Article Text

Abstract
Objective: To compare the prognostic abilities of lactic acidosis and hyperlactatemia and determine the influence of metabolic acidosis when attempting to predict the outcome of septic patients using serum lactate levels.
Method: 126 patients with severe sepsis or septic shock were prospectively included in this study at an emergency department. Haemodynamic variables, simplified acute physiology score (SAPS) II, arterial blood gas studies and serum lactate levels were obtained at the time of presentation (0 h) and 4 h after presentation. The probability of mortality was calculated using SAPS II scores and compared with actual inhospital mortality at different serum lactate levels and arterial pH. Survival curves for lactic acidosis and severe hyperlactatemia were analysed using the Kaplan–Meier method.
Results: The calculated probability of mortality decreased from 35.7% (95% CI 30.2 to 41.2) at presentation to 29.3% (95% CI 24.2 to 34.4) at 4 h post-presentation. 27.0% of patients (34) died in hospital. Arterial pH and SAPS II scores were independent factors for predicting mortality of septic patients, at 0 h and 4 h. Serum lactate levels were closely related to severity of illness and metabolic acidosis in septic patients. Patients with lactic acidosis had significantly higher inhospital mortality than patients with normal pH and normal lactate levels by Kaplan–Meier survival analysis as determined based on measurements made at 0 h and 4 h (p<0.001, p<0.001 by the log-rank test, respectively). No significant difference in survival was found between patients with hyperlactatemia and those with normal pH and serum lactate levels.
Conclusion: Lactic acidosis not hyperlactatemia was found to predict inhospital mortality more exactly in severe sepsis and septic shock patients. The acid-base state should be considered when attempting to predict the outcome of septic patients using serum lactate levels.
Statistics from Altmetric.com
Tissue hypoxia is one of the most important prognostic factors in septic patients.1 2 If uncorrected, tissue hypoxia can drive the pathogenic effects of sepsis and lead to organ failure and death.2 Moreover, tissue hypoxia induces lactate production, and numerous studies have concluded that serum lactate can be used as a prognostic marker of global tissue hypoxia in circulatory shock. However, the merits of a single serum lactate determination as a marker of tissue hypoperfusion are debatable,3 4 and therefore serial measurements of serum lactate or lactate clearance rates have been used to predict mortality.5 6 Moreover, the importance of lactate clearance remains an issue for study and it is uncertain which of the absolute serum lactate level on admission or lactate clearance is the better predictor of patient outcome. Although hypoxic tissues have elevated rates of anaerobic glycolysis and lactate production, well-oxygenated tissues can also generate lactate via aerobic glycolysis.7 Lactate generated via tissue hypoperfusion is, however, associated with high serum levels and metabolic acidosis.7 In addition, dysfunctional tissue perfusion in septic shock reduces lactate and hydrogen ion elimination from tissues and thus aggravates lactic acidosis. Mild to moderate hyperlactatemia frequently presents as an endogenous accompaniment to elevated endogenous catecholamines after shock or trauma.3 Hyperlactatemia without acidosis does not, however, predict mortality in septic shock.8 In order to use serum lactate as a prognostic indicator, it is important to differentiate lactic acidosis and hyperlactatemia (normal pH and an elevated lactate level). We hypothesised that lactic acidosis (high serum lactate levels with metabolic acidosis) may more accurately reflect tissue hypoperfusion and be more closely related to mortality in septic patients than hyperlactatemia without metabolic acidosis.
The aims of this study were to compare the prognostic abilities of lactic acidosis and hyperlactatemia and to determine the influence of metabolic acidosis when attempting to predict the outcome of septic patients using serum lactate levels.
MATERIALS AND METHODS
Study design
This was a prospective observational study of a series of adult patients enrolled from January 2005 to June 2007. Our Institutional Review Board approved the study and waived the requirement for informed consent.
Setting
The study was carried out in a 590-bed university teaching hospital with a 40-bed emergency department (ED) that provides care for approximately 40 000 patients per year. The mean ED stay time was 247 minutes (SD 74).
