Article Text

Abstract
Introduction A key principle in the effective management of major incidents is triage, the process of prioritising patients on the basis of their clinical acuity. In many countries including the UK, a two-stage approach to triage is practised, with primary triage at the scene followed by a more detailed assessment using a secondary triage process, the Triage Sort. To date, no studies have analysed the performance of the Triage Sort in the civilian setting. The primary aim of this study was to determine the performance of the Triage Sort at predicting the need for life-saving intervention (LSI).
Methods Using the Trauma Audit Research Network (TARN) database for all adult patients (>18 years) between 2006 and 2014, we determined which patients received one or more LSIs using a previously defined list. The first recorded hospital physiology was used to categorise patient priority using the Triage Sort, National Ambulance Resilience Unit (NARU) Sieve and the Modified Physiological Triage Tool-24 (MPTT-24). Performance characteristics were evaluated using sensitivity and specificity with statistical analysis using a McNemar’s test.
Results 127 233patients (58.1%) had complete data and were included: 55.6% men, aged 61.4 (IQR 43.1–80.0 years), ISS 9 (IQR 9–16), with 24 791 (19.5%) receiving at least one LSI (priority 1). The Triage Sort demonstrated the lowest accuracy of all triage tools at identifying the need for LSI (sensitivity 15.7% (95% CI 15.2 to 16.2) correlating with the highest rate of under-triage (84.3% (95% CI 83.8 to 84.8), but it had the greatest specificity (98.7% (95% CI 98.6 to 98.8).
Conclusion Within a civilian trauma registry population, the Triage Sort demonstrated the poorest performance at identifying patients in need of LSI. Its use as a secondary triage tool should be reviewed, with an urgent need for further research to determine the optimum method of secondary triage.
- major incidents, epidemiology
- prehospital care, major incident/planning
- triage
Statistics from Altmetric.com
Key messages
What is already known on this subject
The key to success in major incident triage is identifying patients in need of life-saving interventions (LSIs). Currently, the UK and many other countries use a two-stage approach to major incident triage.
As a secondary triage process, the Triage Sort aims to refine the triage decisions previously made by primary triage tools. It has previously demonstrated good success at predicting mortality from injury.
However, in studies in the military environment, the Triage Sort has shown limited ability to predict the need for LSI.
What this study adds
Applying the Triage Sort retrospectively to a civilian trauma database (UK TARN), this study has demonstrated that the Triage Sort has poor sensitivity in identifying patients in need of LSI, and had lower sensitivity than two primary triage methods, the National Ambulance Resilience Unit (NARU) Sieve and the Modified Physiological Triage Tool-24 (MPTT-24).
Introduction
Major incidents occur worldwide on a regular basis; in 2017, the UK alone witnessed at least six major incidents, resulting in over 100 fatalities and >400 injured.1 2 Triage, the process of prioritising patients on the basis of their clinical acuity, is a key principle in their effective management.3 Taught in a number of countries worldwide, the Major Incident Medical Management and Support course delivers a two-stage approach to triage, with primary triage being conducted at the scene of the incident, followed by a secondary triage assessment, typically performed in a more permissive setting.4 5 In the UK, primary triage is currently conducted using the National Ambulance Resilience Unit (NARU) Sieve, followed by secondary triage using the Triage Sort. As the secondary triage process occurs within a more permissive setting, such as the Casualty Clearing Station, it is typically performed by a more experienced clinician.
At a major incident, it is generally agreed that for the clinician on the ground, identifying those patients in need of a life-saving intervention (LSI) is the most important metric as it reflects actual patient acuity rather than mortality prediction and Injury Severity Score (ISS).6–8 Such patients should be identified as priority 1 using the triage tool. A number of studies have demonstrated that existing methods of primary triage (START, Careflight, Triage Sieve and NARU Sieve) have poor performance at identifying patients in need of LSIs, with sensitivities as low as 20% in the civilian setting.7–10
A new triage tool, the Modified Physiological Triage Tool-24 (MPTT-24), has recently been developed. Designed specifically to identify patients needing LSIs, the MPTT-24 consistently outperformed existing methods in both the military and civilian environments.11 Reflecting a change in practice, the MPTT-24 has recently been adopted by the Defence Medical Services for the purposes of primary triage and also the National Health Service (NHS) England 2018 Clinical Guidelines for Major Incidents.
