boards into routine clinical practice. It is also in use in a number of large health systems in Australia.
Limitations
Our study had several limitations. Data for this validation were collected several years before the data definitions upon which the EDACS-ADP derivation study was created. It is uncertain how this could have biased the results of this analysis. Areas of change over this time period include the publication of the third universal definition of myocardial infarction,10 how emergency physicians approach patients with chest pain, what proportion of patients undergo cardiac evaluations, how patients are referred for additional testing, the use of non-invasive imaging prior to invasive angiography and perceptions of the benefit from revascularisation procedures. These items could have had an uncertain effect on rule performance, the selection of the study cohort and the outcomes of the cohort. It should also be noted that the cTnT assays in use at the host institution at the time of patient recruitment are now old relative to currently available troponin assays. This is important because troponin forms part of both the index test and the reference standard. This could potentially lead to both an underestimation or overestimation of the sensitivity. It is reassuring that no patients in the low-risk group were identified as having had MACE within 30 days or were present in the British Columbia Death Registry, but it is still recommended that further contemporaneous validation be conducted. In this population, the EDACS-ADP had a false positive rate of 53.7% and therefore the EDACS-ADP should be used as a screening process for ‘rule out’ with non-low-risk (‘positive’) patients proceeding to usual investigations. It is also important to note that almost all of MACEs occurred within the index presentation. Since there were only three MACEs during subsequent 30-day follow-up, the sensitivity and specificity have wide CIs such that their calculation may not be meaningful for this follow-up phase.
The performance of the ADP could vary in other settings. Patients recruited into this study were required to have chest pain, so the findings cannot be extrapolated to patients with atypical symptoms such as weakness, nausea or dyspnoea. Patients who were discharged from the ED were not required to have follow-up biomarker testing or mandatory provocative cardiac testing, although approximately 40% of the study cohort did have these investigations. It is therefore possible that clinically silent ACS events were unreported. It is also possible that outcome events were modified in those patients who had additional testing. The EDACS-ADP cannot be used for the exclusion of rare, but potentially lethal causes of chest pain, such as aortic dissection or pulmonary embolism, as they were not assessed in this study.
Conclusion
In this study performed in Canada, we retrospectively applied the EDACS-ADP and found that a large proportion of ED chest pain patients with possible ACS were correctly classified as low risk for 30-day MACE. The EDACS-ADP could facilitate early discharge of such patients into an outpatient setting.
Acknowledgments
The authors thank Dr William Parsonage and Professor Richard Troughton, who assisted with data analysis and manuscript review, and Associate Professor John Pickering, who also assisted with manuscript review.
References
Footnotes
Additional material is published online only. To view please visit the journal online (http://dx.doi.org/10.1136/emermed-2015-205028)
Contributors DF: design, data analysis, result interpretation, manuscript write up, review and submission. MT and LC: design, result interpretation, manuscript write up and review. FXS, JC and BB: design, data collection, result interpretation, manuscript write up and review. JG, SA, CJH and JP: result interpretation, and manuscript review. JD: result interpretation, manuscript write-up and review.
Funding The research was supported by the AusHSI PhD Scholarship. The paper development was supported by the Emergency Care Foundation, Christchurch, New Zealand.
Competing interests DF, MT, LC, SA, JG and JD were involved in the derivation of the EDACS-ADP. DF received funding from AusHSI for travel costs, accommodation and equipment used in this research PHD000493.
Ethics approval The Providence Health Care Research Ethics Board P98-0133.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional variables collected from participants, not relevant to the current study, are available by contacting the corresponding author.