Study protocol
A total of 133 adult patients over 20 years of age who presented at the ED with severe sepsis or septic shock were enrolled in the study. The inclusion criteria consisted of a suspected sepsis source and the following:9 (1) septic shock; two of the four systemic inflammatory response syndrome criteria (temperature >38°C or <36°C; heart rate >90 beats/minute; respiratory rate >20 breaths/minute or arterial carbon dioxide tension <32 mm Hg; white blood cell count >12 000 cells/μl or <4000 cells/μl or >10% of band cells) and a systolic blood pressure of less than 90 mm Hg after a 20 ml/kg fluid challenge and/or (2) severe sepsis; two of the systemic inflammatory response syndrome criteria with organ dysfunction. The exclusion criteria were patient with trauma, acute myocardial infarction, seizure, haemorrhagic shock, requiring immediate surgery and do not attempt resuscitation order. Therapies in the ED included antibiotics, fluid resuscitation, mechanical ventilation, vasopressor and inotropics as required. Patients were initially resuscitated with normal saline. Central venous access was established within 1 h after ED presentation. Hypotensive patients with an adequate filling pressure were treated with a vasopressor, such as dopamine or norepinephrine.10 The clinical goals of resuscitation were a mean arterial blood pressure of 65 mm Hg or more, a central venous pressure (CVP) of 10 cmH2O or more, an hourly urine output of 0.5 ml/kg or more and a central venous oxygen saturation (Scvo2) level of more than 70%.9 10
Measurements
The primary outcome was inhospital mortality. Blood pressure, respiratory rates, heart rates and electrocardiography findings were routinely monitored and patient demographic information and admission diagnoses were recorded. The arterial blood gas variables, CVP, Scvo2, pH and serum lactate levels were obtained at the time of presentation (0 h) and at 4 h after presentation.
Simplified acute physiology scores (SAPS) II were used during ED treatment to assess illness severity and physiological condition and to calculate the probability of inhospital mortality on a patient-by-patient basis.11
Primary data analysis
Measured values (blood pressure, arterial pH, serum lactate levels, etc) were compared for survivors and non-survivors. Estimated lactate clearance was calculated by dividing the difference between serum lactate levels at 0 h and 4 h post-presentation by the lactate value at presentation. Multiple logistic regression analysis was used to identify variables (at 0 h and 4 h post-presentation) that were independently associated with death. Significant variables at 0 h and 4 h were entered into a backward, stepwise, logistic regression model. Changes in the probability of mortality, as determined using the SAPS II score and serum lactate levels were analysed to determine the nature of the relationship between sepsis severity and serum lactate level. The relation between arterial pH and serum lactate was investigated to determine the relationship between serum lactate and metabolic acidosis. Patients were categorised into six groups based on arterial pH and serum lactate level as follows:7 12 (1) normal (pH ⩾7.35 and serum lactate <2.0 mmol/l); (2) mild hyperlactatemia (pH ⩾7.35 and serum lactate 2.0∼5.0 mmol/l); (3) severe hyperlactatemia (pH ⩾7.35 and lactate ⩾5.0 mmol/l); (4) only acidosis (pH <7.35 and lactate <2.0 mmol/l); (5) mild hyperlactatemia with acidosis (pH <7.35 and lactate 2.0∼5.0 mmol/l); (6) lactic acidosis (pH <7.35 and lactate ⩾5.0 mmol/l). Actual inhospital mortality was compared with the probability of mortality to compare the treatment outcome between the groups. The survival curves of the severe hyperlactatemia and lactic acidosis groups were drawn using the Kaplan–Meier method at 0 h and 4 h post-presentation and were compared with those of the normal group using the log rank test. All statistical analyses were carried out using SPSS version 11.0, and the data are expressed as means (SD) or as means (95% CI). Continuous variables were compared using one-way analysis of variance or Student’s t-test, as appropriate. Proportion was compared using the χ2 test. p Values of less than 0.05 were considered significant.