As a secondary triage tool, the Triage Sort originated from the Triage Revised Trauma Score, developed in the 1980s as a field triage tool determining the need for major trauma centre care.12 While it has previously demonstrated extremely high sensitivity (>95%) at predicting those who die following trauma,13 in a more recent study looking at a prospective cohort of military patients, it was found to have limited accuracy when identifying patients in need of LSI.14 No similar studies have been conducted in the civilian setting.
The aim of this study was to determine the performance of the Triage Sort at predicting the need for LSIs within a civilian trauma registry setting. The secondary aim was to determine whether the secondary triage process conveys an improvement in performance over primary triage methods, by performing a comparative analysis with the existing UK civilian/military primary triage method, the NARU Sieve and the newly derived MPTT-24. A comparison of the three triage tools is provided in table 1.
Comparison of triage tools
Methods
A retrospective review of the Trauma Audit Research Network (TARN) database was conducted for all adult patients (aged >18 years), meeting TARN inclusion criteria and who presented to hospitals in England and Wales between 1 January 2006 and 31 December 2014. The largest trauma registry in Europe, TARN collects data from all trauma receiving hospitals in England and Wales on patients with moderate to severe traumatic injuries who are admitted to hospital for ≥3 days, admitted to a critical care unit or who die in hospital. Specific groups of patients with single injuries (such as a fractured hip) are excluded. Patients who are declared dead in the prehospital setting and not conveyed to hospital are not included. Data are collected by clerical staff from the receiving hospital and submitted electronically to TARN and include records across the whole patient pathway, from the point of injury through to discharge.
For this study, we reviewed the TARN database to identify patients who received one or more LSIs. These interventions were previously defined through a Delphi consensus of experts involved in the management of major incidents.3 As not all LSIs are recorded as specific variables on the TARN database, surrogates were required for a number of variables in order to conduct the analyses; these are provided in the online supplementary table 1.
Supplementary file 1
Using first recorded emergency department physiology (consistent with arrival at a medical treatment facility during a major incident), we applied the Triage Sort, the MPTT-24 and the NARU Sieve to determine the priority (priority 1 or not-priority 1) patients would have been assigned using that method. Outliers were defined in keeping with the MPTT derivation study (heart rate >170 beats per minute, respiratory rate >45 breaths per minute and systolic blood pressure >206 mm Hg) and were removed from the analysis.15
Only patients who were direct admissions from the scene of injury were included in the analysis, and those with incomplete or missing physiological data were excluded. Due to the nature of the TARN database, patients who were declared dead at the scene and those who were not conveyed to hospital for any reason were not included in the analysis. Patients were assumed to be non-ambulant due to the nature of the inclusion criteria of the TARN database.
Statistical analysis was performed using sensitivity and specificity, under-triage (1-sensitivity) and over-triage (1-positive predictive value).16 17 The primary aim was to compare the accuracy of the Triage Sort with both the NARU Sieve and the MPTT-24 in terms of identification of adult patients in need of LSIs. A statistically significant difference in performance was evaluated using a McNemar’s Χ2 test with a Bonferroni correction to reduce for Type 1 errors (α=0.05/3=0.0167).
Post hoc analysis
Previous TARN studies have demonstrated that the principle mechanism of injury is a fall from a low height.18 As this mechanism is unlikely to be observed at a major incident, a post hoc analysis was conducted with this cohort of patients removed. Simple descriptive demographics (age, ISS, gender, outcome and priority 1 status) are provided in table 5 and statistical analysis is provided in table 4.
Full test characteristics
Comparison of study characteristics between the entire study population and cohort of patients with low falls removed
Missing data
A comparison was made between patients with complete and missing physiological data to evaluate for any differences between the need for LSI, mortality and ISS.
