Article Text

Abstract
Background In 1998 ‘Dubdoc’, Ireland's first out-of-hours general practice emergency service, opened in an outpatient suite in St James's Hospital with a separate entrance 300 m from the emergency department (ED). Dubdoc was established with the aim of providing an easy access out-of-hours service for ambulatory patients of those doctors supplying the service.
Aim To determine whether ED attendances for patients in the lower acuity triage categories 4 and 5 have changed since the establishment of ‘Dubdoc’.
Methods A retrospective review of all attendances at the ‘Dubdoc’ service was compared with attendances at the ED for triage categories 4 and 5 of the same hospital over a 9-year period (1999–2007 inclusive) for equivalent times of day.
Results ED attendances during ‘Dubdoc’ hours have decreased as a proportion of all attendances for triage categories 4 and 5. ED attendances for triage categories 4 and 5 fell substantially during the study period.
Conclusions Although the presence of the ‘Dubdoc’ service has resulted in a decrease in ED attendances for triage categories 4 and 5, this is a minor proportion of the overall decrease in attendances in this group of patients.
- Doctors in PHC
- comparative system research
- emergency care systems
- prehospital care, doctors in PHC
Statistics from Altmetric.com
Introduction
Before 1998, general practitioners (GPs) in Dublin's south inner city used a variety of different types of service to provide out-of-hours care to their patients, such as small rotas for evening and weekend cover. However, the majority of GPs used one of the commercial deputising services for some or all of their out-of-hours care. There was no out-of-hours primary care centre available in 1998. ‘Dubdoc’, Ireland's first out-of-hours cooperative service, was started that year on the St James's Hospital site in Dublin city centre as a quality initiative by local GPs, aimed at improving the care to their patients and reducing the burden on individual GPs, most of whom were in single-handed or very small group practices (2–3 doctors). The emergency department (ED) in St James's is one of the busiest in Dublin, treating in excess of 45 000 patients per annum.
Some research has shown that introducing out-of-hours primary care services can reduce ED attendances.1 A study by van Uden et al found that the creation of a primary care cooperative on the site of a hospital with an ED led to a 53% reduction in the number of emergency attendances.2 In contrast, a UK study found that the introduction of a cooperative did not affect ED attendances or patient satisfaction but did improve GP morale and job satisfaction.3 A recent Irish study also supports this finding.4 The difference in healthcare systems makes it difficult to translate such changes directly across borders. However, local studies confirm the broad acceptance of out-of-hours care by both doctors and patients in Ireland.5–8
The aim of this study was to determine whether ED attendances for patients in the lower acuity triage categories 4 and 5 have changed since the establishment of ‘Dubdoc’.
Methods
A retrospective review of all attendances at the ‘Dubdoc’ service in St James's Hospital was compared with attendances at the ED of the same hospital over a 9-year period from 1999 to 2007 inclusive.
All attendees at the ‘Dubdoc’ service are logged onto an Excel spreadsheet (Microsoft Corporation, Redmond, Washington, USA). On arrival, basic demographic details are recorded including name, age, sex, address, name of own GP and eligibility for free services or for private practice only. Clinical notes are recorded on paper. On completion of the consultation, these notes are faxed to the patient's GP during the same clinical session. The diagnosis, treatment prescribed and follow-up advice is recorded on the Excel record.9 At the end of each month, all clinical records are forwarded to the relevant participating doctor for storage. A detailed analysis of anonymised data of all the service activities is also compiled and forwarded to each participating doctor.
