Article Text

Abstract
Introduction Tranexamic acid (TXA) reduces bleeding and mortality. Recent trials have demonstrated improved survival with shorter intervals to TXA administration. The aims of this service evaluation were to assess the interval from injury to TXA administration and describe the characteristics of patients who received TXA pre-hospital and in-hospital.
Methods We reviewed Trauma and Audit Research Network records and local trauma registries to identify patients of any age that received TXA at all London Major Trauma Centres and Queen’s Medical Centre, Nottingham, during 2017. We used the 2016 NICE Guidelines (NG39) which state that TXA should be given within 3 hours of injury.
Results We identified 1018 patients who received TXA, of whom 661 (65%) had sufficient data to assess the time from injury to TXA administration. The median interval was 74 min (IQR: 47–116). 92% of patients received TXA within 3 hours from injury, and 59% within 1 hour. Half of the patients (54%) received prehospital TXA. The median time to TXA administration when given prehospital was 51 min (IQR: 39–72), and 112 min (IQR: 84–160) if given in-hospital (p<0.001). In-hospital TXA patients had less haemodynamic derangement and lower base deficit on admission compared with patients given prehospital TXA.
Conclusion Prehospital administration of TXA is associated with a shorter interval from injury to drug delivery. Identifying a proportion of patients at risk of haemorrhage remains a challenge. However, further reinforcement is needed to empower pre-hospital clinicians to administer TXA to trauma patients without overt signs of shock.
- trauma centres
- multiple trauma
- tranexamic acid
- haemorrhage
- fibrinolysis
Statistics from Altmetric.com
Key messages
What is already known on this subject
Tranexamic acid (TXA) reduces bleeding and mortality after traumatic injury.
Recent large multicentre trials have demonstrated improved survival with shorter intervals to TXA administration.
Pre-hospital TXA could speed up the time to administration.
What this study adds
In this retrospective study of 661 major trauma patients, time from injury to TXA administration was halved if given before arrival in hospital.
Patients receiving in-hospital TXA had less overt haemodynamic instability than those who received it pre-hospital.
Introduction
Major trauma is the leading cause of death in under 45 year olds in the UK and bleeding accounts for 40% of all injury-related deaths.1 2 Tranexamic acid (TXA) inhibits fibrinolysis and has been shown to decrease both all-cause mortality and deaths due to bleeding in trauma patients.3 The CRASH-2 trial demonstrated improved survival when TXA was given within 3 hours from injury. Survival was greater in the group of patients who received TXA within 1 hour.4 The care of trauma patients has improved since the introduction of England’s regional Major Trauma Networks in 2010.5 6 A recent analysis of the Trauma and Audit Research Network (TARN) database demonstrated that prior to publication of the CRASH-2 study, almost no trauma patients received TXA. By 2016, 10% (4593) of all trauma patients submitted to TARN were given TXA.7 Within Trauma Networks, TXA is given to patients suspected, or known to have, haemorrhage according to NICE Clinical Guidelines on major trauma.8 The guidelines state that TXA should be given as soon as possible, within 3 hours from injury, when active bleeding in major trauma is suspected. An individual patient level meta-analysis of 40 138 bleeding patients enrolled in the CRASH-2 and WOMAN trials9 demonstrated a 70% survival improvement when TXA was given immediately after haemorrhage, with a 10% reduction in benefit every 15 min and no benefit at all after 3 hours.10
There is a proposal to change the timing threshold for TXA administration. Currently, a hospital is eligible to receive the National Health Service (NHS) Best Practice Tariff if a patient with bleeding, who subsequently receives a blood transfusion, is given TXA within 3 hours.11 Under the new proposal, patients will need to have TXA within 1 hour from injury. To achieve this shorter time interval, Major Trauma Networks must understand where improvements can be made, for example, maximising the administration of TXA in the pre-hospital setting for patients at risk of haemorrhage. The aims of this study were to quantify the time to TXA administration, assess the proportion of patients achieving both timing thresholds and explore causes of delayed administration. We hypothesised that the characteristics of patients who received prehospital TXA were different from those that received it in hospital.
Methods
This was a retrospective review of trauma admissions during 2017 who received intravenous TXA in the acute phase of care. Patients were admitted to one of five Major Trauma Centres (MTCs) in England, the four MTCs in London (The Royal London Hospital, St. George’s Hospital, St. Mary’s Hospital and King’s College Hospital) and Queen’s Medical Centre, Nottingham. These five sites were chosen as they are among the highest contributors to the TARN database.12 Each MTC is part of a Trauma Network which also contains a number of smaller hospitals designated as Trauma Units (TU). Severely injured trauma patients may be initially managed at a TU before transfer to an MTC and were included in this study. Several local ambulance services bring patients into the Trauma Networks. Authors at each site identified patients by searching both the MTC’s submissions to TARN and the MTC’s local trauma registry where available. Trauma patients of all ages are submitted to the TARN database if they have an injury which results in either a hospital admission of 3 days or longer, a critical care admission, transfer to a specialist centre or in-hospital death within 30 days. Patients with isolated femoral neck or single pubic ramus fracture who are older than 65 years and those with simple isolated injuries are excluded.13 Two of the MTCs maintain local trauma registries which prospectively record all trauma team activations.
