Article Text

Abstract
Introduction: Implementing foundation and specialty training programmes within emergency medicine raised concerns about the potential work productivity and effectiveness of new junior doctors. Between August 2006 and July 2007 senior house officers (SHO) on 6-month posts and foundation year 2 (FY2) doctors on 4-month placements worked on the same roster, rotating between the emergency department at Ninewells Hospital, a university teaching hospital in Dundee, and a smaller affiliated unit at Perth Royal Infirmary. To compare the efficiency and productivity of both groups of junior medical staff.
Methods: A prospective observational study was performed at both departments using the number of patients seen per hour as an indicator of productivity. These rates were calculated using information gathered from a computerised patient record and management system. Analysis was performed using unpaired t tests.
Results: Both groups demonstrated a significant rise in performance between the first and last month of their attachment. There was no statistical performance difference between months 4 and 6 of the SHO group, and no significant statistical difference existed between the two groups over the study period.
Conclusions: With FY2 trainees changing every 4 months, departments are potentially exposed to reduced productivity particularly in month 1. Whereas FY2 trainees have no performance difference when compared with their peers, their presence has undoubtedly impacted on middle and senior staff. Only 65% of patients attending this department are seen by junior medical staff and the vast majority of these are reviewed by senior doctors. Increasing supervision, teaching and assessments improve training, but has reduced shop floor presence and productivity.
Statistics from Altmetric.com
Postgraduate medical training and education has undergone many changes over recent years, with the implementation of foundation and specialty training programmes. These programmes have reformed postgraduate education, offering doctors focussed and modernised training, aiming to produce competent doctors and improving patient care.1 Emergency medicine has been actively involved in the implementation of these reforms.
In emergency departments (ED), concerns have been raised about the ability of junior doctors to work efficiently2 and be effective members of the team. In particular these criticisms have included:
Less experienced junior staff working on the shop floor, thereby increasing middle and senior grade workload.
Shorter ED secondments (previously 6-month attachments, now reduced to 4 months) offering less clinical learning and experience.
Shorter ED secondments reducing the productivity and effectiveness of junior doctors.
More time away from the shop floor at weekly foundation tutorials.
Organisational issues with more frequent induction programmes.
Increased supervisory and assessment requirements.
Trainees may be allocated to the ED rather than choosing to gain experience in emergency medicine and therefore may not perform optimally due to a lack of interest.
Some of these potential criticisms have been compounded with a reduction in junior doctors’ working hours to comply with regulations as laid down in the European Working Time Directive.3
The aim of this study was to compare the efficiency and productivity of junior doctors in emergency medicine on 4 or 6-month attachments.
METHODS
Ninewells Hospital in Dundee is a university teaching hospital, with a busy ED providing care for the Tayside region. A smaller affiliated department operates at Perth Royal Infirmary 25 miles away. Together, the departments see approximately 75 000 new attendances per year, with a typical case mix (66% minors, 22% majors, 11% resuscitation, 18% paediatrics and 22% admitted). Junior doctors rotate between both departments while on an emergency medicine attachment. Senior cover is provided by six full-time consultants, eight full-time registrars and one associate specialist. There is 24-h specialist registrar cover at Ninewells Hospital and consultant presence within the department between 08:00 and 00:00 hours weekdays and 08:00 until 18:00 hours at weekends. Outwith these hours, consultants are on call. Both departments have 24-h junior medical staff cover.
Between 2 August 2006 and 31 July 2007, senior house officers (SHO; 6-month posts) and foundation year 2 doctors (FY2; 4-month posts) worked on the same rota within both departments. Some of the SHO doctors had previously spent up to 6 months in emergency medicine, with general post-registration experience ranging from 1 to 3 years. We wished to compare the productivity and efficiency of the two groups to determine whether any difference existed. For investigation purposes we established the number of patients seen per hour as a measure of productivity.
A prospective, observational study was performed in both ED. The number of patients seen by individual doctors in both groups was recorded at the end of each month between 2 August 2006 and 31 July 2007. This information was obtained from a computerised patient record and management system (Symphony version 2.21.1.5; Footman–Walker Ringwood, UK). Individual doctor performance details were made anonymous to prevent potential bias by investigators. In addition, to prevent performance bias, junior doctors were unaware of the study. An average number of shop floor hours were calculated for both groups of trainees using the following formula:
Average shop floor hours = ((A.B) − (C+D))/B
where A is the number of hours per week, B is the number of weeks spent in ED, C is the number of hours spent of annual leave or study leave and D is the number of additional hours away from the shop floor, eg, protected teaching, rest breaks, assessments, etc.
For statistical analysis and comparison “hourly rates” and group mean measurements were recorded for both groups of doctors.
Results were analysed using SPSS for Windows, and Microsoft Excel 2007 and comparisons were made using unpaired t-tests. Ethics approval was not required for this study.
RESULTS
Between 1 August 2006 and 31 July 2007, junior medical staff comprised a mixture of 12 FY2 doctors (4-month attachments averaging 40.33 shop floor hours per week) and eight SHO (6 months, averaging 41.14 shop floor hours per week).