The basic demographic and clinical details for all patients attending the ED are entered on the ClinicomPAS system (Torex PLC, Stonesfield, Witney, Oxfordshire, UK) and monthly anonymised details are forwarded to the Hospital Quality Officer for tabulation. Attendance figures at the St James's ED were extracted by triage category from the ED electronic record system and divided by time of day to match against the opening hours of ‘Dubdoc’. The ED uses the Manchester Triage System9 to categorise patients. Nursing staff in the St James's ED act as trainers for the Manchester Triage System, both within the hospital and for other sites. The validity of triage scoring and interobserver reliability have been demonstrated on the St James's site through a series of internal validation exercises. To investigate the impact of a GP cooperative on attendances, it was necessary to include only those ED patients who might otherwise have been appropriately treated by a GP. Triage categories 1, 2 and 3 are generally held to be unsuitable for primary care, whereas categories 4 and 5 are generally considered to be treatable in a primary care setting (see table 1).10
Attendances for St James's Hospital emergency department (ED) and ‘Dubdoc’
To test if the ‘Dubdoc’ patient catchment corresponded with the St James's catchment, it was necessary to map the GPs and the hospital catchment. The hospital emergency ambulance catchment boundaries were acquired from the Health Services Executive. GP addresses were acquired from the ‘Dubdoc’ database and geocoded using the Ordnance Survey of Ireland GeoDirectory database of addresses.
The anonymised records from ‘Dubdoc’ and those from the ED, which had been extracted and collated by PKP, were analysed by CH and FOK. As there was evidence of a systematic reduction in ED attendances for patients in triage categories 4 and 5, the proportion of all triage 4 and 5 patients attending during ‘Dubdoc’ hours was used for analysis to adjust for the underlying overall decrease in attendances. The change in proportions over time was analysed using linear regression.
On attending an ED in Ireland, patients are required to make a co-payment for the cost of treatment (although certain patients are exempted on the basis of means testing). This co-payment is a fixed fee set by the Irish government. Changes in the value of the co-payment were also analysed along with changes in the demographics of the hospital catchment as potential explanations for trends in ED attendances.
Results
The map of GP practice locations and St James's Hospital catchment is shown in figure 1. With the exception of 6 of the 32 GP practices, all are located within the St James's catchment area. In figure 1, symbols for the practices are sized according to the number of registered patients who attended ‘Dubdoc’ during 2007. The outlying six practices historically feed via a major arterial route into St James's Hospital rather than to the catchment hospital for their area which lies across the river and is difficult to access by public transport. These latter practices account for 11% of patients eligible to use ‘Dubdoc’. It can be assumed that most of the remaining 89% of patients eligible to use ‘Dubdoc’ reside within the St James's catchment area and would, in the absence of an out-of-hours service, use the St James's ED in preference to other EDs. Of the 191 GPs in the St James's ED catchment, 50 participate in ‘Dubdoc’.

Locations of ‘Dubdoc’ GPs relative to the St James's Hospital catchment.
The number of attendances at ‘Dubdoc’ has been increasing year on year since the first full year of service in 1999. The number of attendances at the St James's ED for triage categories 4 and 5 has been decreasing since 1999 from 23 888 to 11 386 in 2007. While these attendances more than halved, the ‘Dubdoc’ attendances more than doubled in the same period. The absolute increase in adult attenders at ‘Dubdoc’ is greater than the absolute fall in ED attenders in triage categories 4 and 5. Attendees at Dubdoc aged ≤16 years represent approximately 36% of the workload and are not relevant to this paper, as the ED sees only those aged >14 years, with minuscule figures for those aged between 14 and 16 years.
The lower acuity triage category attendances during ‘Dubdoc’ hours have decreased as a percentage of all lower acuity triage category attendances, as can be seen in figure 2. Attendances during ‘Dubdoc’ hours have fallen by 54% compared with a fall of 52% outside ‘Dubdoc’ hours. The results of the regression analysis indicate that the decrease in proportion is statistically significant (p≤0.033, R2=0.50). The coefficient for time indicates an annual fall of 0.0021 in the proportion of patients seen during ‘Dubdoc’ hours. The number of patients seen during ‘Dubdoc’ hours in 2007 was 7% less than if the 1999 proportions still applied.