All adult and paediatric trauma admissions during 2017 who received TXA following their injury were included. Patients were excluded if: TXA was administered in the context of a clinical trial, there was no documentation of the time of TXA administration, or both the time of injury and the 999 call were missing. If the time of injury was not reliably recorded, it was approximated using the time of the 999 call. A standardised data collection form was used at all sites. During the initial analysis, we noted a large proportion of missing data from the registries. Where registry data were incomplete, authors at each MTC manually searched the patients’ original medical records. Missing details were retrieved from the patients’ medical record only by authors at the MTC in which the patient was treated. Only deidentified data were collected centrally for analysis. As a retrospective service evaluation, NHS Health Research Authority ethical approval was not required. Investigators at each site registered the study with their local audit office.
Patients were analysed in two groups depending on the location of TXA administration, either prehospital or in-hospital. To assess the potential for confounding due to different patient characteristics, we performed a subgroup analysis on patients from one of the five sites. Additional data were available at this site to describe the patients’ injury severity, on-scene and admission physiology and length of stay.
We used the current NICE Guideline (NG39), ‘Major trauma: assessment and initial management’ as the standard to assess the time to TXA administration.8 These guidelines recommend:
Administer intravenous TXA as soon as possible in patients with major trauma and active or suspected active bleeding.
Do not use intravenous TXA more than 3 hours after injury in patients with major trauma unless there is evidence of hyperfibrinolysis.
We did not assess the appropriateness of TXA administration in this service evaluation.
Statistical analysis
Statistical analysis was performed using SPSS 24 (IBM, Armonk, New York, USA) and graphs were built with Prism 8 (GraphPad Software, San Diego, California, USA). Categorical variables are expressed as frequency and percentage and analysed with the χ² or Fisher’s exact test. The normality of continuous variables was assessed using Q-Q plots and the Shapiro-Wilk test. Non-normally distributed data remained as such even after logarithmic and square root transformations. Consequently, they are expressed as median and IQR and were analysed with the Mann-Whitney U-test. The OR was used to quantify the likelihood of receiving TXA within 3 hours and 1 hour from injury depending on the location of TXA administration. Tukey’s method was used to create boxplots. A complete case analysis was conducted.
Results
Total 1018 patients received TXA in 2017 across all five study sites, of whom 57 were excluded due to enrolment in the CRASH-3 trial. Following review of the patients notes, a further 300 were excluded due to missing timing of TXA administration (online supplementary table 1). This left 65% (661/1018) of the patients for analysis (figure 1A). Patients were predominantly male and young. Road traffic collisions and stabbings were the most common mechanisms of injury, followed by falls. One or more units of packed red blood cells was given within the first 24 hours from injury to 67% (262/390) of the patients (table 1).
Supplementary file 1
Patient characteristics according to the location of TXA administration

Flow diagram of (A) main analysis cohort and (B) supplemental analysis cohort. InH, in-hospital; PreH, prehospital; Suppl., supplemental; TXA, tranexamic acid.
