Article Text

Abstract
COVID-19 has had a significant effect on healthcare resources worldwide, with our knowledge of the natural progression of the disease evolving for the individual patient. To allow for early detection of worsening clinical status, protect hospital capacity and provide extended access for vulnerable patients, our emergency department developed a remote patient monitoring programme for discharged patients with COVID-19. The programme uses a daily emailed secure link to a survey in which patients submit biometric and symptoms data for monitoring. Patients’ meeting criteria are escalated to a physician for a phone or video visit. Here, we describe the development, implementation and preliminary analysis of utilisation of the programme.
- emergency care systems
- emergency departments
- emergency department management
- effectiveness
- infectious diseases
- viral
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
- emergency care systems
- emergency departments
- emergency department management
- effectiveness
- infectious diseases
- viral
Background
One of the most feared complications of COVID-19 is respiratory failure. Although some patients are known to be at high risk of complications, understanding of the natural history of COVID-19 is incomplete. Clinicians are unable to predict which patients will decompensate and at what time point during the illness decompensation might occur. Given capacity-constrained healthcare systems, patients at low risk of decompensation should be managed as outpatients.1–4 Remote patient monitoring (RPM), the transmission of physiologic data from the home setting to clinicians, allows patients to be routinely monitored outside the hospital setting. RPM is typically used in management of chronic conditions such as diabetes and hypertension.5 6 RPM can be used longitudinally to both escalate patient care at the earliest signs of worsening as well as to provide reassurance for patients and connection to the healthcare system for those isolating at home.
During the COVID-19 pandemic, health systems in the USA have rapidly scaled up the use of telehealth to safely care for patients through episodic visits.7 This was aided by changes to regulations that allow non-primary care physicians to initiate and be reimbursed for remote monitoring for patients with acute conditions and specifically to improve the care of patients with COVID-198 9
In this paper, we outline our experience rapidly developing and deploying an RPM programme for patients diagnosed with COVID-19 and discharged from an urban, academic emergency department (ED) in Washington, DC, USA. The department serves mainly adult patients and has an annual census of approximately 86 000. Our objective was to allow for early detection of worsening clinical status in low to moderate risk patients diagnosed with COVID-19 who are deemed appropriate for discharge from the ED.
Phase I: programme development
We conceived a programme to monitor discharged patients with COVID-19 during the acute phase of illness. The RPM programme leveraged our 24-hour telehealth command centre, which provides telemedicine access to board certified emergency physicians (EPs) for individuals in remote or isolated settings, in particular, the maritime and aviation industries. From 2012 to 2015, the centre supported an innovative RPM research study of patients on home peritoneal dialysis that demonstrated feasibility and improved outcomes.10 General concepts from remote monitoring of patients with chronic conditions were adapted to meet the need to monitor those with an acute condition. The COVID-19 RPM programme was designed using existing information technology software platforms: Power Automate, Forms (Microsoft Corporation, Redmond, Washington, USA) and QuickBase (Quickbase, Cambridge, Massachusetts, USA). The use of these applications ensured that security features and appropriate agreements were in place to meet all requirements for patient privacy protection such as compliance with the Health Insurance Portability and Accountability Act, the federal law that governs the privacy and security of protected health information in the USA. This strategy allowed for rapid implementation on a platform that is secure, low cost, web-based and simple to use.
A process map was built accounting for daily data collection (figure 1) to conceptualise how patients flow through the programme. The existing software infrastructure allowed our informatics physician to quickly build surveys and a COVID-19-focused RPM dashboard. The administrative team developed a registration process to ensure that patients would be called within 24 hours of ED discharge to answer questions about the programme, confirm demographics, initiate the medical record, capture insurance information and to complete patient onboarding. Collection of accurate patient registration data, consent and insurance information was an operational challenge of the programme and required coordination between the ED, outpatient department’s registration staff and the telehealth command centre.

Remote patient monitoring programme protocol, graduation and escalation criteria. ED,emergency department; EMT, emergency medicaltechnician.
Prior to launch, educational materials were developed as well as front-end guidance for EPs regarding patient selection and enrolment criteria (table 1), referral procedures and provision of home monitoring equipment. These materials were distributed by email to all clinicians as well as posted in the ED. The nursing staff, who serve as advocates for the programme, were made aware of the programme through their daily huddles. Informational, educational and consent documents were created for patients in both English and Spanish. These included general information and a detailed description of the programme with videos in English and Spanish coupled with electronic and physical teaching materials.