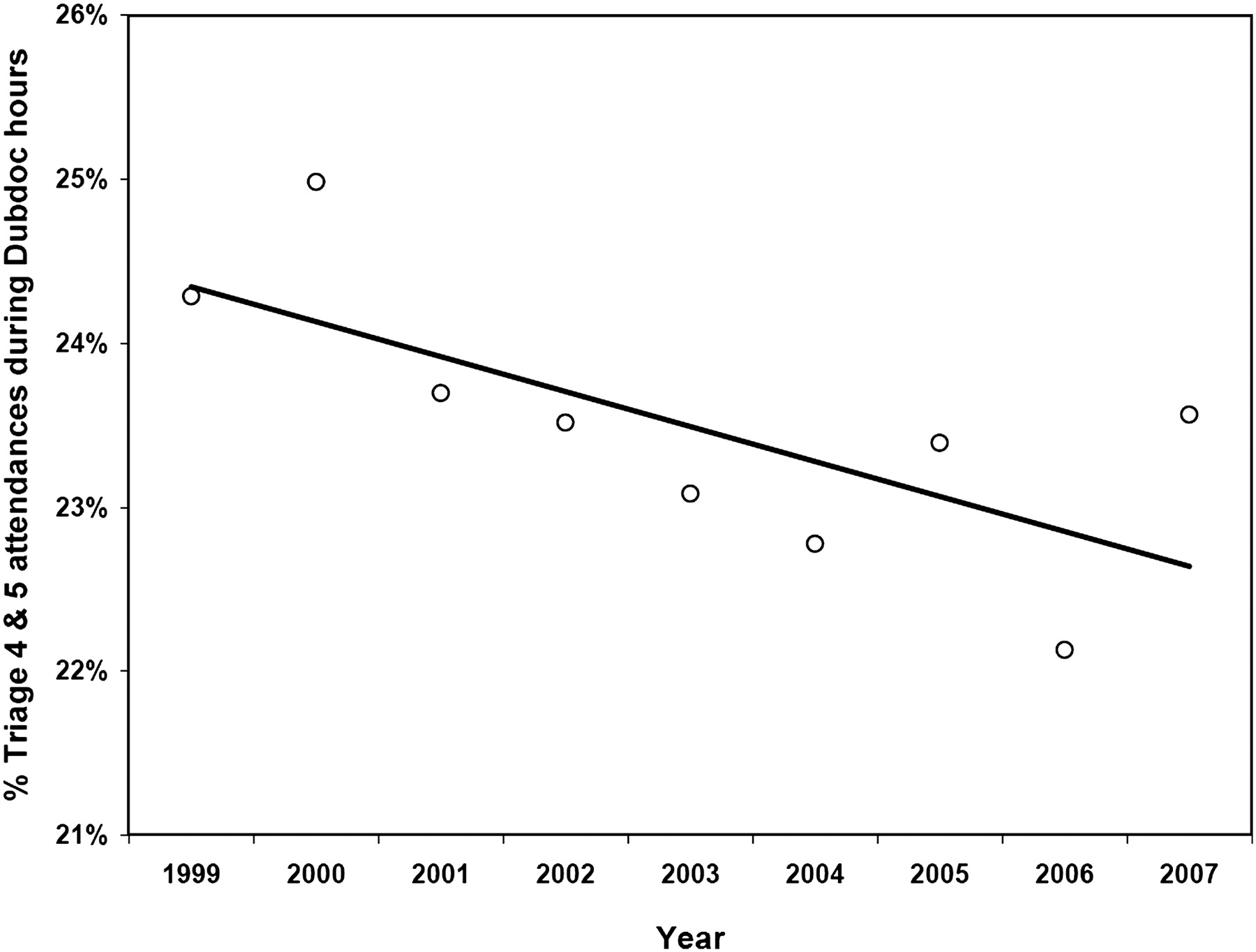
Percentage triage categories 4 and 5 attendances during ‘Dubdoc’ hours by year.