Results
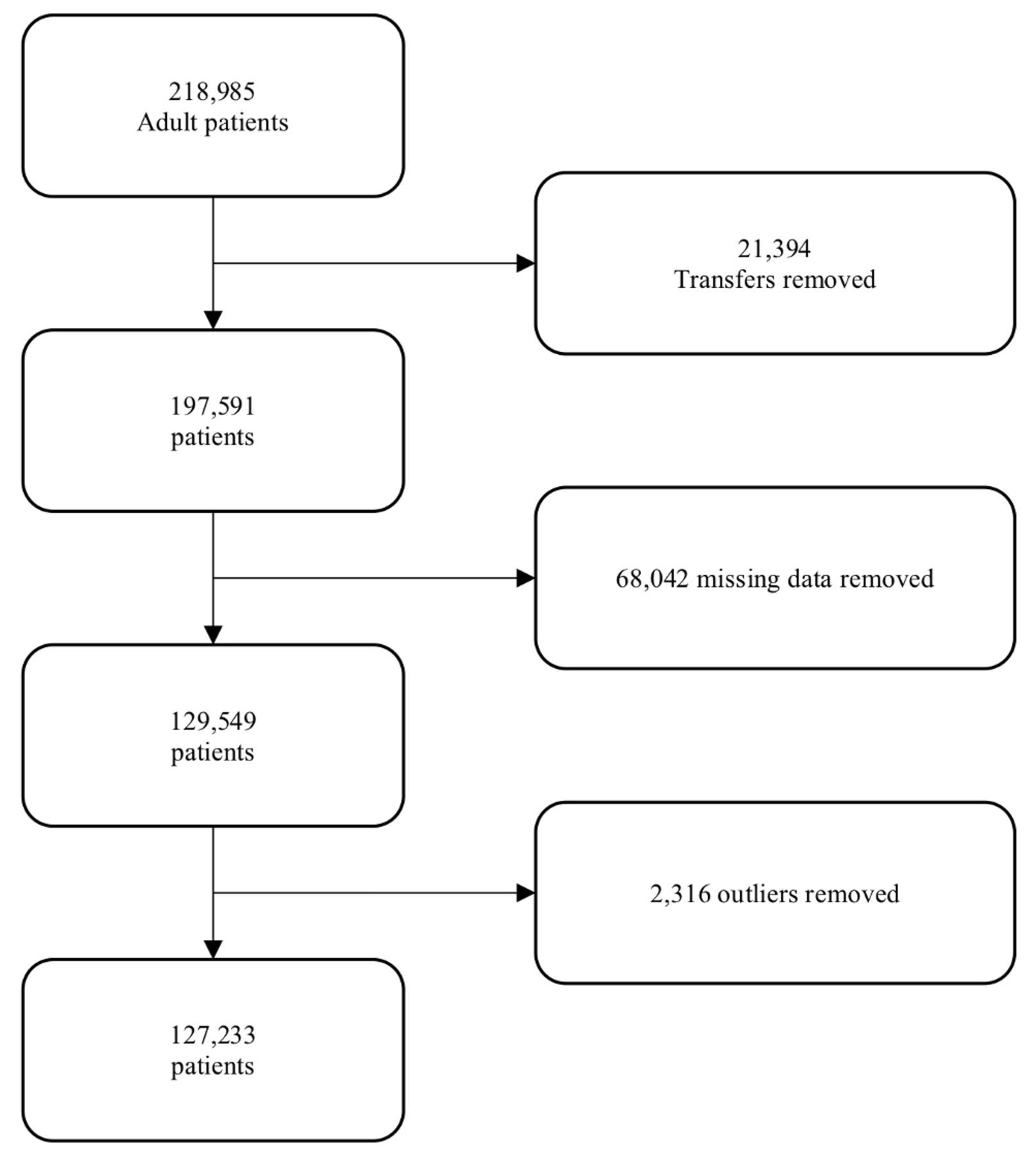
A total of 218 985 patients met TARN inclusion criteria during the study period and 127 233 were included in the final analysis (figure 1). 55.6% were men with a median age of 61.4 years (IQR 43.1–80.0) and a median ISS of 9 (IQR 9–16). The most common mechanism of injury was low falls (n=68 354, 53.7%) followed by road traffic collisions (n=27 915, 21.9%). 24 791 patients (19.5%) received at least one LSI and were therefore categorised priority 1; intubation and ventilation was the most frequently recorded LSI (n=8813, 24.8%). Overall 30-day mortality was 5.7% (n=7266). Full characteristics of the study population are provided in table 2.
{kind=link}
Participation flow diagram.
