Article Text

Abstract
Introduction Major trauma is the third leading cause of avoidable mortality in the UK. Defining which patients require care in a major trauma centre is a critical component of developing, evaluating and enhancing regional major trauma systems. Traditionally, trauma patients have been classified using the Injury Severity Score (ISS), but resource-based criteria have been proposed as an alternative. The aim of this study was to investigate the relationship between ISS and the use of life-saving interventions (LSI).
Methods Retrospective cohort study using the Trauma Audit Research Network database for all adult patients (aged ≥18 years) between 2006 and 2014. Patients were categorised as needing an LSI if they received one or more interventions from a previously defined list determined by expert consensus.
Results 193 290 patients met study inclusion criteria: 56.9% male, median age 60.0 years (IQR 41.2–78.8) and median ISS 9 (IQR 9–16). The most common mechanism of injury was falls <2 m (52.1%), followed by road traffic collisions (22.2%). 15.1% received one or more LSIs. The probability of a receiving an LSI increased with increasing ISS, but only a low to moderate correlation was evident (0.334, p<0.001). A clinically significant number of cases (5.3% and 7.6%) received an LSI despite having an ISS ≤8 or <15, respectively.
Conclusions A clinically significant number of adult trauma patients requiring LSIs have an ISS below the traditional definition of major trauma. The traditional definition should be reconsidered and either lowered, or an alternative metric should be used.
- trauma
- emergency care systems
- major trauma management
Statistics from Altmetric.com
Key messages
What is already known on this subject
Funding through the UK major trauma tariff is aligned with the Injury Severity Score (ISS) and whether a patient’s ISS is >9 or >15.
Previous studies have demonstrated that the ISS is closely linked to mortality, but little is known about its correlation with the resource needs of the major trauma patient.
What this study adds
The ISS has only low to moderate correlation with the need for life-saving intervention.
The number of life-saving interventions received by a patient is strongly correlated with mortality and increasing injury severity. The provision of a life-saving intervention appears therefore to be an important criterion in defining the need for major trauma centre care.
A clinically significant number of adult trauma patients requiring life-saving interventions have an ISS below the traditional definition of major trauma and below that which attracts funding through the UK major trauma tariffs.
Introduction
Major trauma is a major public health problem that represents the third leading cause of avoidable mortality in the UK. It is responsible for 3000 fatalities, 8000 patients with severe disabilities, £0.4 billion of immediate treatment National Health Service (NHS) costs and a £3.5 billion loss in economic output each year in England.1 In 2012, major trauma care in England was reconfigured with the introduction of regional networks, aiming to concentrate seriously injured patients in specialist major trauma centres (MTC).2 3 The bypass of non-specialist local hospitals (non-MTCs) with less experience, resources and expertise has been associated with improved patient outcomes.4
Defining which patients require care in an MTC is a critical component of developing, evaluating and enhancing regional major trauma systems.5 A valid reference standard for major trauma would inform the development and validation of triage tools; help assess the performance of trauma networks and mass casualty systems, determining whether the ‘right person is being treated in the right place at the right time’; and guide resource allocation. However, despite its importance there is no clear gold standard for defining which patients should receive MTC care.
Traditionally, trauma patients have been classified according to an assessment of anatomical injuries using the Abbreviated Injury Scale (AIS) and Injury Severity Score (ISS) with an ISS threshold of greater than 15 defining major trauma.6 7 While the ISS provides an overall estimate of injury severity, it has a number of limitations. Many different injury patterns, often with varying acuity and prognosis, can yield the same ISS. Its calculation is influenced by the extent of radiological investigation performed, potentially inflating apparent injury severity through detection of incidental findings, or underestimating severity if patients are not fully imaged.8–10 Furthermore, the ISS>15 threshold does not account for heterogeneity in intensity, urgency and complexity of treatments required for different injuries, the appropriateness of aggressive management in elderly or severely comorbid patients, or patient wishes and values.
Consequently, resource-based criteria have been proposed as an alternative to anatomical measures to define major trauma.11 A number of consensus-based definitions have been formulated focusing on identifying patients who need specialised trauma interventions that are unavailable in non-MTCs.12 13 These include a recent UK-developed reference standard comprising the essential life-saving interventions required during the definitive care phase of a major incident.14
The aim of this study was to investigate the relationship between ISS (the traditional anatomical criteria defining major trauma) and the use of life-saving interventions (resource-based criteria). Specific objectives were to describe the proportion of patients receiving life-saving interventions with different injury severity scores; to evaluate whether commonly used ISS thresholds (1–8, 9–15 and ≥16) reflect an increased use of specialised trauma resources and mortality; to compare patients identified as needing MTC care by receiving a life-saving intervention to those identified using increased ISS; and to determine if provision of life-saving interventions is associated with mortality and age.