It is evident that there has been a substantial decrease in ED attendances for triage categories 4 and 5 during the study period from 23 888 in 1999 to 11 386 in 2007. Attendances for triage categories 4 and 5 have also decreased as a percentage of all ED attendances from 46% in 1999 to 24% in 2007.
To test the possibility of ‘up-triaging’ occurring, the admission percentage was used as a surrogate marker of the validity of assigned triage categories. Triage 1 had an effective admission rate of 100% during the study period when excluding mortality prior to admission. The percentage admissions for triage 2 varied between 57% and 69% with the figure stable at 62% for the last 2 years of the study period. The equivalent figures for triage 3 show that the percentage admissions range from 29% to 35% with a figure of 27% for the last 2 years of the study period. For both triage 2 and 3 the numbers of attendances have increased markedly during the study period, more than tripling for triage 2. Similarly, the percentage of admissions for triage 4 and 5 has been relatively stable over the study period. Triage 4 attendances have ranged from 2% to 5% while triage 5 admissions have been consistent at 2%. In terms of demographic changes, the population of the ED catchment increased by 10.9% in those aged ≥16 years between 1996 and 2006.
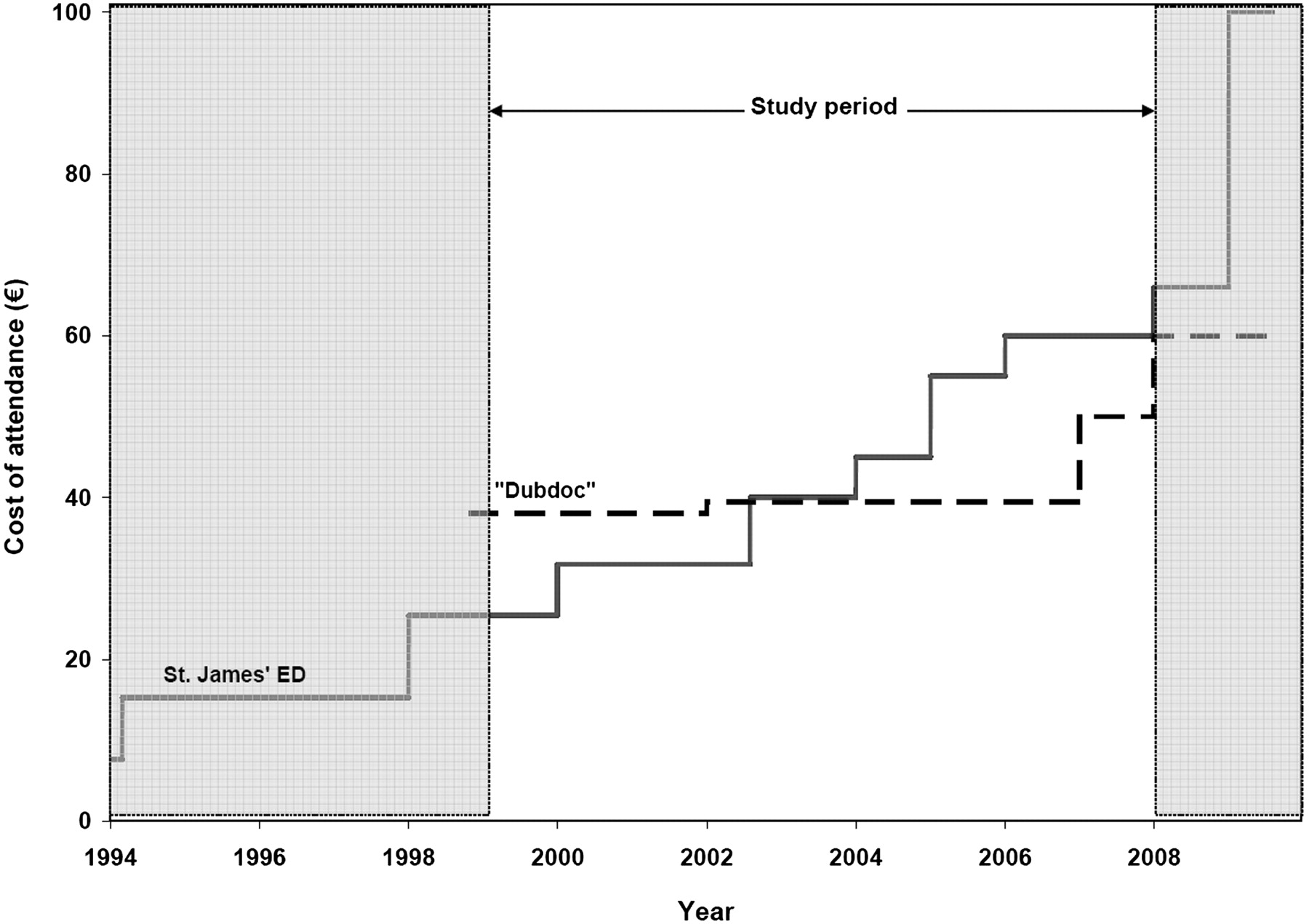
The changes in fees for attending the ED and ‘Dubdoc’ are shown in figure 3. While initially more expensive than the ED, from 2004 attendance at ‘Dubdoc’ has been less expensive than the ED.

{kind=link}
{kind=link}
{kind=link}
Fees for emergency department (ED) and ‘Dubdoc’ attendance by year.
Discussion
The statistically significant decrease in the percentage of attendances during ‘Dubdoc’ hours, coupled with the absolute figures involved, suggests that the presence of the ‘Dubdoc’ service has resulted in a minor decrease in ED attendances. However, the impact is small and, taken in the wider context of the overall decrease in triage 4 and 5 attendances, the impact does not have any substantial implications for the ED service.
The ED attendances for triage categories 4 and 5 have more than halved in the 9-year period studied. The total numbers attending the ED have been relatively stable with increased numbers attending in triage categories 1–3. The proportion of patients admitted from each triage category has remained stable, implying that there is no deviation in the process which is based on the Manchester Triage System. Richardson has previously published admission rates from the Australian Triage System, which is also a 5-stage system and is only slightly different from the Manchester Triage system used in St James's Hospital with comparable stable admission percentages.10 