RESULTS
Baseline characteristics of patients and ED management
Six patients with do-not-attempt-resuscitation orders and one patient requiring immediate surgery were excluded. A total of 126 patients was analysed in this study. There were 48 septic shock patients. The probable mortality of patients determined using SAPS II decreased from 35.7% (95% CI 30.2 to 41.2) at presentation to 29.3% (95% CI 24.2 to 34.4) at 4 h, after initiating ED therapies. Thirty-four patients (27.0%) died in hospital and their median survival (minimum–maximum) was 3.5 days (1–26). Upon admission, the most common diagnosis was pneumonia (table 1).
Haemodynamic and laboratory variables of survivors and non-survivors at 0 h and 4 h
After initiating ED therapies, the mean SAPS II score of the study patients at 0 h and 4 h post-presentation improved from 43 (SD 20) to 39 (SD 19) (p = 0.093). Mean arterial pressures, heart rates, body temperatures, arterial blood pH values, arterial oxygen tension (Pao2)/fractional inspired oxygen (FIo2), base deficit and serum lactate levels were significantly different for survivors and non-survivors. At 4 h post-presentation, mean arterial blood pressure and CVP in both survivors and non-survivors were significantly improved compared with 0 h values. No significant difference in lactate clearance was observed between these two groups (24.6% versus 20.9%, p = 0.547) (table 2).
Multiple logistic regression analysis using significant variables
Significant variables at 0 h and 4 h, incidence of mechanical ventilation, mean arterial pressure (MAP), heart rate, respiratory rate, body temperature, arterial pH, Pao2/FIo2, serum lactate levels and SAPS II were introduced into a backward, stepwise, logistic regression model (table 3). Base deficit was excluded from the regression analysis, because of a high correlation between arterial pH and base deficit (r = 0.842 at 0 h, r = 0.756 at 4 h). The SAPS II values and arterial pH levels were found to be independently associated with increased mortality at 0 h and 4 h post-presentation.
Relation between serum lactate level and metabolic acidosis
