Article Text

Abstract
Background: The decision by paramedics to alert a receiving hospital to the imminent arrival of a critically ill patient is currently based on the crew’s clinical judgement.
Aims: To evaluate the efficiency of current alerting practice and to assess the need for objective guidelines.
Methods: Data were collected in the Birmingham Heartlands Hospital, Birmingham, UK, over 1 week in February 2005. All alerted patients and all critically ill patients brought to the emergency department over this time period were identified. These two groups were studied to find those patients who were alerted but not critically ill, those who were critically ill but not alerted, and those who were both alerted and critically ill. The presenting conditions were identified and compared between groups.
Results: 454 patients were brought by ambulance to the emergency department during the study week. Of the 27 alerted patients, 23 were critically ill, leaving four patients alerted inappropriately. 29 of the 52 critically ill patients had not been alerted by ambulance crews. Most (n = 22) of these patients were adults with medical conditions.
Conclusions: Ambulance crews do not alert hospitals to critically ill patients adequately. The Modified Early Warning Score should be considered to be the basis of a prehospital tool to aid their decision.
- MEWS, Modified Early Warning Score
Statistics from Altmetric.com
Alerting of hospitals for critically ill patients by paramedics allows hospital staff time to prepare the necessary space, personnel and equipment to ensure that appropriate and timely medical care is delivered. Where crews alert hospitals too readily (overalerting), hospital trauma and medical teams might be assembled unnecessarily and this can lead to a general apathy to ambulance alerts. Conversely, underalerting may cause delays in providing care for critically ill patients.
Currently, the decision whether to alert a hospital or not depends predominantly on the experience and clinical acumen of the ambulance crew. Guidance from the Joint Royal Colleges Ambulance Liaison Committee merely states that “in all time critical cases, pre-alert of the receiving hospital and request of an appropriate team standby is essential”.1
Previously, attempts have been made to provide ambulance crews with scoring systems to enable them to identify patients most in need of immediate medical attention, and hence to alert hospitals appropriately.2 Most of these scores have been compiled for patients with trauma—for example, the Circulation, Respiration, Abdominal Motor and Speech Scale3 and the trauma score.4 Critically ill patients form a larger proportion of the paramedic workload than critically injured patients.5,6 Little has been done to provide ambulance crews with a tool to determine how unwell these medical patients are. In hospitals, the Modified Early Warning Score (MEWS) is a widely used and well-validated indicator of the severity of a patient’s condition and is used to prompt the escalation of treatment.7 The score is compiled from routinely recorded observations. Its use does not currently extend to prehospital care.
Previous studies have identified that inappropriate alerts are infrequent and underalerting is a more common problem,6,8 particularly in medically ill patients. Evidence suggests that although patients with severe trauma are also often underalerted, the overalerting of patients with non-severe trauma is a common problem.9
We present a study of current alerting practice in the emergency department at the Birmingham Heartlands Hospital, Birmingham, UK, under the Joint Royal Colleges Ambulance Liaison Committee guidelines, to identify which patients are underalerted or overalerted. We suggest a method for developing clearer guidance for ambulance crews.
METHODS
We reviewed the records of all patients who arrived by ambulance during 1 week in February 2005, and identified two groups of patients:
1. Patients alerted to the emergency department: All ambulance-alerted patients were identified prospectively from the alert log that is kept by the alert telephone and is completed for every alert call.
2. Critically ill patients attending the emergency department: The computerised emergency department records were searched for critically ill patients brought in by ambulance over the same 1-week period. Allocation to this category was determined by one or more of the following criteria:
a. Triage category of “priority one” (Manchester triage system) on arrival at the department
b. Presenting complaint or diagnosis of any of the following: cardiac arrest, respiratory arrest, myocardial infarction, severe burns, status epilepticus, ruptured ectopic pregnancy, shock, coma, hypothermia, poisoning, meningitis, acute pulmonary oedema or life-threatening asthma
c. Immediate requirement of any of the following: theatre, intensive care unit, high-dependency unit, mortuary or transfer to tertiary centre for definitive care.
The criteria for defining critically ill patients in this second group were determined prospectively by the authors to include all patients for whom immediate reception by emergency department staff seemed appropriate.
In the emergency department at the Birmingham Heartlands Hospital, most alerts are intradepartmental. The standard alert bleep notifies the emergency department consultant, specialist registrar and senior house officer on call. Other personnel from departments such as paediatrics, anaesthesia and trauma are called as required by the senior emergency department staff.