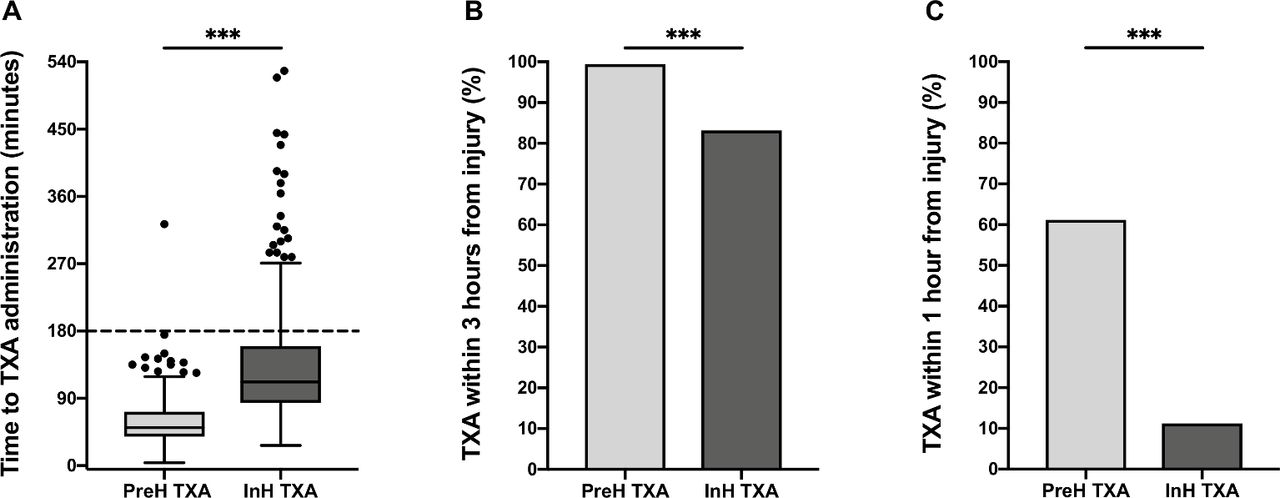
Of the 661 patients who were given TXA, 608 (92%) received it within 3 hours. The median time to TXA administration overall was 74 min (IQR: 47–116). There were 358 (54%) patients who received prehospital TXA. There was a significantly shorter median time from injury to TXA in the pre-hospital group of patients compared with the in-hospital group 51 min (IQR: 39–72) vs 112 min (IQR: 84–160), p<0.001 (figure 2A). Patients who received prehospital TXA had a higher probability of meeting the 3 hour target (figure 2B), OR=36.02 (95% CI 8.69 to 149.33), and the 1 hour target (figure 2C), OR=12.47 (95% CI 8.23 to 18.88).
{kind=link}
{kind=link}
(A) Interval to TXA administration. (B) Proportion of cases meeting the current 3 hour target. (C) Proportion of cases meeting the proposed 1 hour target. (A) Horizontal dashed line represents the current 3 hour TXA target interval. There are four additional outliers: one prehospital at 608 min and three in-hospital at 808, 885 and 1155 min. Time to TXA administration: pre-hospital, 51 min (IQR: 39–72); in-hospital, 112 min (IQR: 84–160). InH, in— hospital; PreH, pre-hospital; TXA, tranexamic acid.
Patients who received pre-hospital TXA were more likely to be treated by physician-led crews (60.5% vs 31.6%, p<0.001). However, there was no difference in overall mortality or in the proportion of patients who received a blood transfusion (table 1). To explore potential confounders, we analysed more detailed patient data which was available from patients at site 1 (figure 1B). Patients at site 1 who received pre-hospital TXA had evidence of early haemodynamic instability; heart rate on scene: 109 bpm (IQR: 83–130) vs 99 bpm (IQR: 74–120), p=0.062; systolic blood pressure on scene: 106 mm Hg (IQR: 89–33) vs 123 mm Hg (IQR: 92–141), p=0.079. On admission to hospital, patients in this group had a higher base deficit: 7.1 mEq/L (IQR: 2.3–12.9) vs 2.5 mEq/L (IQR: −0.2–8.2), p=0.004). Transfusion requirements and clinical outcomes appeared similar between the two groups, although this analysis is underpowered (table 2).
Additional patient characteristics according to the location of TXA administration at Site 1 only
Of the 661 patients for whom we could calculate the interval to TXA administration, there were 53 patients (8%) who received TXA beyond 3 hours from injury. Documented reasons for this delay and the commonly associated factors were sought from the patients notes. In the absence of a documented reason for the delay, we classified the cause as ‘clinical oversight’. This occurred in 60% (32/53) of cases. We noted several commonly associated factors with delayed TXA administration; secondary transfer (22%), late Emergency Medical Services arrival (8%), late patient deterioration (4%), long extrication time (4%) and initial uncertainty around time of injury (2%).
Discussion
In this study of five Major Trauma Networks in 2017, we observed that 92% of injured patients given tranexamic acid received the medication in under 3 hours. Patients given pre-hospital TXA received it earlier than those given the medication in-hospital and had higher odds of receiving it within current and proposed guidelines. On average, the time taken for a patient to receive in-hospital TXA was double that of patients given pre-hospital TXA. From the results of robust level one evidence, it is clear that early TXA leads to improved survival in bleeding patients.10
Identifying patients at risk of bleeding can be challenging. In this study, we did not observe a difference in injury severity scores between patients that received prehospital and in-hospital TXA. Those patients who received pre-hospital TXA often had more overt haemodynamic instability, suggestive of bleeding. There were only minor differences in the proportion of transfused patients and in-hospital mortality between patients who received the drug in or before hospital. We acknowledge that this study is underpowered to detect significant differences in clinical outcomes. Nevertheless, the in-hospital TXA patients were still characterised by a high mortality and transfusion rates. Based on the evidence of large trials,10 these patients would possibly benefit from earlier TXA administration. Consequently, future research should focus on pre-hospital prediction strategies to identify patients that are at risk of haemorrhage and may benefit from early TXA.