At 0 h and 4 h post-presentation, serum lactate levels were significantly and positively correlated with base deficit (r = 0.808, p<0.001, r = 0.704, p<0.001, respectively) and significantly and negatively correlated with arterial pH (r = −0.777, p<0.001, r = −0.666, p<0.001, respectively). Patients with a serum lactate level of 10 mmol/l or greater at both 0 h and 4 h post-presentation showed significant arterial pH depression (fig 1).

The changes in the probability of mortality and actual inhospital mortality according to serum lactate levels
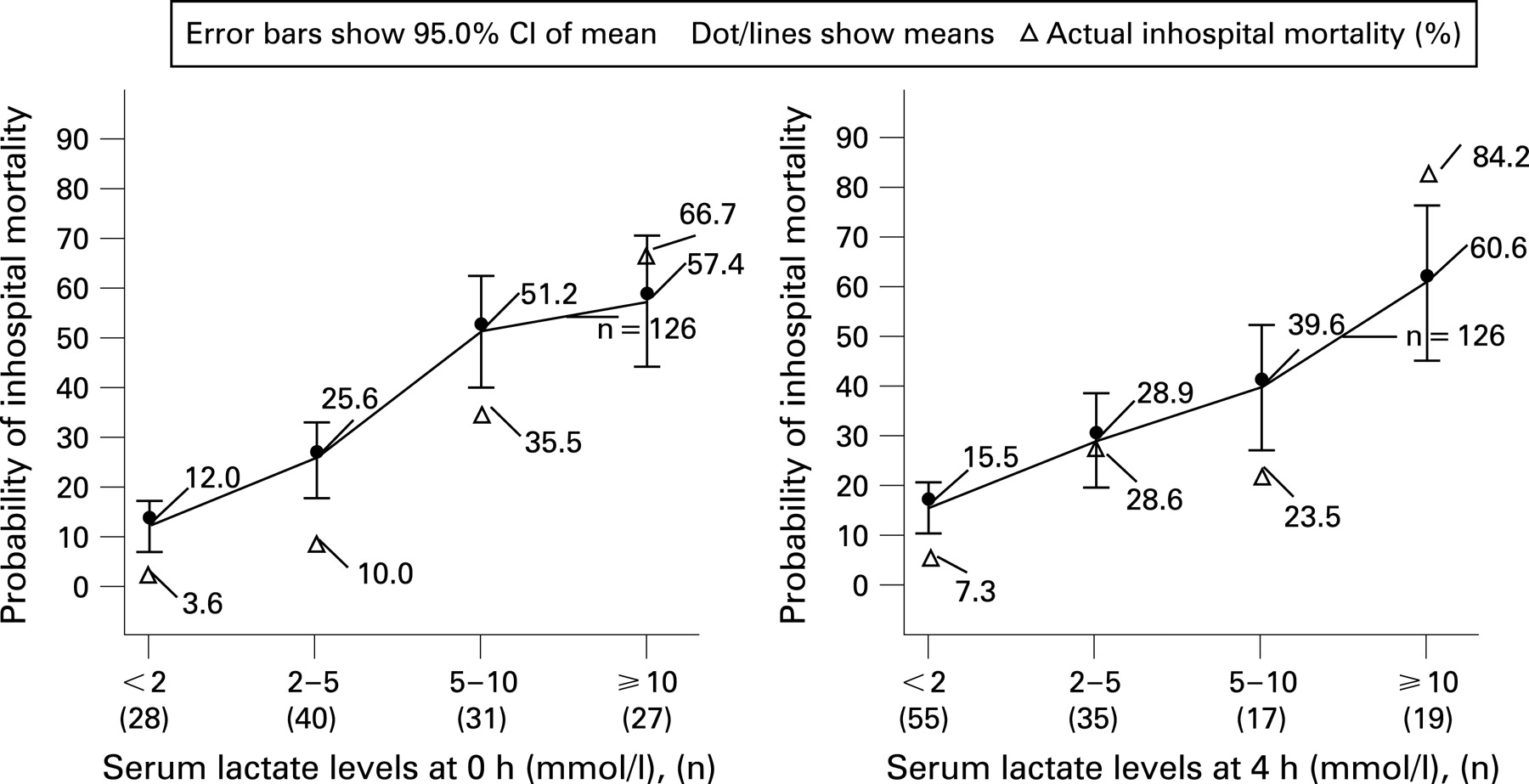
The probability of inhospital mortality and the actual inhospital mortality increased with increasing serum lactate levels as determined at both 0 h and 4 h (fig 2). At 0 h, the actual mortality of patients with a serum lactate level of less than 10 mmol/l was significantly lower than expected based on the calculated probability of mortality. Similarly, at 4 h post-presentation, the actual patient mortalities of patients with a serum lactate level of less than 2 mmol/l or from 5 to 10 mmol/l were significantly lower than expected based on calculated probabilities of mortality. At 4 h post-presentation, after emergency resuscitation, the actual inhospital mortality of patients (n = 19) who had high serum lactate levels of 10 mmol/l or greater was significantly higher than the probability of mortality. A total of 19 patients had 65 mm Hg (SD 21) of MAP, 10.2 cmH2O (SD 3.2) of CVP and 64.7% (SD 13.9) of Scvo2.
Comparison of the actual mortality and the probability of inhospital mortality according to serum lactate levels and arterial pH
At 0 h, actual mortality was lower than the probability of mortality for the normal group, mild hyperlactatemia and severe hyperlactatemia groups (fig 3). At 4 h post-presentation, the normal group and severe hyperlactatemia group had significantly low actual mortality compared with the probability of mortality. At 4 h post-presentation, patients with mild hyperlactatemia with acidosis showed a high probability of mortality and high actual mortality, and the actual mortality of patients with lactic acidosis was significantly higher compared with the probability of mortality. At 4 h post-presentation, after emergency resuscitation, the actual inhospital mortality of patients with lactic acidosis was significantly higher than the probability of mortality.