Methods
A retrospective cohort study was conducted using data from the Trauma Audit Research Network (TARN) registry.
The TARN database has been described in detail previously.15 16 Briefly, injured patients of any age are enrolled from trauma-receiving hospitals who fulfil one of the following criteria: admission to a critical care area; transfer for specialist care; death; and hospital admission for >3 overnight stays. The following patients are excluded: patients admitted under care of a rehabilitation team only; and certain isolated injuries, for example, eye, skin, fractured neck of femur, pubic rami and closed limb fractures. Information is collated from patient records by local hospital data coordinators and entered into the registry via a web-based portal. After 2012, participation in TARN was mandatory for MTCs with reimbursement of a major trauma tariff for patients with an ISS ≥9 dependent on case submission. Submission of data for non-MTCs, and prior to 2012 for MTCs, was voluntary with no financial incentive for case ascertainment.
The current study included all adult patients (aged ≥18 years) meeting TARN inclusion criteria and directly admitted to hospitals in England and Wales between 2006 and 2014. The proportion of eligible trauma-receiving hospitals contributing data to TARN varied from 32% to 89% for each year during the study period. Children and adults undergoing secondary transfer from non-participating hospitals were excluded.
A data set of demographic, injury, management and outcome-related variables was extracted from the TARN registry for eligible cases. Patients were categorised as needing a life-saving intervention if they received one or more from a previously defined list of 32 interventions considered life-saving (online supplementary table 1 online supplementary file 1). This list was derived for the purposes of defining life-saving interventions during the definitive care phase of a major incident through an international Delphi consensus process at any time during their presentation.14 While not specific for determining the need for treatment at an MTC it was chosen for use in this study due to its derivation; a large number of participants across two countries from a variety of medical specialities, all routinely involved in the management of acute trauma patients.14 Not all interventions are recorded as discrete variables on the TARN database, therefore surrogates were used where necessary to represent the closest approximation to the specific variable (online supplementary table 2). Independent, trained TARN injury coders centrally graded individual injuries for each case according to the AIS dictionary criteria17 (AIS, 2005 revision) based on clinical, radiological and postmortem information, and a subsequent ISS was assigned. Only definite injuries were considered with possible, probable or suspected injuries excluded.
Supplemental material
Characteristics of patients with different injury severity
Analysis proceeded in six stages. First, the demographics and characteristics of the sample were examined using descriptive statistics. Second, the relationship between the probability of receiving a life-saving intervention and ISS was assessed. The proportion of patients receiving a life-saving intervention was plotted for each ISS along with the 95% Confidence Intervals (95% CIs), and Spearman’s coefficient was calculated to assess correlation. In order to explore for potential confounding by age, this second stage was repeated with the study population stratified into three age groups (young adult aged 18–39.9 years, middle aged 40–64.9 years and elderly aged 65+ years). Third, the study sample was categorised into subgroups according to ISS: ≥16, 9–15 and 1–8 (corresponding to the traditional definitions for major and moderate trauma, and the UK trauma best practice tariffs). The sample characteristics and provision of life-saving interventions were then described for each subgroup and compared using Kruskal-Wallis and χ2 tests. Fourth, the association between provision of a life-saving intervention and age was explored. The proportion of patients receiving a life-saving intervention was calculated for different age groups (<20 years, ≥90, and intervening 10 years age bands) and plotted graphically with 95% CIs. The association between the number of life-saving interventions across age groups was then evaluated using χ2 tests. Fifth, the association of life-saving interventions and ISS with mortality was examined by plotting the probability of death against ISS and number of life-saving interventions and performing χ2 tests. Finally, the proportion of patients requiring the highest acuity management at each ISS was examined in a sensitivity analysis using a more restrictive definition of life-saving intervention. This high-acuity definition included advanced airway management, mechanical ventilation, initiation of a resuscitation protocol (eg, ALS), resuscitative transfusion of >4 units of blood and urgent non-orthopaedic surgical or radiological procedures (thoracotomy, laparotomy, neurosurgery, haemorrhage control). This definition closely mirrors that offered by Lerner et al with the exception of intracranial pressure monitoring and a more aggressive stance towards fluid resuscitation.12
Statistical analyses were carried out in Stata V.13.1 (StataCorp, College Station, USA). A two-sided p value <0.05 was considered to be statistically significant. TARN data are submitted in an irreversibly anonymised format with no patient identifiable information available. TARN is funded by contributions from participating hospitals. No additional funding was provided for this study.