The findings in the present study support recently published data from 2016. In a large TARN database study, 82% of patients given TXA received it within 3 hours from injury, and 30% of patients received TXA within 1 hour from injury. This TARN based analysis reported similar times to our present study with median time intervals of 49 min (IQR 33–72) and 111 min (IQR 77–162) for pre-hospital and in-hospital TXA administration.7 Our present study provides an additional perspective by starting to describe the proportions and characteristics of patients who receive TXA before and after admission.
NHS (England) has made timely and appropriate TXA administration a determinant of MTC remuneration.14 This service evaluation only assessed whether TXA was given in a timely nature and not whether it was appropriate to give it. Nonetheless, we suggest that the financial incentivisation of timely TXA administration contributes to the high overall 3 hour compliance rate observed. In other studies of TXA administration, a wide range of compliance is seen (26%–100%). Two of these studies were undertaken in single level-one trauma centres in France. The first reported a compliance of at least 81% (98/121) in a cohort of patients treated between 2010 and 2014,15 while the second, with data from 2013 to 2014, described a lower proportion of 26% (10/39).16 In a Canadian level-one trauma centre between 2012 and 2015, 76% (51/67) of patients received TXA within 3 hours.17 Finally, a 15-centre Japanese study reported that all the 281 patients that were treated with TXA in 2012 received it within 3 hours from injury.18 Reasons for difference in performance are not clear but can be presumed to be due to differences in system organisation, implementation of evidence-based guidelines and incentivisation. However, even within the high volume, mature NHS Major Trauma Networks examined in this study, rates of breach of the 3 hour guideline ranged from 2% to 15%. More than 50 patients had TXA beyond 3 hours from injury. Explicit causal analysis, including potential complications, was not possible in this study but it is worrisome that this degree of variation exists.
Initiatives aimed at shortening the interval from injury to TXA administration must encompass the different organisations responsible for care in the UK, including charitable prehospital air ambulances, Ambulance Trusts, MTCs and TUs. English MTCs and TUs, which accrue financial benefit from compliance with mandated trauma standards, do not have operational lines of control over the prehospital systems charged with enhanced delivery. An Ambulance Trust, for example, may service several MTCs. While the clinical argument for earlier administration is strong, the current model of financial incentivisation may not drive improvement as efficiently as desired. The proposed reduced timeline target may have the unintended consequence of increasing overtriage. Protocols must balance the rare risks of unnecessary administration of TXA (hypersensitivity reactions, cerebrovascular accident, myocardial infarction and pulmonary embolism)19 with the need to enable rapid administration. The potential for harm if TXA is given beyond 3 hours also requires increased educational emphasis.
This study shares limitations common with many retrospective studies.20 For example, some data were not captured and this may not be random.21 Despite searching patients’ original case notes, we were unable to find almost a third of the missing data (online supplementary figure 1). However, data capture and data accuracy were maximised by combining TARN data with data obtained from original medical records. This approach improves data fidelity over using registry data alone. In 232 patients (23% of the total study population), no time of TXA administration was available. There are two likely causes for this missing information: inadequate clinical documentation and missing documentation.
The five MTCs included in the study are high volume contributors to the TARN database and are likely to represent efficient systems. Although multiple prehospital ambulance trusts operate within these Trauma Networks, extrapolation outside of these Trauma Networks should be made with caution.
Conclusion
The location where TXA is given is a key determinant of when it is administered. Half of the patients received TXA in the prehospital phase of care and in-hospital TXA patients waited twice as long to receive TXA. Further reinforcement is needed to empower prehospital clinicians to identify and treat patients at significant risk of haemorrhage. It is these high-risk patients that are likely to benefit from early TXA administration.
Acknowledgments
We thank Dr Charles Prior, Dr J Um, Mr Adam McDonald, Ms Anita West, Ms Helen Olaniyi and Ms Ayesha Khalid for their assistance with data collection. We thank Dr Elaine Cole and Professors Ian Roberts and Karim Brohi for their insightful advice reviewing the manuscript.
Footnotes
Twitter @maxmarsden83
Contributors MERM and AR collected the data, analysed the data, wrote and edited the manuscript. CABD and TGDW conceived the study and were local leads registering the study and collecting data. WPB and SS were local leads registering the study and collecting data. RB contributed to data collection and manuscript preparation. NRMT edited the manuscript and provided critical review.
Funding AR was supported by a scholarship for high-quality postgraduate training from the Fondazione Cassa Rurale di Trento, Italy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.