The survival curves of lactic acidosis and severe hyperlactatemia
Mean serum lactate levels (minimum–maximum) in the lactic acidosis, severe hyperlactatemia without acidosis and acidosis with normal lactate level or mild hyperlactatemia groups were 14.2 mmol/l (5.3–29.8), 7.1 mmol/l (5.0–15.8) and 2.5 mmol/l (1.9–4.8) at 0 h (p<0.001) and 13.8 mmol/l (5.1–26.2), 8.2 mmol/l (5.0–16.5) and 2.6 mmol/l (1.5–4.9) at 4 h (p<0.001), respectively (fig 4). Patients with lactic acidosis showed significantly higher inhospital mortality than normal patients at both 0 h and 4 h post-presentation. No significant differences were observed between the survival curves of patients with severe hyperlactatemia and normal–mild hyperlactatemia patients at both 0 h and 4 h.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
In our study, at both 0 h and 4 h post-presentation, SAPS II and arterial pH, rather than serum lactate, were found to be independently related to the inhospital mortality of septic emergent patients. These results are similar to those reported by Stacpoole et al,13 who found that the APACHE II score, systolic blood pressure and arterial pH at 24 h most strongly predicted mortality in patients with lactic acidosis and that lactate level did not predict survival. SAPS II reflects the physiological status such as age and chronic illness, admission type, haemodynamic status and organ dysfunction in patients.11 Multiple organ dysfunction increases mortality in patients with severe sepsis or septic shock, and haemodynamic variables, such as MAP, are associated with mortality in septic shock.14 In the present study, non-survivors showed unstable vital signs (eg, low blood pressure and a rapid heart rate), hypoxia and a high incidence of septic shock. In addition, SAPS II provides an estimate of the risk of death without having to specify a primary diagnosis.11 We thus used SAPS II as a marker of sepsis severity and as a predictor of mortality risk.
In this study, serum lactate levels were closely related to the severity of sepsis and correlated with arterial pH. Sapiro et al15 reported that the serum venous lactate level is a promising risk-stratification tool for emergency patients with infection. In addition, Trzeciak et al16 reported that an initial lactate level of 4 mmol/l or greater substantially increases the probability of acute phase death. In this study, serum lactate levels correlated well with the probability of inhospital mortality and actual inhospital mortality. However, the actual mortality of patients with a serum lactate level of less than 10 mmol/l was significantly lower than expected based on the calculated probability of mortality. Most of the patients (serum lactate levels <10 mmol/l) did not have acidosis. Hyperlactatemia without acidosis showed a relatively good prognosis compared with hyperlactatemia with acidosis. Patients with serum lactate levels of 2–5 mmol/l or 5–10 mmol/l at 4 h had similar actual inhospital mortalities despite these different serum lactate levels (fig 3), which may be explained by their similar arterial pH levels (fig 2). Hyperlactatemia may be frequently accompanied by persistently elevated endogenous catecholamines after acute stress.17
Severe tissue hypoperfusion produces much serum lactate and hydrogen ion and decreases the elimination of them from tissue, which aggravates lactic acidosis.18 In this study, patients with high serum lactate levels (⩾10 mmol/l) showed severe acidosis and their probability of mortality was high (fig 3). Persistent lactic acidosis after resuscitation may reflect uncorrected tissue perfusion. If dysfunctional tissue perfusion is not corrected, persistent tissue hypoxia may result in multiple organ dysfunction and high inhospital mortality.1 2 In this study, high serum lactate levels (⩾10 mmol/l) and lactic acidosis after emergency resuscitation showed higher actual inhospital mortality than the probability of mortality (fig 2). Indeed, they had low MAP and Scvo2. In addition, patients with lactic acidosis after initial resuscitation also showed high actual mortality compared with the probability of mortality. These results indicated that persistent lactic acidosis after initial resuscitation may reflect that persistent tissue hypoperfusion results from the inadequacy of resuscitation.