Patient and public involvement
No patient involvement.
Results
Study sample
During the study period, 218 985 patients were enrolled in the TARN registry, with 193 290 meeting study inclusion criteria following the exclusion of children and indirect admissions. The median age of the cohort was 60.0 years (IQR 41.2–78.8 years) with males comprising 56.9% (n=110 030) of the sample. Blunt trauma predominated (96.5%, n=186 435) with the leading mechanism of injury being falls less than 2 m (52.1%, n=100 780), followed by road traffic collisions (22.2%, n=42 853). The study population had a median ISS of 9 (IQR 9–16). Over three-quarters of the study population had an ISS ≥9 and thus qualified for the UK major trauma tariff (76.3%, n=147 533), with 30.2% (n=58 404) having an ISS ≥16, thereby meeting the traditional definition of major trauma. 15.1% of the study population received at least one life-saving intervention (n=29 117) with intubation the most frequent procedure (3.2%, n=6218). Full study demographics are provided in table 1.
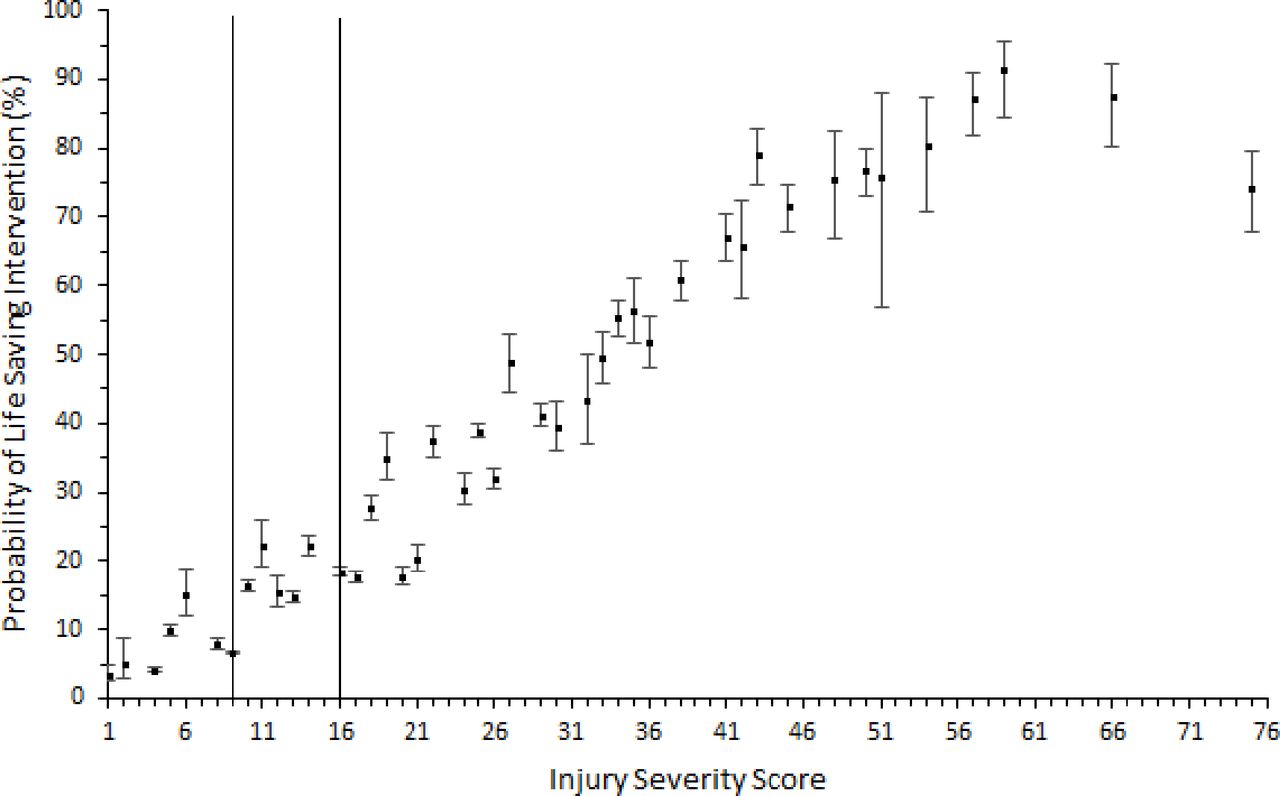
The probability of receiving a life-saving intervention increased with increasing ISS in a curvilinear fashion, from 3.4% for the lowest recorded ISS score of 1, to 75.2% for the highest ISS score of 75 (see figure 1). Low to moderate correlation was evident with a Spearman’s correlation coefficient of 0.334 (p<0.001). When exploring for potential confounding by age, the probability of receiving a life-saving intervention increased in a curvilinear fashion across all age groups (online supplementary figure 1) and a low to moderate correlation was again observed across all age groups (0.391, p<0.001 (18–39.9); 0.358, p<0.001 (40–64.9); and 0.247, p<0.001 (65+)).