Enrolment criteria for the COVID-19 remote patient monitoring programme
Phase II: implementation
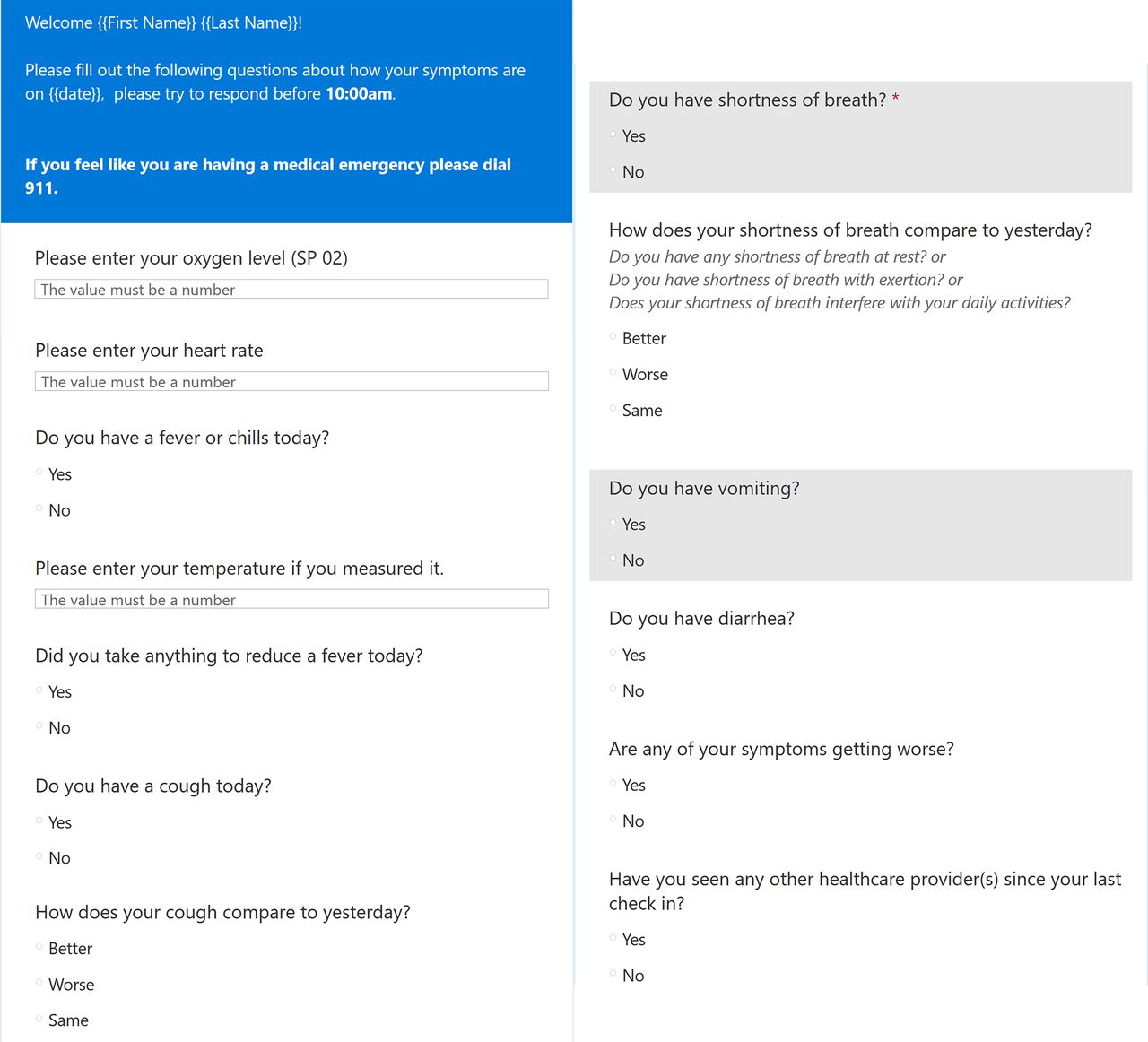
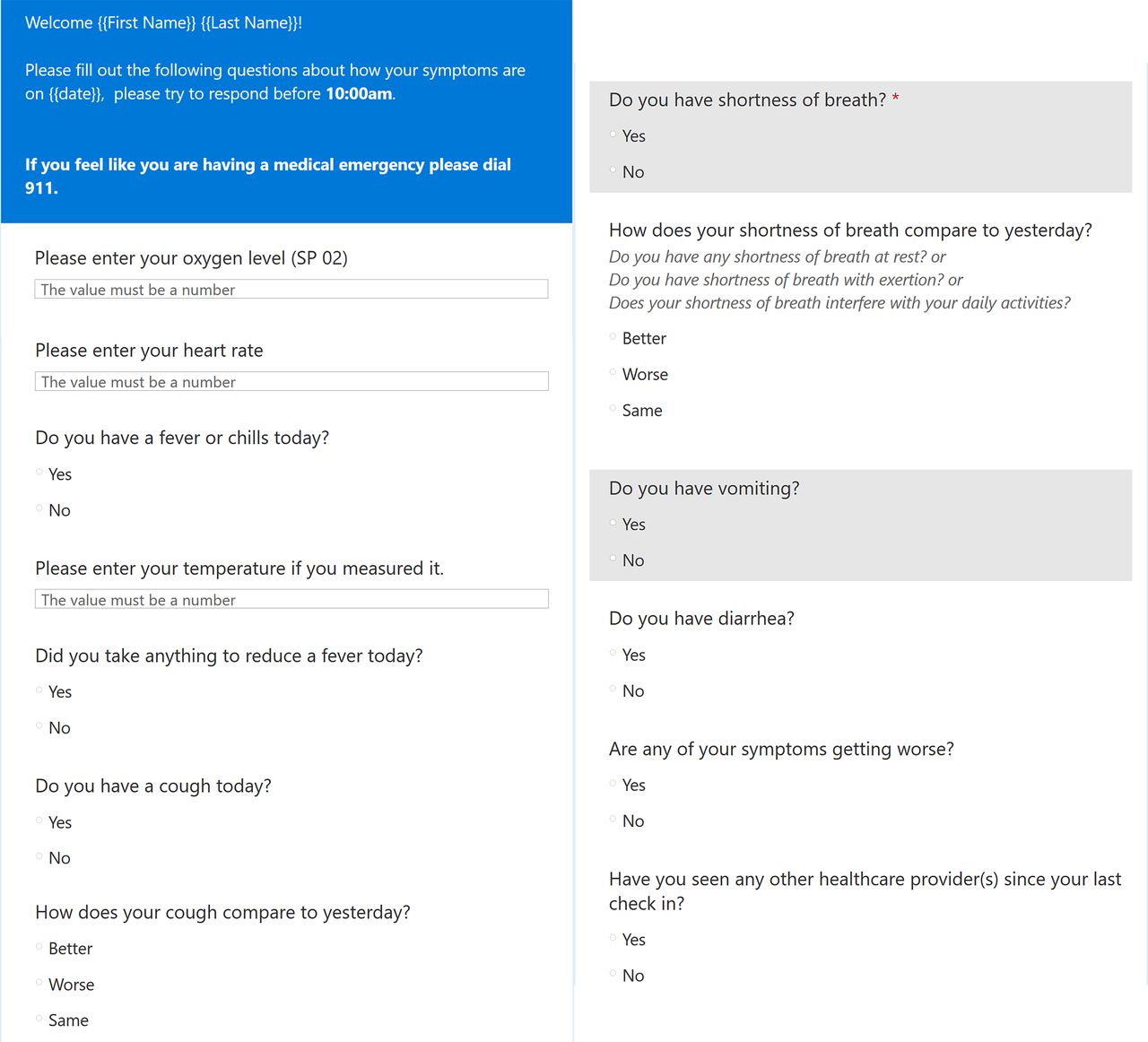
Patients were referred to the programme by their treating ED provider and given verbal and written instructions, a pulse oximeter and a thermometer while still in the ED. Each morning an automated email was sent to each patient in the programme with a hyperlink to a short survey. This survey contained simple language and basic questions to elicit information about patients' symptoms, improvement or deterioration, their temperature, heart rate and oxygen saturation (figure 2).