This implies that the reduction in attendees for triage categories 4 and 5 is genuine. The most likely reasons for the reduction are the combined impacts of increased numbers attending in triage categories 1–3, which will have a serious effect on waiting times, and the increased co-payment which acts as a financial disincentive to use the ED and should encourage greater use of GP services. ‘Dubdoc’ attendances are almost three times those for triage categories 4 and 5 in the ED at equivalent times.
Since the early 1990s, the value of co-payments for ED attendance has increased steadily, as can be seen in figure 3. The deflective impact of increased co-payment has previously been reported from this ED, although it appeared to have a lower impact at that time.11 During the study period, the cost of ED attendance increased from €25.40 to €60, representing a more than doubling of the cost. When ‘Dubdoc’ commenced, the cost of attendance was €38.10 which was significantly higher than the ED cost. At the start of 2004 the ED co-payment exceeded the ‘Dubdoc’ fee for the first time and has stayed higher ever since. The ‘Dubdoc’ fee is representative of typical GP consultation fees.10
The number of GPs involved in the ‘Dubdoc’ cooperative has been increasing over time. As only patients registered with ‘Dubdoc’ GPs can use the service, the number of potential patients has increased. This increase has been reflected in the growth in ‘Dubdoc’ attendances. The service is advertised to patients of participating doctors by notices in their clinical rooms and in the waiting rooms. Out-of-hours patients are directed to Dubdoc by an answer phone message on the telephone system of the participating doctor. ‘Dubdoc’ is not a walk-in service and patients wishing to access the service have to telephone a dedicated number and make an appointment. Appointments are always in the same session and patients are usually seen within 10–15 min of their appointed time. Patients of participating doctors who attend at the ED and are in triage categories 4 or 5 can be directed to Dubdoc by nursing staff. This accounts for about 100 referrals per year. A cap has recently been put in place as the service is operating at capacity and infrastructural constraints prevent any further expansion. ‘Dubdoc’ accounts for only a quarter of the GPs working in the St James's ED catchment area. As a result, the majority of patients in the ED catchment cannot avail of the ‘Dubdoc’ service. Given that it is a large ED with a substantial catchment population, it is perhaps not surprising that the impact of ‘Dubdoc’ is so modest. In a different setting such as a smaller ED or a greater proportion of participating GPs, the impact of the cooperative might have been more significant.