Supplemental material

The probability of receiving a life-saving intervention for each Injury Severity Score (ISS). Bars represent 95% CIs. Vertical lines correspond to ISS thresholds for the UK major trauma tariffs (≥9 and ≥16) and the traditional anatomical definition of major trauma (≥16).
A clinically significant number of cases, 5.3% and 7.6%, received a life-saving intervention despite ISS of ≤8 or ≤15, respectively. These interventions comprised high-acuity procedures including intubation and ventilation, or non-orthopaedic emergency surgical intervention, in 1.8% of cases with an ISS ≤8% and 3.4% of patients with an ISS ≤15. Sample characteristics are displayed in table 1.
The probability of receiving a life-saving intervention decreased significantly with age from 26.2% for adults under 20 years to 7.6% for patients 90 years or over as shown in figure 2 (p<0.01). Underlying injury severity remained constant across age categories (median ISS 10 for age groups under 30, median ISS 9 for age groups >30 years). The number of interventions also fell significantly across increasing age categories, with 8.3% of those under 20 years receiving two or more life-saving procedures decreasing to 0.7% of patients aged 90 or over (p<0.01) (figure 3).

The probability of receiving a life-saving intervention across increasing age groups. Bars represent 95% CIs.

Number of interventions across increasing age groups.
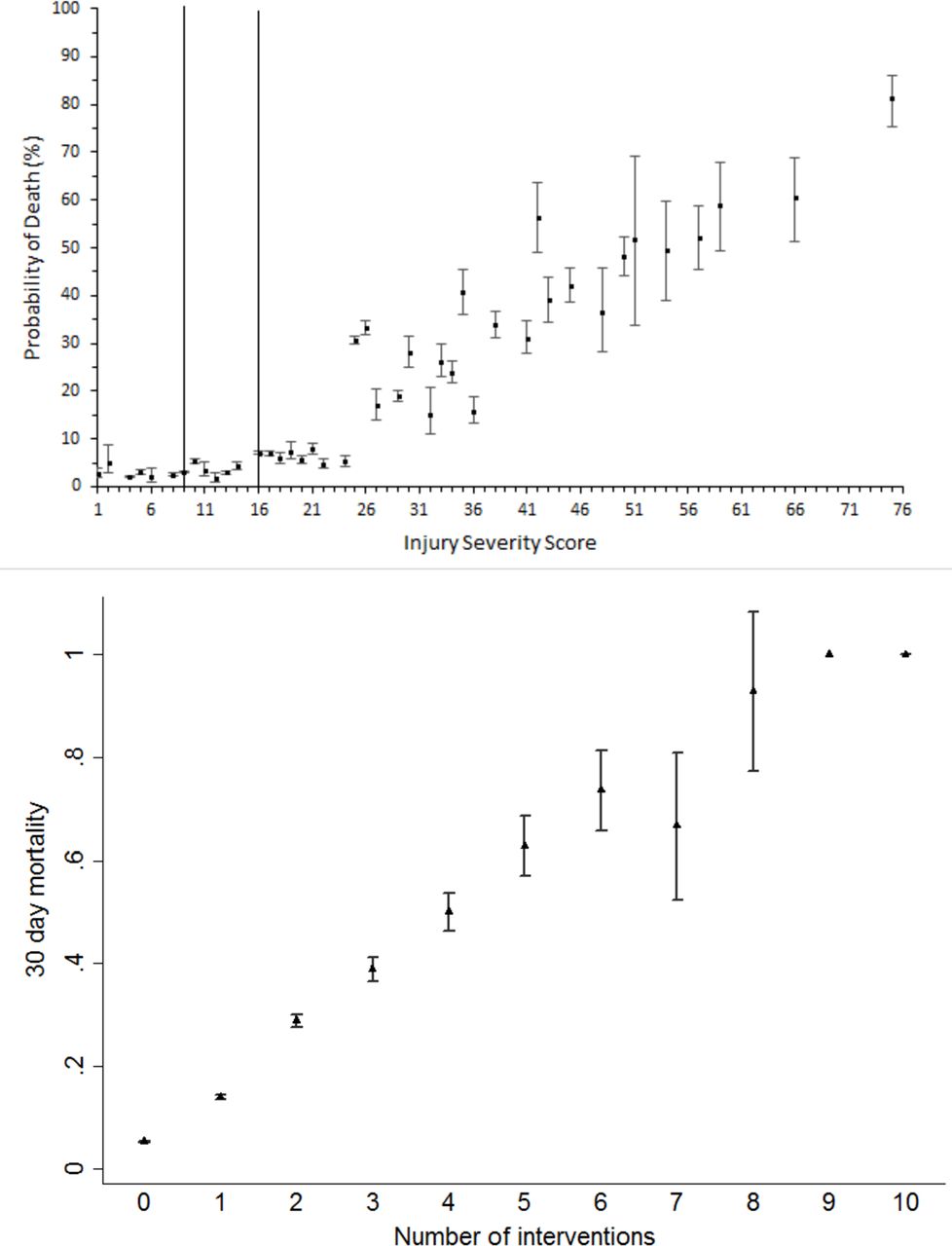
Thirty-day day mortality increased with higher ISS as shown in figure 4 (χ2 test, p<0.01). Correlation was good with a Spearman’s coefficient of 0.91 (p<0.01). Thirty-day mortality slowly increased from ISS of 1 upwards, but remained <10% until an inflection point was observed at an ISS of 25. Further spikes