{kind=link}
{kind=link}
Remote patient monitoring programme daily monitoring survey.
A tiered escalation model was developed to account for non-responding patients and patients submitting abnormal vital signs or worsening symptoms. Survey responses are automatically analysed by our dashboard and flagged for clinician follow-up if they indicate possible deterioration (figure 1). An emergency medical technician (EMT) in the command centre calls flagged patients to verify the validity of the trigger. Based on the predetermined criteria (figure 1), one of three patient actions will be recommended; return to routine monitoring, escalate to a telemedicine appointment with a dedicated COVID-19 telemedicine doctor (ED physicians) or refer to the closest ED with activation of the 911 systems for ambulance transport if deemed necessary.
Phase III: optimisation
After enrolling the first 15 patients, we paused enrolment for 48 hours to incorporate experience into the process of enrolment, patient call backs, documentation and escalation rules. Graduation criteria (figure 1) for monitored patients were developed based on early observations of the programme and Centres for Disease Control and Prevention criteria for discontinuation of isolation. We are closely monitoring clinical outcomes to refine enrolment criteria, adjust clinical pathways to ensure that patients receive the most appropriate follow-up and to determine how to expand the programme.
Preliminary data
We present results for the first 83 patients enrolled for monitoring. Patients responded to (1 848) surveys, 869 (47%) were completed over the phone by the EMT when patients did not complete the electronic survey sent by email on time for any given day. Patients were monitored for an average of 21.8 days (1–42, median 18) and completed an average of 14.5 (3–57, median 13) daily survey responses. During their monitoring period, 60 (72%) patients triggered an automated flag at least once, 39 (47%) patients were escalated to a telehealth consult and 17 (20%) patients were referred to the ED for inperson evaluation and possible admission. Five (6%) of these 17 were referred to the ED by ambulance transport (911). The average time of human interaction with healthcare providers was 48.7 (median 45.5, range 4–143) min per patient during the monitoring period, which included EMT calls to patients, time spent on data review and physician calls to patients and excluded telehealth visits.
Discussion
There have been numerous attempts to leverage connected health technologies, such as RPM, to meet demands placed on the healthcare system during the COVID-19 pandemic.11 Infrastructure and processes developed through RPM programmes have the potential to enhance outpatient management of COVID-19 from the point of diagnosis, whether at a telemedicine visit, outpatient clinic visit or urgent care or ED visit as well as after hospital discharge. Based on our preliminary data (56%), 22 out of the 39 patients who triggered a red flag and needed a provider evaluation did not need an inperson evaluation and benefited from a telehealth visit, avoiding unnecessary exposure and related personal protective equipment use. However, monitoring did require extensive human resources to ensure appropriate engagement and follow-up.
There have been a variety of RPM programmes recently reported in the literature. COVID-19 Watch, an RPM programme at the University of Pennsylvania, demonstrated high patient engagement, using short message service messaging to check-on patients with COVID-19 isolating at home two times daily, and if worsening, escalate to a clinician for assessment.12 An RPM programme in Minnesota similarly used patient monitoring questionnaires and enrolled patients in RPM after telemedicine, urgent care and ED visits.13 In a programme described by Gordan et al in Boston, patients were provided a pulse oximeter, thermometer and app-based symptom reporting on hospital discharge.14 Only 14 of 225 enrolled patients in the programme had a repeated ED visit or hospital readmission.14 The COVID-19 precision recovery programme in New York has a similar model to ours but has only reported patient demographics to date.15 The data generated by these programmes in their various formats may help clarify the natural history of COVID-19, enabling evidence-based identification of patients who may benefit from early intervention or escalation to inperson care. Importantly, RPM programmes consistently receive positive reception among healthcare workers and patients, as without their engagement, these programmes would not be possible.
Conclusion
RPM, traditionally used for chronic condition management, underwent a crisis-induced expansion for use in acute disease monitoring, demonstrating high levels of engagement. Further study is needed to understand efficacy, cost, risk and implications of using RPM in the acute or postacute setting for COVID-19 as well as other diagnoses.
Footnotes
Handling editor Mary Dawood
Twitter @draalam
Contributors All authors have contributed in writing the manuscript and building the remote patient monitoring program.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.