The emergency department records were retrieved for both groups. All critically ill patients were assumed to have been alerted by the ambulance service.
Analysis of the two groups and the overlap between them identified four categories of patients. These were as follows: alerted patients who were critically ill (appropriate alerts); alerted patients who were not critically ill (inappropriate alerts); critically ill patients who were not alerted; and stable patients who were not alerted. Underalerting and overalerting were identified from these categories. The presenting conditions for all patients were grouped into arrests, medical (non-arrest), paediatric (non-arrest) and surgical.
RESULTS
In all, 454 patients attended the emergency department by ambulance during the 1-week study period. Of these, 30 (6.6%) patients were alerted. Of these 30 patients, 27 were identifiable from the emergency department computer records. As per our criteria, 23 of these alerted patients were critically ill, leaving four inappropriate alerts. As the “appropriateness” of the alert in three cases could not be determined, 77–87% of the alerts were appropriately made, whereas 13–23% were inappropriate.
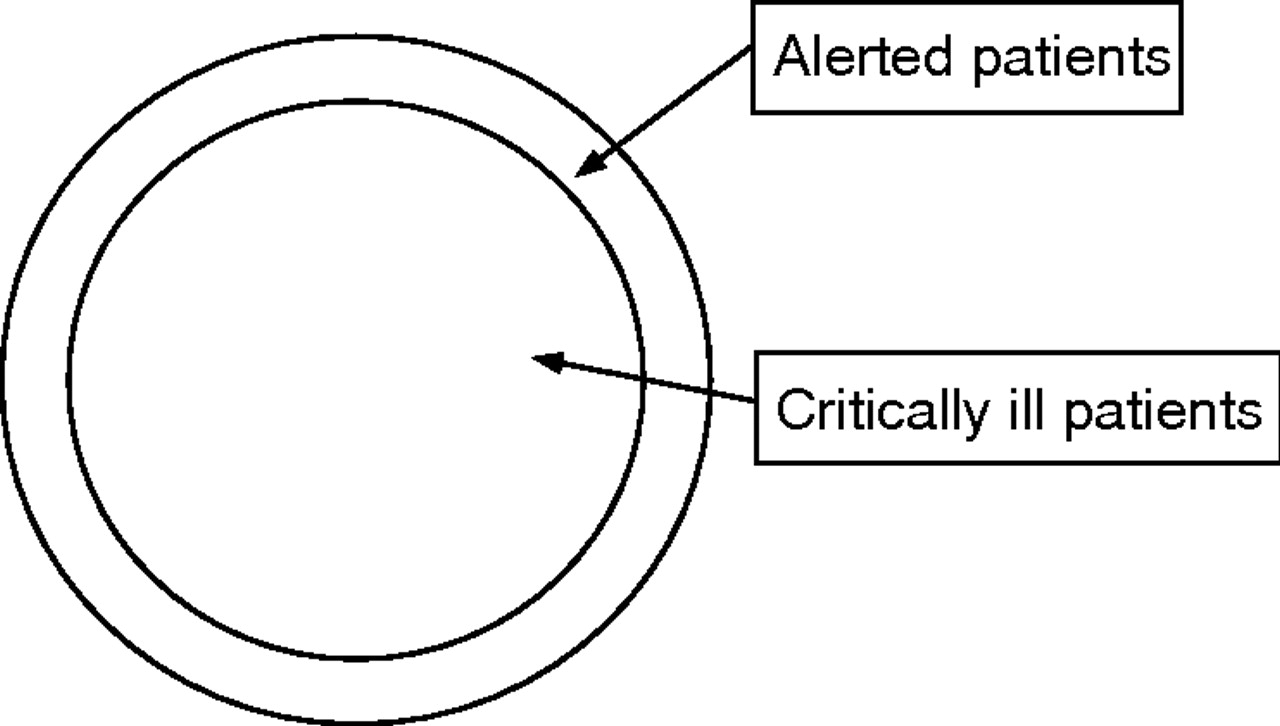
In all, 52 of 454 (11.4%) patients fitting the critically ill criteria were identified over the same period. Of these, 23 (44%) had been alerted, whereas the remaining 29 (56%) critically ill patients arrived at hospital unannounced (fig 1). Also, 395 patients were stable and not alerted—these shall not be considered further.

Overview of results.
Appropriate alerts (critically ill and alerted)
All of the six patients with cardiac and respiratory arrests had been alerted. Most other appropriate alerts were medical. One patient qualified as critically ill purely by triage category; he presented with a severe exacerbation of chronic obstructive pulmonary disease. This group included five patients with trauma and two paediatric patients (table 1).