Characteristics of study population10
Of the three triage tools compared, the Triage Sort demonstrated the lowest sensitivity at identifying patients in need of LSI (15.9% [95% CI 15.5% to 16.4%]), and thus the highest rate of under-triage (84.1% [95% CI 83.6% to 84.5%]). However, the Triage Sort had the greatest specificity of all triage tools (98.6% [95% CI 98.6% to 98.7%]). A summary of triage tool performance is provided in table 3 with full test characteristics in table 4.
Summary of triage tool performance
In comparison, the NARU Sieve demonstrated comparable specificity to the Triage Sort (93.6% vs 98.6%), but with approximately twice the sensitivity at identifying the need for LSI (29.5% [95% CI 28.9% to 30.1%]). Of the three triage tools compared, the MPTT-24 demonstrated the greatest sensitivity at identifying the need for LSI (53.5% [95% CI 52.9% to 54.1%]), and thus had the lowest rate of under-triage (46.5% [95% CI 45.9% to 47.1%]). However, this was at the expense of the highest frequency of over-triage (66.0% [95% CI 65.7% to 66.3%]).
Using a McNemar Χ2 test with a Bonferroni correction (α=0.0167), a statistically significant difference in performance was observed between the MPTT-24 and Triage Sort (p<0.001; - χ2=33 056), the MPTT-24 and NARU Sieve (p<0.001, - χ2=25 145) and the NARU Sieve and the Triage Sort (p<0.001, - χ2=7580).
Subgroup analysis
A post hoc analysis was conducted excluding the cohort of patients who were injured as a result of low falls. A change in study demographics was observed (table 5), with a greater number of male patients (73.6%), that were younger (median 45.5 [IQR 29.9–61.5]) and requiring an increased number of LSIs (30.4%).
An improvement in sensitivity was observed for all three triage tools, with an absolute increase ranging from 1.4% (Triage Sort) to 3.8% (MPTT-24). However, this increase in sensitivity was associated with a reduction in specificity. Overall performance was unchanged with the MPTT-24 demonstrating the greatest sensitivity (57.3% [95% CI 56.5% to 58.0%]) at identifying patients in need of LSI and the Triage Sort,the lowest, see table 4.
Missing data
Mortality was significantly higher in the cohort of patients with missing data (10.1% vs 5.7%, p<0.001) and with a greater proportion of priority 1 patients (34.7% vs 19.5%, p<0.001). Additionally, there was a statistically significant difference between the two cohorts in terms of median ISS (10 [IQR 9–24] vs 9 [IQR 9–16]).
Discussion
In this study, we used a civilian trauma registry population as a surrogate for a major incident population and demonstrated that the existing method of UK secondary triage, the Triage Sort, has the poorest performance at identifying patients in need of LSI when compared with both the NARU Sieve and the MPTT-24. Designed to be a more detailed assessment, the Triage Sort includes an assessment of systolic blood pressure and the Glasgow Coma Scale. Not only do these assessments require training to be performed appropriately, but they also require equipment (for systolic blood pressure) and will result in a longer time required to triage when compared with simple primary methods.4 Our results suggest that this additional assessment, requiring more equipment and skilled personnel, does not achieve additional benefits.
A number of studies have compared the performance of existing primary triage tools at predicting need for LSIs, but for secondary triage, the literature is limited to a single, prospective military study.14 Within this setting, the Triage Sort was found to have a greater sensitivity for identifying need for LSI compared with our results here (58.6% [95% CI 51.8% to 65.4%]). Similar findings with primary triage tools have been documented previously, where performance is greater in a military rather than a civilian setting. This may be explained to a degree by the homogeneous nature of the population involved; young men with limited comorbidities injured predominately by blast and/or penetrating trauma. By comparison, the demographics of the civilian trauma population are more diverse; an older population (IQR 43.1–80.0 years) that has the potential to include multiple comorbidities and polypharmacy, injured by a completely different trauma mechanism.
While we report the ability of the physiological criteria within the Triage Sort to identify patients in need of LSI, we are unable to objectively determine the performance of the fourth assessment ‘upgrade at senior clinician’s discretion’. 4 Being a subjective assessment, we are unable to quantify the sensitivity of this aspect of the triage tool, and whether with this, the performance of the triage tool will in fact increase.