in mortality were present at ISS of 35 and 42. In contrast, the number of life-saving interventions increased in a positive linear relationship with very high correlation (χ2 test, p<0.01; Spearman’s coefficient 0.98, p<0.01). Figure 4 presents the association of mortality with ISS and number of life-saving interventions.
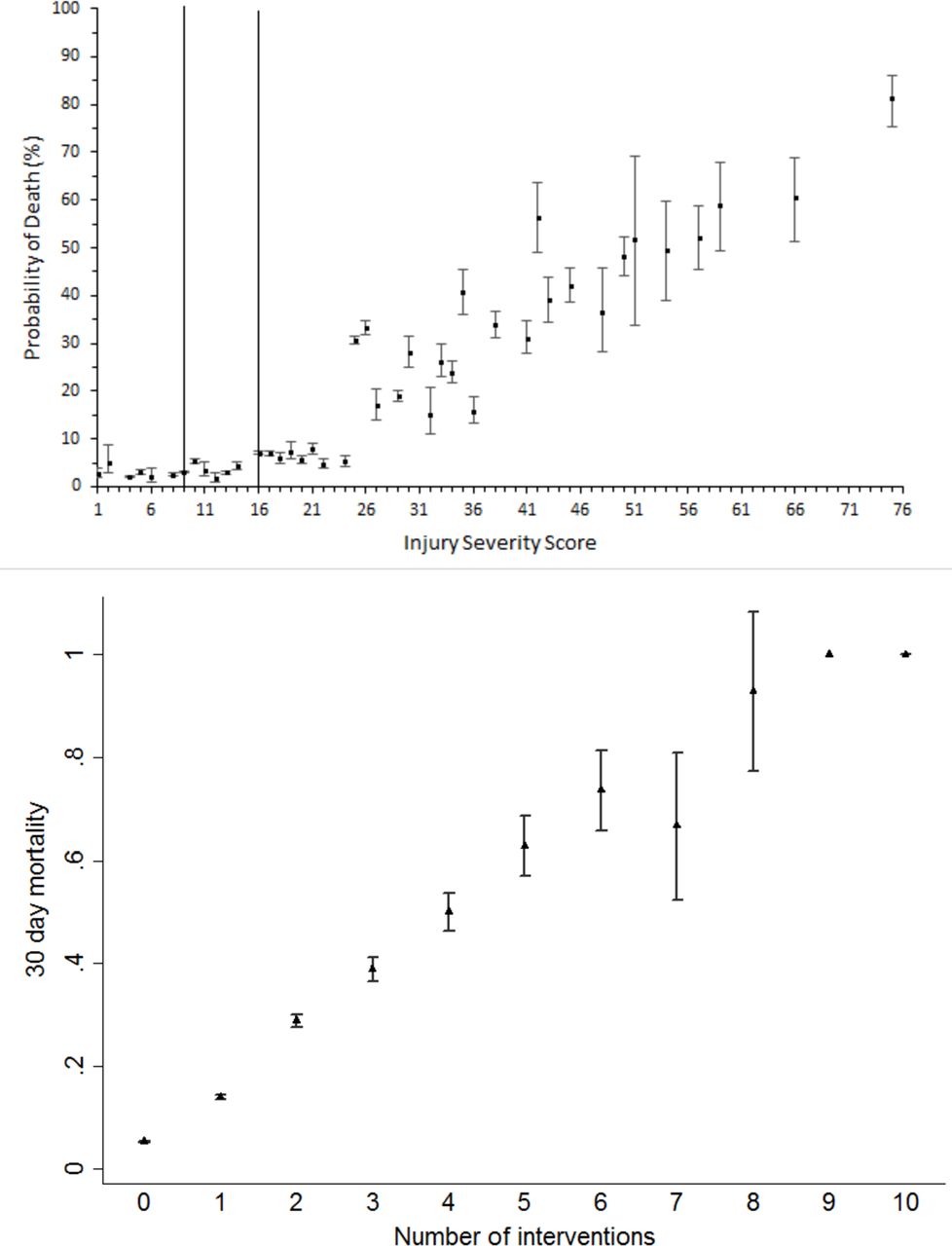
The probability of 30-day mortality with increasing ISS (upper panel) and higher number of life-saving interventions (lower panel). Bars represent 95% CIs. Note that CIs were not tractable for 9 and 10 life-saving interventions secondary to low cell counts.
Sensitivity analysis
An additional analysis was conducted using a restrictive definition of life-saving intervention, with a reduction in cases observed (10.0% (n=19 288) vs 15.1% (n=29 117)). Baseline demographics were largely unchanged between the restrictive and full definitions; predominately male (75.7% vs 71.1%) with a similar proportion of blunt injury (85.7% vs 88.9%) and median age (45.0 vs 48.1 years). However, a higher mortality (25.4% vs 19.6%, p<0.0001) was observed in the restrictive group and this was associated with a significantly higher median ISS (25 vs 19, p<0.0001).
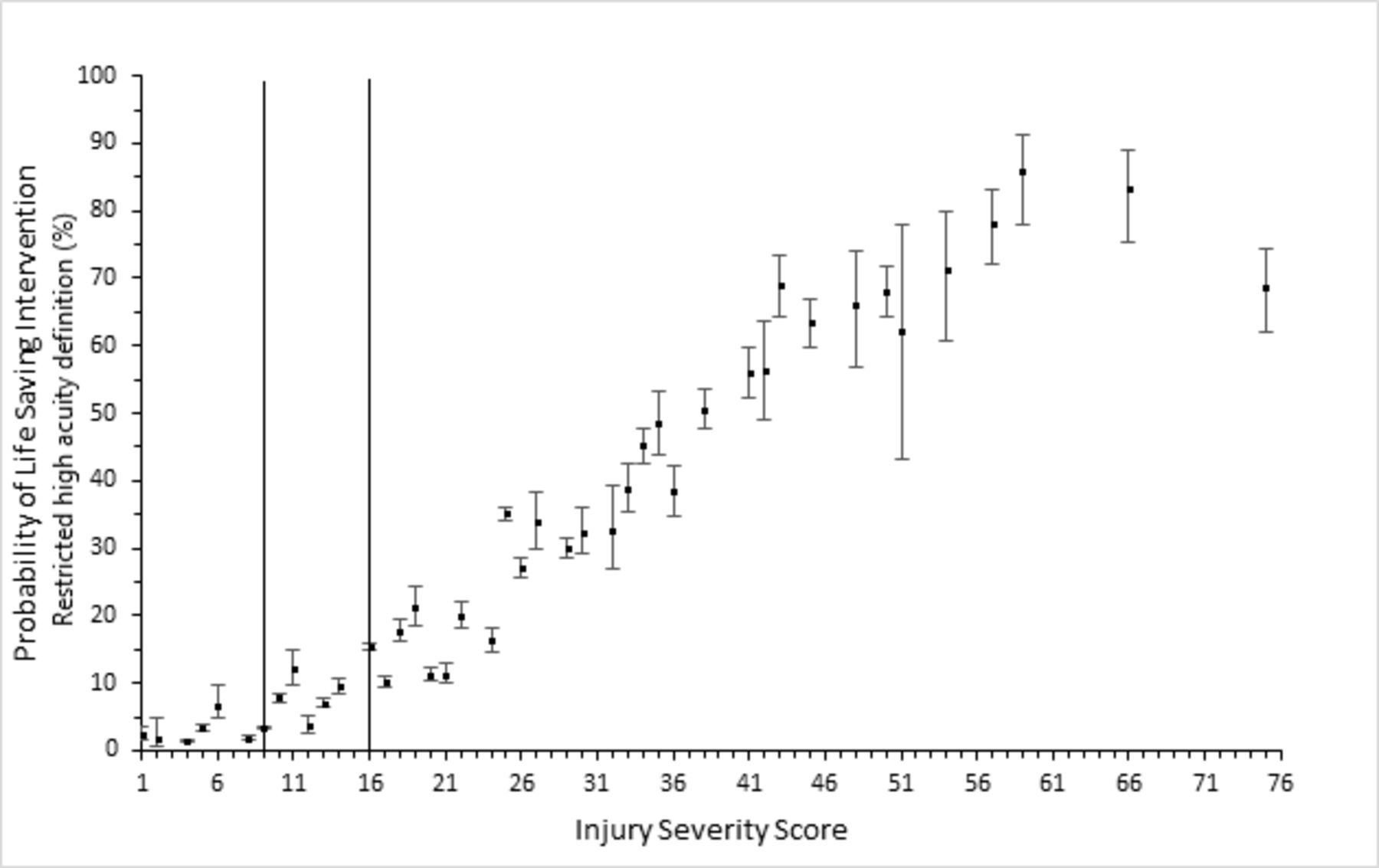
Using this restrictive definition, the results (figure 5) are largely unchanged when compared with the complete analysis (figure 1) with an increased probability of receiving a life-saving intervention with increasing ISS in a curvilinear fashion. A clinically significant proportion of cases, 3.4% (n=4578) received a life-saving intervention from the restrictive definition despite having an ISS ≤15.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The probability of receiving a life-saving intervention (restrictive definition) for each Injury Severity Score (ISS). Bars represent 95% CIs. Vertical lines correspond to ISS thresholds for the UK major trauma tariffs (≥9 and ≥16) and the traditional anatomical definition of major trauma (≥16).