Category of patient by diagnosis or destination
Inappropriate alerts (alerted but not critically ill)
Four patients who were not in the critically ill category were alerted. They were stable patients with medical conditions (table 1).
Critically ill patients who were not alerted
Of the 52 critically ill patients attending the emergency department by ambulance, 29 (56%) had not been alerted. Most patients in this group were medically unwell patients, including eight patients with myocardial infarcts (table 1).
Overview by specialty
Medical patients form the majority of all groups, and 22 of the 29 (76%) patients were in the “needed alerting” group (table 2).
Overview by specialty
DISCUSSION
Our study provides a 1-week snapshot of ambulance-alerting activity in a large inner-city hospital. The paramedics made their alerting decisions prospectively; we evaluated their decisions retrospectively using clinical notes describing subsequent hospital assessment and diagnoses. Notwithstanding these limitations, our findings suggest that most alerted patients are alerted appropriately (85%) by ambulance crews (slightly lower than the 93% found by Brown and Warwick8). However, many seriously ill or injured patients continue to arrive at the hospital without the benefit of prior warning (56% of all critically ill patients). Although we acknowledge that some patients will become critically ill only after their arrival at hospital, this remains a subject of concern.
The largest group of underalerted patients in our study is that of patients presenting with medical problems; this is particularly a problem in patients presenting with chest pain. These findings correlate with previous data suggesting that medically ill patients are those most likely to be missed.8 Alerting practice regarding these patients needs to be improved.
We found overalerting to be a comparatively smaller problem (15%). In comparison, Brown and Warwick8 found that 7% of alerts were unnecessary by clinical condition at presentation. However, the literature on this aspect is scarce and other figures vary from 0.7% (impression of an alert being unnecessary)6 to 75% when applied purely to patients with trauma.9 Further studies are required to quantify ambulance alerting practice more accurately.
Previous attempts to provide ambulance crews with scoring systems to allow them to identify patients most in need of immediate medical attention have been largely limited to the assessment of patients with trauma.2 Critically ill medical patients form a larger proportion of the paramedic workload than critically injured patients.5 Little has been done to provide ambulance crews with a tool to determine how unwell these patients are; hence, there is no clear threshold at which ambulance crews trigger a hospital alert.
Ideally, hospitals should receive a prior alert for all critically ill patients en route to the emergency department. A few non-critical patients could also be alerted to allow a small margin of safety and to account for the mechanism and unusual circumstances. Figure 2 shows this model of “ideal” alerting practice.
{kind=link}
{kind=link}
Ideal alerting practice.
MEWS10 (table 3) is a widely used tool to aid recognition of the critically unwell patient in hospital. Physiological variables (heart rate, respiratory rate, temperature, conscious level, urine output, systolic blood pressure and oxygen saturations) are measured and used to calculate a score that, at a certain threshold, will prompt staff to activate an urgent medical or critical care outreach team review. At the Birmingham Heartlands Hospital, a MEWS of 4 will trigger an urgent medical review.
The Modified Early Warning Score10
MEWS is related to in-hospital mortality,7,11,12 length of stay11 and need for intensive or high-dependency care.7 It is well validated in hospital for both medical7 and surgical13,14 patients, and has been found to decrease mortality, reduce hospital stay and reduce the rate of readmission when acted upon appropriately.15
MEWS could be modified further for use in prehospital care by removing the need to record urine output and temperature, although this new prehospital variant of MEWS would need to undergo field testing and validation. This would include the retrospective application of MEWS variants to prehospital variables to test whether the use of such a score would have increased alerting of critically ill patients. The other physiological variables in MEWS are routinely measured by paramedic crews in unwell patients.
A threshold within the score could be determined to trigger an alert call to the receiving hospital. We would suggest that the level at which a new prehospital MEWS would trigger an alert be set at 5, although further work through re-audit is required to validate this proposal.
Any scoring system developed for prehospital carers needs to acknowledge crew experience, and will not take into account non-medical factors such as mechanism of injury or illness, and comorbidity or specific environmental factors. This type of approach has been introduced in South Africa in the form of the Cape Triage Score. This score is a novel approach and serves as a starting point for exploring this type of prehospital assessment model for introduction in the UK.16,17
Acknowledgments
We thank Colonel Timothy Hodgetts for his advice and the clerical staff at Heartlands Hospital for retrieving the records.
REFERENCES
Footnotes
-
Competing interests: None.