In most cases of clinically significant lactic acidosis, lactate was both over-produced and probably defectively utilised. In the present study, non-survivors had higher SAPS II scores and persistently lower Pao2/FIo2 ratios during resuscitation than survivors. It is known that hypoxia and hypoperfusion lead to reduced lactate uptake by the liver and that organ dysfunction reduces lactate clearance by the liver and kidneys.7
Mizock and Falk12 reported that the severity of lactic acidosis in critically ill patients correlates with overall oxygen debt and survival. In this study, actual mortality in patients with lactic acidosis was highest at both 0 h and 4 h. Patients who had lactic acidosis showed significant differences in the survival curve when compared with patients who had normal lactate levels and normal pH at both 0 h and 4 h post-presentation. However, there were no significant differences in survival curves between severe hyperlactatemia without acidosis and the normal group (fig 4). Although the serum lactate levels of the severe hyperlactatemia group were significantly lower than those of the lactic acidosis group, the severe hyperlactatemia group had high serum lactate levels, which were clinically significant in other studies.15 16 They did not, however, have acidosis. We thus postulate that the acid-base state of septic patients should be considered when using the serum lactate level as a predictor of outcome.
Lactic acidosis has been defined in various ways in the literature. Currently, the most accepted definition of lactic acidosis is a serum lactate level greater than 5 mmol/l and a pH less than 7.35.7 Depending on the definition used, mortality rates vary between 30% and 88%.7 In this study, the mortality rates of patients with lactic acidosis at 0 h and 4 h post-presentation were 68.6% and 78.3%, respectively.
Serial measurements of lactate and lactate clearance rates may be better predictors of mortality than a single lactate measurement.5 6 In this study, serum lactate levels improved in both survivors and non-survivors, and these two groups were not significantly different in this respect. Moreover, no significant difference in the simple lactate clearance rate was evident in these two groups. Nguyen et al6 reported that lactate clearance early during a hospital stay may indicate the resolution of global tissue hypoxia and thus a reduced risk of mortality, but no lactate clearance rate has been determined to predict a good outcome in cases of sepsis. Normalisation of serum lactate levels during the early period can only significantly predict mortality in critically ill patients.7 13
In this study, we measured haemodynamic variables at ED presentation and 4 h later. These times were chosen because the mean ED stay time for emergency patients at our institution was approximately 4 h.
This study has several limitations. First, base deficit was not included in our definition of lactic acidosis. Stacpoole et al13 defined lactic acidosis as an arterial lactate concentration of 5 mmol/l or greater and an arterial pH of less than 7.35 or a base deficit greater than 6 mmol/l, whereas we defined lactic acidosis as a serum lactate level greater than 5 mmol/l and an arterial pH of less than 7.35. Husain et al19 reported that serum lactate levels appear to be superior to corresponding base deficit levels for predicting mortality in critically ill surgical patients, and Smith et al20 found that the combination of lactate and base excess predicted mortality better than either of these two variables alone. However, we consider that these differences in the definition of lactic acidosis affect primary outcomes minimally, because of the high correlations between base deficit and arterial pH and the serum lactate level. The second limitation is that we did not have a device measuring Scvo2 continuously, but measured Scvo2 intermittently at 0 h and 4 h post-presentation using central venous blood gas analysis. We thus could not use a Scvo2 value of 4 h post-presentation as an early goal of sepsis treatment. In the present study, however, the Scvo2 value at 4 h post-presentation guided the treatment of patients in the intensive care unit.
Nevertheless, our findings indicate that bedside measurements of lactic acidosis in severe sepsis or septic shock patients may provide emergency physicians with useful prognostic information during the course of sepsis. Further studies will be needed to overcome some of the above-mentioned limitations.
In conclusion, patients who had hyperlactatemia without acidosis showed discordance between actual mortality and probable mortality. Initial lactic acidosis that includes high serum lactate levels and metabolic acidosis more precisely predicted the inhospital mortalities of severe sepsis and septic shock patients than hyperlactatemia without acidosis. Therefore, the acid-base state should be considered when attempting to predict the outcome of septic patients using serum lactate levels. Moreover, persistent lactic acidosis after emergency resuscitation showed significantly higher inhospital mortality compared with hyperlactatemia without acidosis. The measurement of both serum lactate levels and arterial pH may be a useful marker of the subsequent adequacy of resuscitation in septic emergency patients.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: The Institutional Review Board approved the study and waived the requirement for informed consent.