Discussion
This study demonstrates that ISS has only low to moderate correlation with the need for life-saving intervention. This is particularly true for those with a lower anatomical injury burden, in other words, some patients who do not have multiple injuries or a high anatomical injury burden still require a life-saving intervention. To our knowledge, this is the first study to compare the correlation between the ISS and the need for life-saving intervention within the UK trauma population.
We observed that a clinically significant number of patients below the existing UK major trauma tariff ISS thresholds required life-saving interventions; while these thresholds may reflect severity of anatomical injury, they do not necessarily reflect either resource requirements or acuity. Additionally, despite the major trauma patient being traditionally defined as having an ISS >15, a small but potentially clinically significant number of patients were observed to require high-acuity life-saving interventions (such as blood product resuscitation, laparotomy and thoracotomy) despite having an ISS below this threshold.
We have demonstrated that 30-day mortality is strongly correlated with both increasing injury severity and increasing numbers of life-saving interventions received by a patient. The provision of a life-saving intervention appears therefore to be an important criterion in defining the need for MTC care.
The major trauma patient is one who requires the timely delivery of complex interventions within an organised trauma system.18 We must therefore correctly and accurately define this cohort of patients in terms of the interventions that they require. Subsequently, the next stage in the management of these patients is to correctly identify and transport them to the most appropriate medical treatment facility. However, existing methods of identifying major trauma patients, trauma triage tools, have been designed and validated to identify those with an ISS >15.
The findings within this study suggest that the ISS does not fully reflect the need for MTC care, nor is an arbitrary definition of ISS >15 sufficient to define the major trauma patient. This has implications for validating triage rules (to determine who should be transported to an MTC), and for the evaluation of trauma systems and reimbursement in the form of major trauma tariffs. Within the major incident setting, novel triage tools have been derived specifically for the purposes of identifying patients in need of life-saving interventions and we would speculate that this may be a more appropriate metric with which to validate individual trauma triage algorithms.11 12
Baxt and Upenieks were the first to determine a lack of correlation between the ISS and the need for life-saving intervention, with 20% of those receiving a life-saving intervention having an ISS <15.19 Our study provides further evidence, but with poorer correlation; 7.6% of our study population receiving a life-saving intervention had an ISS <15. This difference may be explained to some extent by a different definition of life-saving intervention being used between the two studies. Indeed, several alternative definitions of life-saving interventions have previously been published11–13 20; a comparison is provided in online supplementary table 3.