Table 1 shows the breakdown of patients seen per hour by FY2 and SHO doctors on a monthly basis. This shows a mean rise in productivity for FY2 doctors between months 1 and 4 of 0.278 patients per hour (p = 0.004; 95% CI 0.069 to 0.487). A mean rise in productivity of 0.583 patients per hour was also noted for SHO doctors between months 1 and 6 (p = 0.008; 95% CI 0.101 to 1.065).
Figure 1 illustrates the mean productivity, with confidence intervals, in both groups. The mean productivity of both FY2 and SHO doctors during months 1–4 was 1.165 patients per hour, compared with a mean of 1.391 patients per hour for SHO doctors in months 5 and 6. This demonstrated a rise of 0.226 patients per hour (p = 0.022). There was no significant difference between the number of patients seen per hour by SHO doctors at month 4 and month 6 (p = 0.265; 95% CI −0.845 to 0.119).
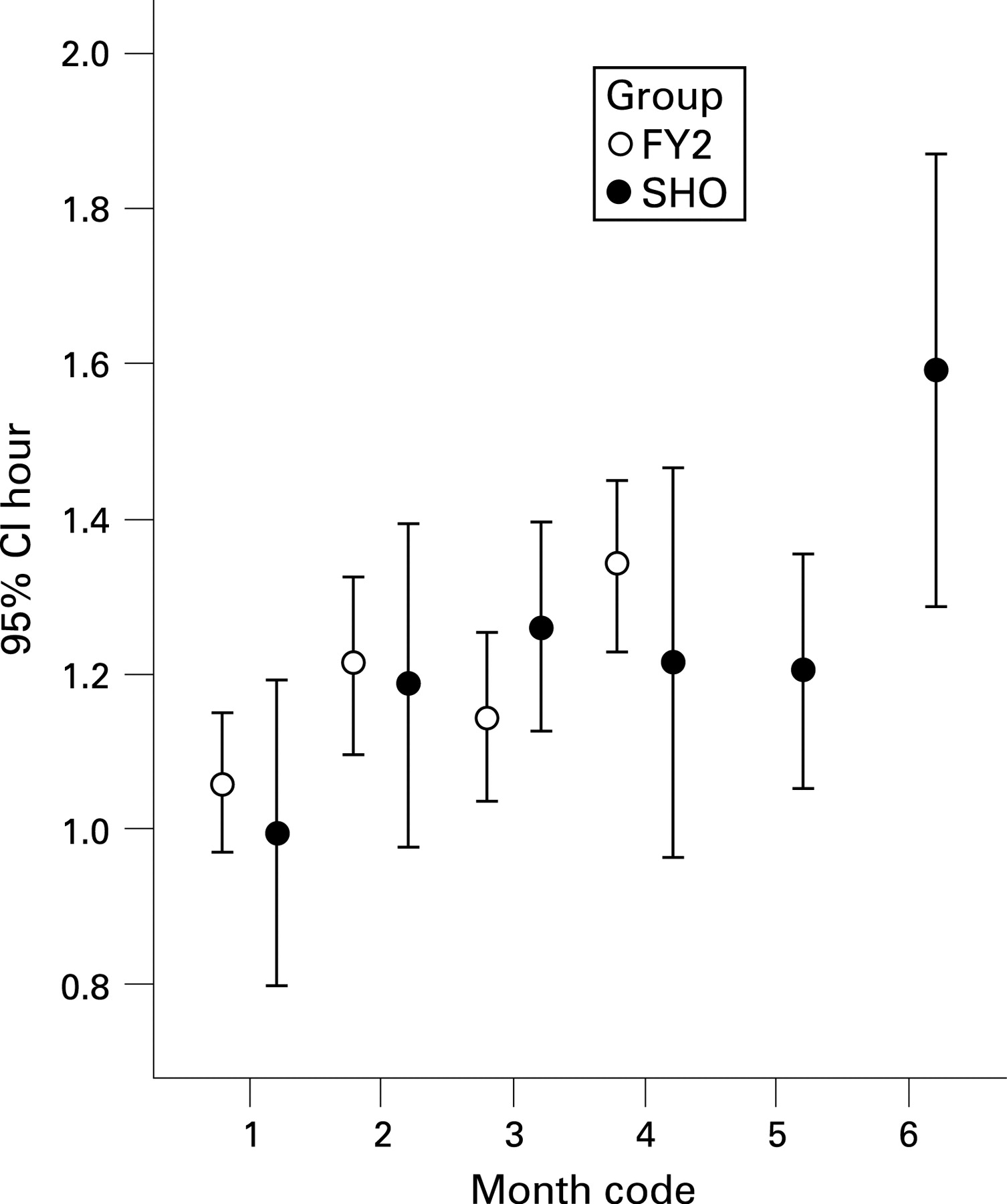
{kind=link}
Final analysis looked at the total data from each group to form a mean value of patients seen per hour for the full 12-month study period. There was no significant statistical difference in the number of patients seen per hour overall by FY2 doctors (1.19) and SHO doctors (1.24) (p = 0.289; 95% CI −0.148 to 0.044). Of the 73 352 new patients who attended the departments over this time period, 47 199 (64.35%) were seen by junior medical staff. FY2 doctors saw 27 607 (37.64%) and SHO doctors saw 19 592 (26.71%).