It is now 10 years since the first Irish GP out-of-hours cooperative was established. Since then, a further 12 cooperatives have been established around the country, with 1883 GPs (75% of the total) now providing service to approximately 3.7 million people. GP cooperatives are now the largest suppliers of out-of-hours GP services in the country, but not all areas are covered by these services. The advent of GP out-of-hours cooperatives has been well received by those using these services both in Ireland and elsewhere, as demonstrated by repeated satisfaction surveys.3 It is also well established that GPs' satisfaction with these services is high.7
Assessing the impact of ‘Dubdoc’ has been complicated by underlying changes in ED utilisation, particularly in the relevant triage categories 4 and 5. Without information on trends in general practice attendances, this study could not test whether or not the fall in ED attendances has been balanced by an increase in primary care attendances. It is possible that the presence of a GP cooperative generates demand for service and it may be seen as more convenient than seeking a daytime consultation for some clients. The high numbers of attendees might not be a reflection of service need but a transfer of daytime patients to an out-of-hours setting. It was not possible to determine if the proportional fall during ‘Dubdoc’ hours extended to the higher triage categories which would imply a time of day effect, although such an effect seems unlikely. A final notable limitation is that ‘Dubdoc’ is not co-located with St James's Hospital ED but rather is in close proximity. Patients are not faced with the option of entering one or other and are likely to have made a conscious decision to attend one or other service; the small number of referrals from the ED to ‘Dubdoc’ supports this view.
Previous research on primary care and emergency departments have focused on the differences between GPs and hospital doctors from the point of view of resource utilisation, cost and attitudinal issues.12–14 As the first GP cooperative service, ‘Dubdoc’ was established to enhance GP out-of-hours care for patients of participating doctors and to improve the working conditions for the participating GPs. It was not established with a view to reducing attendances at EDs. Indeed, there is no evidence that such interventions work to reduce ED attendances.15 16 Dubdoc is the only GP cooperative of the 13 that is based on hospital grounds close to an ED, and its impact on ED attendances is possibly further limited by the fact that it is not located adjacent to or within the ED. If GP cooperatives are to be presented as a potential mode to reduce ED attendances, it may be critical that they are integrated into the ED infrastructure.
Conclusions
The fact that the ‘Dubdoc’ service has had a small impact on ED attendances is a welcome if fortuitous outcome of the formation of this facility. The attendances affected are in low priority patients (from an ED perspective) who tend to have longest waiting times in the ED. This benefits patients rather than the Health Service, and should be welcomed. If medical service planners truly wish to reduce attendances and admissions in the ED, they may need to think of integrating GP-delivered out-of-hours primary care into, or more directly alongside, emergency medicine.
Acknowledgments
The authors thank Dr F X Flanagan for providing national data on GP cooperatives and Carol Hickey at St James's Hospital for kindly extracting data.
References
Footnotes
Funding CT was funded by the Health Research Board of Ireland through the HRB Centre PRIMCARE under grant 1139.
Competing interests FDO'K is a member of Dubdoc. PKP is Clinical Director in Emergency Medicine at St James's Hospital. Both were involved in the initial setting up of DubDoc.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Primary survey