Although not directly comparing ISS and need for life-saving intervention, Palmer et al 21 reported that of patients requiring urgent surgery or intensive care admission, only 35% and 46%, respectively, had an ISS >12. By comparison, using this lower ISS threshold in our population, less discrepancy is observed with only 14.2% requiring surgery and 26.0% needing intensive care admission.
With regard to mortality, our results are consistent with previous studies demonstrating an increasing mortality with increasing ISS. Previously, an ISS >15 had been described as being consistent with approximately 10% mortality,21 22 which, when age adjusted, increased to approximately 20% in patients over 50 years of age. While an increase in mortality (8.8% vs 4.6%) was observed in our study for older patients sustaining trauma (≥50 years), this remains lower than was previously observed by Copes et al.23 Additionally, the inflection point for increased mortality following trauma occurred at an ISS >25 rather than the traditionally depicted ISS >15 (figure 2). Further adjusting the population for injury type (penetrating vs blunt), overall mortality within our population remained consistently below 10%. The increase in survival across all age groups and trauma mechanisms that is observed in our study is likely to be explained by advances in trauma management, including the introduction of damage control resuscitation and massive haemorrhage protocols. The reduction in numbers of life-saving interventions performed at the higher ranges of ISS is likely to be related to the unsurvivability of these injuries (eg, devastating brain injury) and a ceiling of treatment being applied (figure 2). This is particularly apparent in the elderly population and is likely to explain the observed reduction in correlation coefficient (online supplementary figure 1).
In keeping with other retrospective database studies, there are a number of limitations associated with our study. First, with TARN inclusion criteria, the population will differ from the more complete NHS Hospital Episode Statistics data with the implication that patients receiving life-saving interventions but who do not fulfil TARN inclusion criteria would not be included. Additionally, participation in TARN increased during the study period, but it is recognised that not all non-MTCs (but who do still receive trauma patients) participate in TARN, thereby the population studied is unlikely to be representative of the entire UK trauma population across the whole study period. While ISS and mortality data were recorded for all patients analysed, the ability to determine need for life-saving interventions is dependent on the data recorded and transferred to the database, thereby introducing potential information bias. It is not possible to determine whether an intervention did not occur or whether it was simply not recorded. However, the intensity and high profile of the included interventions might suggest it is unlikely that that there was no record of these procedures in the patient record.
While the interventions used in this study were derived using an international Delphi process, they were originally intended for the major incident setting.14 Although there is likely to be considerable overlap, they were not specifically intended for purposes of determining the need for MTC care. For example, the use of intraosseous access for resuscitation purposes may not necessarily reflect the acuity of a major trauma patient, but rather may be representative of difficult vascular access. Conversely, the findings were materially unchanged in a sensitivity analysis using a more restrictive definition of life-saving intervention, which broadly mirrored previous consensus definitions, for example, the US consensus definition of trauma centre need. Additionally, not all interventions considered life-saving are recorded as variables on the TARN database, thereby requiring surrogates to be used for analysis.24
Lastly, we acknowledge that a considerable proportion of survivors following trauma suffer long-term disability; mortality was the only outcome measure recorded in our study and therefore we are unable to comment on the morbidity following trauma. With TARN now recording patient-recorded outcome measures, this represents a potential avenue for additional future work.
Conclusion
A clinically significant number of adult trauma patients requiring life-saving interventions have an ISS below the traditional definition of major trauma. With only a low to moderate correlation between the ISS and the resource needs of trauma patients, the validity of using the ISS as a method of defining the major trauma patient, validating triage algorithms and determining reimbursement is brought into question. We believe that this original definition should be reconsidered, and either lowered, or an alternative metric should be used.
Acknowledgments
The authors thank Professor Fiona Lecky (research director) and Antoinette Edwards (chief executive officer) at Trauma Audit Research Network (TARN) for facilitating access to the TARN database.
References
Footnotes
Handling editor Caroline Leech
Presented at RCEM Annual Scientific Conference 2018
Contributors JV devised the study, conducted the initial analysis and wrote the first draft. GF conducted additional analyses and helped produce the second draft. JES oversaw the project and revised the drafts for critically important intellectual content. All authors approved the final version. JV takes responsibility for the manuscript as a whole.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The National Information Governance Board for Health and Social Care regulates the use of patient information in the UK and has previously provided ethical approval for research using anonymised TARN data (approval number: PIAG3-04(e)/2006).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. Data came from the TARN database.