DISCUSSION
Modernising medical careers and the development of the foundation programme created apprehension about service provision within the ED. In addition to predictable organisational issues such as the implementation of more frequent induction programmes, increased shop floor supervision and assessment and a reduction in shop floor working time, concerns about the effectiveness of junior medical staff were raised. With the change to an apprentice-based training system, “knock on” effects to the delivery of services and ultimately patient care were anticipated.4 A study by Eager and Banks,5 however, indicated that transition to the foundation programme had no effect on the number of patients seen by junior doctors in the ED. In addition, they demonstrated that the number of patients seen by junior medical staff tailed off after month 4. Eager and Banks5 involved similar overall patient attendance figures (80 981) and identical junior doctor numbers (20) to our study, but demonstrated reduced productivity. They appeared to use the number of patients seen per month as a marker of effectiveness, which could be influenced by external factors.
Our study demonstrates significantly lower productivity in month 1 compared with month 4 in the FY2 group. This group of junior doctors changes every 4 months in the foundation programme. This potentially exposes departments to reduced productivity due to the increased frequency of induction programmes and “first month” productivity.
The doctors on 6-month rotation (SHO) similarly had a significant rise in productivity between the start and end of their attachment (month 1, month 6). Our data contradict some of the findings of Eager and Banks,5 as we did not demonstrate a fall in productivity in the final 2 months of attachment. Presumably, the improved productivity is the result of trainees demonstrating greater confidence in their clinical examination, more focussed history taking and becoming accustomed to the nature of ED working.
Analysis of the data collected over 12 months does not demonstrate any statistical difference in the number of patients seen per hour between FY2 and SHO doctors. There are more dips in productivity with FY2 doctors on 4-month attachments, but this does not impact on service provision over a full year when compared with the traditional model.
We used the number of patients seen per hour as an indicator of productivity, but accept that other performance measures exist. In addition, we recognise that a faster clinician does not necessarily provide better care.6 Speed variations will always exist between clinicians; however, by reviewing data collected over a full year and using mean values we would hope to have balanced this issue.
Croft and Mason7 recently gave several explanations for a reduction in the experience of junior doctors performing practical procedures in the ED. It is therefore reassuring to demonstrate that foundation trainees can work with the same efficiency as their peers, hopefully optimising their experience and learning opportunities. Indeed, the findings of Kilroy and Southworth8 in a UK pilot of the foundation programme indicated that there was no reduction in clinical competency associated with a 4-month rotation.
It may be beneficial to analyse the efficiency, quality of assessment and development of a treatment plan when comparing SHO and FY2 junior doctors. This could be facilitated by fully reviewing the competency of the two groups using indexed cases with expert agreed ED management, such as the acute management of a patient with a fractured neck of femur. This is certainly an area for further investigation.
The “Way ahead” document, produced in 2005 by the College of Emergency Medicine and British Association for Emergency Medicine,9 is the reference from which departments coordinate and plan manpower in the work place. The authors suggest that in a typical ED, the average SHO should see 1.5 new patients per hour, thereby seeing approximately 3000 new patient per year (1.5 multiplied by 44 shop floor hours per week, multiplied by 45 actual work weeks per year accounting for annual and study leave). They do, however, acknowledge that this might be as low as 2000 new patients per year in departments with an unusually heavy case mix. Our figures reveal that both study groups failed to achieve these expectations. An average FY2 doctor seeing 1.19 new patients per hour, and having 40.33 actual shop floor hours per week, would therefore see in the region of 2159.6 new patients per year (71.9% of the 3000 target). An average SHO doctor seeing 1.24 new patients per hour, and spending 41.14 h per week on the shop floor would see approximately 2295.5 new patients per year (76.5% of the 3000 target).
CONCLUSION
Whereas this study demonstrates that ED foundation year trainees have no difference in productivity when compared with their peers, their presence has undoubtedly had an impact on middle and senior staff. Only 65% of patients attending this department are seen by junior medical staff and the vast majority of these are reviewed by senior doctors. Increased supervision and teaching, coupled with more frequent formal assessments, may well improve training but it has reduced productivity. This must be taken into account when plans are made for future staffing provision in emergency medicine. A larger number of senior doctors will be required to deliver training, supervision and an efficient good quality service to patients.
Acknowledgments
The authors gratefully acknowledge the statistical support provided by Dr SA Ogston, University of Dundee.
Footnotes
Competing interests: None.
Contributors: PARA coordinated the study, performed data collection and interpretation and wrote the article. ALW performed data collection and interpretation and performed the literature search. ST assisted in the coordination and writing of the study and acts as guarantor.
Linked Articles
- Primary survey