A number of studies have discussed the benefit of senior clinical decision-makers on the triage process. Reporting the Israeli experience, Ashkenazi et al described that when experienced trauma physicians conducted triage, they were able to identify less than 50% patients with severe injuries.19 Although the reference standard in this study was injury burden using the ISS rather than the need for LSI, it does question the benefit of the senior clinical decision-maker. However, in contrast, following the London 7/7 bombings, Aylwin et al reported that an increase in triage accuracy was observed at sites where experienced prehospital clinicians conducted triage, with approximately 50% lower rates of over-triage.20
In keeping with previous studies, the MPTT-24 outperformed both the NARU Sieve and the Triage Sort at predicting the need for LSIs.9 Even so, the MPTT-24 still had a high rate of under-triage. With the MPTT-24 being developed using logistic regression to determine the optimum thresholds for each of the physiological parameters in the triage tool, it is unlikely that manipulating these further will improve the MPTT-24’s performance. It is likely therefore that we have exhausted the contribution of simple physiological measures to triage patients and that further improvement will require the use of additional variables.15 Alternative assessments including the Shock Index have been suggested as a supplement to the triage process and their performance should be assessed in the civilian setting.14 Additional types of triage such as the assessment of anatomical injury and the mechanism of injury exist and are constituent parts of field triage algorithms to determine the need for individual trauma patients to be transferred to a major trauma centre.21 22 With secondary triage intended to take place in a more permissive environment, there is potential merit in these alternative methods of triage being considered for the major incident setting.
Limitations
A key limitation of this work is the use of a trauma database to perform a comparative analysis of major incident triage tools. We acknowledge that the mechanism of injury observed in the TARN database may not be entirely representative of that observed following a major incident. With the leading mechanism of injury on the TARN database being low falls, an additional post hoc analysis was conducted with this cohort removed in an attempt to mitigate this limitation. Ideally, these triage tools should be validated and analysed in the environment in which they are designed to function, but owing to the unpredictable nature of major incidents, this is largely impossible; therefore, surrogates such as trauma databases or series of consecutive trauma patients are often used instead.7 15 23
The presence of inclusion criteria to TARN represents an additional limitation of the use of trauma databases and is likely to result in the study population sustaining a higher mean ISS than the overall population following injury. While the proportion of patients not receiving a LSI in our study was 80.5%, it is expected that the true proportion in the actual population will be higher. The implication of this is that while we expect the sensitivities reported in our study to be accurate (severely injured patients requiring LSIs are likely to fulfil TARN inclusion criteria), caution is required when interpreting triage tool specificity; as not all minimally injured patients (those not requiring LSIs) are captured by the TARN database, we anticipate the actual specificity to be lower than that reported in this study.
Additionally, large numbers of patients were excluded due to incomplete physiological data being recorded. When those who were excluded due to missing data are compared with those who had complete data recorded, a significant difference is observed, with the ‘missing’ cohort having a tendency to be more severely injured and with a greater need for LSI. The removal of these patients has the potential to lead to systematic error and introduce bias into our analysis. While multiple imputation has previously been used as a method to generate missing data, owing to the number of patients with missing data (n=68 042) representing over half (53.5%) of the complete dataset (n=127 233), it was deemed to be inappropriate in this setting and was not performed.
Lastly, we acknowledge that as authors involved in the development of the MPTT-24, this may lead to intellectual bias in the assessment of other triage tools. However, we have attempted to minimise this risk by focussing on the performance of the Triage Sort, rather than a direct comparison with the MPTT-24.
Conclusion
The aim of the secondary triage process at a major incident is to refine the triage decisions made following the initial triage assessment. Using a civilian trauma database population as a surrogate for the major incident population, the Triage Sort fails to achieve this. An urgent review of the method utilised for secondary triage at major incidents is needed.
Acknowledgments
The authors thank Professor Fiona Lecky, Research Director and Antoinette Edwards, Chief Executive Officer, at Trauma Audit Research Network (TARN) for facilitating access to the TARN database.
References
Footnotes
Twitter @jamievassallo
Contributors JV: conceived the idea for the study, analysed, interpreted the data and drafted the first manuscript; takes responsibility for the manuscript as a guarantor. JS: responsible for revising it critically for important intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.